孟氏骨折新分型及其指導臨床治療的療效觀察
2013-05-15 00:38:34連鴻凱黃金承張景義白玉程富禮宋相建景小博
中華肩肘外科電子雜志 2013年1期
關鍵詞:臨床療效
連鴻凱 黃金承 張景義 白玉 程富禮 宋相建 景小博
小兒骨科(張景義、白玉、程富禮、宋相建、景小博)
通訊作者:黃金承,Email:drlaohuang@163.com
【摘要】目的探討及評價新鮮兒童孟氏骨折新分型指導臨床治療的療效。方法采用前瞻性研究方法,對2007年1月至2012年12月收治的125例新鮮兒童孟氏骨折患者,采用孟氏骨折新分型標準進行分型,各分型內患者按門診號或住院號的單雙進行分組:單號為A組,患者先接受閉合手法復位進行治療,若閉合手法復位失敗則轉為手術治療;雙號為B組,患者均接受手術治療。其中,屬于新分型中Ⅰ型的患者共66例,接受閉合手法復位治療的共37例(ⅠA組),接受手術治療的共31例(ⅠB組,包括ⅠA組中2例閉合手法復位失敗者);屬于新分型中Ⅱ型的患者共55例,接受閉合手法復位治療的共26例(ⅡA組),接受手術治療的共44例(ⅡB組,包括ⅡA組中15例閉合手法復位失敗者);屬于新分型中Ⅲ型的患者共4例,接受閉合手法復位治療的共2例(ⅢA組),接受手術治療的共4例(ⅢB組,包括ⅢA組中2例閉合手法復位失敗者)。按HSS肘關節功能評分標準對各組患者治療6個月后肘關節功能的優良率進行統計分析。對于閉合手法復位失敗的患者,肘關節功能優良率視為差。結果125例患者中,9例患者失去隨訪,116例患者獲得隨訪(隨訪率92.8%),隨訪時間9~31個月(平均18.9個月),其中屬于新分型Ⅰ型的共61例,新分型Ⅱ型的共51例,新分型Ⅲ型的共4例;接受閉合手法整復的共60例,接受手術治療的共75例(包括閉合手法復位失敗的19例)。12例合并橈神經損傷的患者,在橈骨頭復位后8~12周均開始恢復。ⅠA組中優28例,良2例,可2例,差2例,優良率88.2%;ⅠB組中優25例,良2例,可2例,差0例,優良率93.1%;兩組患者優良率比較,差異無統計學意義(P=0.822)。ⅡA組中優1例,良3例,可5例,差15例,優良率16.7%;ⅡB組中優34例,良2例,可6例,差0例,優良率85.7%;兩組患者優良率比較,差異有統計學意義(P=0.000)。ⅢA組中優0例,良0例,可0例,差2例,優良率0.0%;ⅢB組中優2例,良1例,可1例,差0例,優良率75.0%;兩組患者優良率比較,差異無統計學意義(P=0.400)。結論以上尺橈關節分離程度為分型依據的新鮮兒童孟氏骨折新分型對指導臨床治療方式的選擇有較好的效果,其中屬于新分型Ⅰ型者應首選閉合手法復位治療,屬于新分型Ⅱ型及Ⅲ型者,應首選手術治療。
【關鍵詞】 孟氏骨折; 上尺橈關節分離; 新分型; 臨床療效
【Abstract】BackgroundIt is widely accepted that the closed reduction should be performed in priority in the choices of treatment for the fresh Monteggia fractures of the children. If the closed reduction failed, surgical intervention should be chosen. However, although most of the patients with the closed reduction can reach satisfactory outcomes, it is possible that the reduction may be failed and exacerbate the psychic trauma of the patients and their parents. Moreover, excessive repeated closed reduction could also make more disruption of local soft tissue around the elbow joint. Based on many years clinical observation, we introduced a new clinical classification for fresh Monteggia fracture of children, including three types:type 1 ulnar fracture with mild separation of the upper radioulnar joint and subdislocation of the humeroradial joint, type 2 ulnar fracture with severe separation of the upper radioulnar joint and complete dislocation of the humeroradial joint, and type 3 fractures of both ulnar and radius with dislocation of the radial head. We recommend closed reduction for the type Ⅰ injury, and surgical intervention for type 2 and 3 fractures.MethodsIn the present study,125 patients with acute Monteggia fractures from Jan 2007 to Dec 2012 were discussed according to the classification mentioned above. During this follow-up,9 patients were lost to follow up,116 patients were successfully followed for 9 to 31 months (mean,18.9 months). The rate of follow-up was 92.8%. In this 116 patients,49 were left elbow injuries, and 67 were right elbow injuries.Twenty patients were associated with the radial nerve injury. Their ages ranged from 1 to 14 years (mean, 4.7 years). Time since injury ranged from 1 hour to 26 hours (mean,4.2 hours).(1)Inclusion criteria:①Patients suffered from Monteggia fractures according to the new classification, aged less than 18 years;②Time since injury <3 weeks;③Fresh fracture, not treated by other hospital.(2)Exclusion criteria:①open fracture;②complicated by acute compartment syndrome which need emergency intervention;③any disease history threatening life, such as malignant tumors;④severe mental disease or disability to live himself in daily life;⑤poor in compliance or deny to participate in the trial program;⑥participated in other trial program in 1 month before the follow-up;⑦any conditions that researcher considered would influence the effectiveness or safety of the trial.All fractures were classified according to the new classification system. Then the patients were randomized into two groups based on their ID number of outpatient or inpatient. Those with odd ID number were allocated to group A, and those with even ID number were distributed into group B. Patients in group A were in the treatment of closed reduction. Operation would be performed if closed reduction failed. Patients in group B were treated by operation. Sixty-six fractures were classified as type Ⅰ. GroupⅠA had 37 patients who received closed manipulation. GroupⅠB were composed of 31 patients who received surgical operation.Fifty-five cases were classified as type Ⅱ,26 cases in group ⅡA, and 44 cases in group ⅡB. The reduction failed in 15 cases from the group ⅡA. Only four cases were classified as type Ⅲ. Two cases originally arranged in group ⅢA failed in the closed treatment, so all the 4 cases of type Ⅲ were in group ⅢB. The clinical outcomes were analyzed during the 6 months after the initial treatment. (3)Treatment Methods:①Closed Reduction Group:The deformity of the ulnar or radius was first corrected, then the dislocation of the radial head was reduced. The patient was placed in supine position, after the brachial plexus block or general anesthesia, the shoulder was abducted with the extended elbow and the supination of the forearm. Two assistants held the distal upper arm and the wrist joint, respectively. The surgeon held the ends of the fracture site, and pressed the ulnar fracture ends in the opposite direction of the angular deformation by lifting and pressing methods, which could make the angular and overlap deformity corrected. Then the surgeon pressed the radial head in the opposite direction of dislocation and reduced the radial head. The reduction was considered as successful if the raidal head did not dislocate again while the elbow was slightly flexed. For patients with both ulnar and radius fractures, the ulnar and radius overlap and angular deformity should be first corrected, and then the dislocation of the radial head was restored. The reduction could be performed twice more following the failure of the first reduction. ②Operation group:This group were treated by open reduction and internal fixation. Boyd incision was made along the posterior-lateral side of the elbow joint with a length of 10 cm. The skin, subcutaneous tissue and fascia were cut, then the ulnar and radius were visible. The fractures were anatomically reduced and fixed with plates. Then the radial head was reduced with the elbow flexed to 90 degrees. A 1.4mm Kirschner wire was inserted into the posterior elbow side along the radius canal to fix the humeroradial joint. The cast was immobilized at the elbow in the flexion of 90 degrees. The Kirschner wire was removed 6 weeks postoperatively and functional exercise began. The plates were removed 3 months postoperatively.③Management of the radial nerve injury:12 patients were combined with radial nerve injury, but were not treated by the nerve exploration. Only drugs were used to restore the nerve function. The symptoms started to recover during the 8 to 12 weeks after the restoration of the radial head.ResultsOne hundred and sixteen patients were followed up. The mean period of the follow-up was 18.9 months (range,9-31 months).Nine cases were lost to follow up. The rate of the follow-up was 92.8%.Sixty one cases from typeⅠ,51 cases from type Ⅱ and 4 cases from type Ⅲ were successfully followed up. The functional outcome was evaluated using the HSS scoring. The outcome would be regarded as bad if closed reduction failed in group A. There were no significant differences both between group ⅠA and ⅠB (P=0.822>0.05), and between group ⅢA and ⅢB (P=0.40>0.05). The difference between group ⅡA and ⅡB was statistically significant (P=0.00<0.05).DiscussionThough multiple classification systems for Monteggia fracture exist in clinical application, the Bado classification is most commonly used, which divides the Monteggia fracture into 4 types according to the direction of radial head dislocation in the imaging examination. For its neglect of the separation of the upper radioulnar joint, the Bado classification can not guide the prime clinical choice. Through the long-term clinical observation, we found that the operation would be needed because the closed reduction frequently failed in those patients with the so-called complete dislocation of the humeroradial joint, which was shown by X-ray that the distance between the radial side of the coronoid process and the medial side of the radial head was larger or equal to the width of the radial head in anteroposterior position of the elbow, or the inferior border of the radial head totally were separated with the superior border of the ulnar in lateral position. Comparatively, the mild separation of the upper radioulnar joint may be generally treated by the closed reduction. Severe separation of the upper radiounlar joint is mostly caused by high energy trauma, which could make the annular ligament totally ruptured and lose its constraint of the radial head. The ruptured annular ligament and the adjacent soft tissue would be entrapped into the joint space, which could impede the restoration of the radial head. Even the closed reduction was successfully performed, the unstable ends of the ulnar fracture site might be easily displaced after the fixation of the splint or cast. However, the patients with the mild separation of the upper radioulnar joint usually suffered the relatively lower energy trauma. In addition, the radial head epiphysis of the children were more fragile compared with their ligaments. Therefore, those radial heads were dislocated from the inferior border of the annular ligament, and the rupture of the annular ligament did not occur in most of those patients. After the correction of the greenstick fracture deformity or displacement, their radial head could always be restored to its position, and good clinical outcomes would be obtained due to their low possibility of redisplacement or redislocation.ConclusionsThe new classification method can facilitate the treatment for the Monteggia fracture. Closed reduction should be the prime choice for the type Ⅰ fracture, and operation would be recommended for the typeⅡ and Ⅲ fractures. It could obtain satisfactory clinical outcomes to choose the appropriate treatment according to the new classification system. Meanwhile, unnecessary iatrogenic injury could be avoided. Considering that the sample size of our study is limited, more observation and investigation need to be further performed.
【Keywords】 Monteggia fracture; Dislocation of the proximal radioulnar joint; New classification; Curative effect
1814年,學者Monteggia首次將尺骨上1/3骨折合并橈骨頭向前脫位的病變定義為孟氏骨折。1967年,學者Bado將孟氏骨折的概念進一步完善為:任何部位的尺骨骨折合并橈骨頭脫位。隨著對孟氏骨折研究的不斷深入,現將橈骨頭各方向脫位合并不同水平的尺骨骨折或尺、橈骨雙骨折都列入孟氏骨折的范疇。在新鮮兒童孟氏骨折治療方式的選擇上,目前公認的思路為先行閉合手法復位治療,若閉合手法復位失敗即轉為手術治療。雖然多數患者經過閉合手法復位治療能取得不錯的臨床療效,但對于閉合手法復位治療不能成功的患者而言,額外的閉合手法復位不僅增加了患者家屬及患者的心理創傷,而且對患者肘關節周圍軟組織更是一種破壞。
我們根據長期臨床觀察,以上尺橈關節分離程度為標準提出新鮮兒童孟氏骨折新分型,將新鮮兒童孟氏骨折分為三型:Ⅰ型為尺骨骨折,上尺橈關節輕度分離,肱橈關節部分脫位;Ⅱ型為尺骨骨折,上尺橈關節重度分離,肱橈關節完全脫位;Ⅲ型為尺、橈骨雙骨折,合并橈骨頭脫位。對于Ⅰ型患者,我們認為應選擇閉合手法復位治療,Ⅱ型及Ⅲ型患者應選擇手術治療。以此為指導思想,我們對鄭州市骨科醫院2007年1月至2012年12月收治的125例新鮮兒童孟氏骨折患者采用孟氏骨折新分型進行研究,旨在探討及評價該新分型對指導臨床治療的效果。
資料與方法
一、臨床資料
1.診斷標準:以橈骨頭各方向脫位合并不同水平的尺骨骨折或尺、橈骨雙骨折為標準進行診斷。
2.納入標準:(1)根據孟氏骨折診斷標準確診的孟氏骨折患者,男性或女性,年齡<18歲;(2)受傷時間<3周;(3)首診患者,未在其他醫院接受過治療。
3.排除標準:(1)開放性骨折的患者;(2)有前臂筋膜綜合征,需急診手術治療的患者;(3)有包括惡性腫瘤在內的任何嚴重威脅生命疾病史的患者;(4)有嚴重精神病史或生活不能自理的患者;(5)有對正規治療依從性差的病史,或不愿意服從試驗方案的患者;(6)在隨訪之前1個月內參與了任何其他臨床試驗的患者;(7)任何研究者認為將影響有效性或安全性結果的情況。
4.患者一般情況:采用前瞻性研究方法。以2007年1月至2012年12月收治的符合納入標準的125例新鮮兒童孟氏骨折患者為研究對象。其中,9例患者失去隨訪,116例患者獲得9~31個月的隨訪(平均18.9個月),隨訪率為92.8%。左側損傷49例,右側損傷67例;合并橈神經損傷者共12例。患者年齡1~14歲(平均年齡4.7歲),受傷時間1~26 h(平均間隔時間4.2 h),隨訪時間9~31個月(平均18.9個月)。按新鮮兒童孟氏骨折新分型標準進行分型,Ⅰ型61例,Ⅱ型51例,Ⅲ型4例。按門診號或住院號的單雙進行分組,單號先接受閉合手法復位治療,若閉合手法復位失敗則轉為手術治療(A組),雙號接受手術治療(B組)。參加研究的骨科醫師共6名,其中3名參與閉合手法復位治療,3名參與手術治療。屬于新分型中Ⅰ型的患者61例,接受閉合手法復位治療的共34例(ⅠA組),接受手術治療的共29例(ⅠB組,包括ⅠA組中2例手法復位失敗者);屬于新分型中Ⅱ型的患者共51例,接受閉合手法復位治療的共24例(ⅡA組),接受手術治療的共42例(ⅡB組,包括ⅡA組中15例閉合手法復位治療失敗者);屬于新分型中Ⅲ型的患者共4例,接受閉合手法復位治療的共2例(ⅢA組),接受手術治療的共4例(ⅢB組,包括ⅢA組中2例閉合手法復位治療失敗者)。各分組內A、B兩組患者年齡、受傷時間、平均隨訪時間等臨床資料比較,差異無統計學意義,具有可比性,見表1。
表1 新鮮兒童孟氏骨折患者一般臨床資料
二、治療方案
1.閉合手法復位組(圖1):采用閉合手法復位進行治療。根據先糾正尺骨或橈骨骨折畸形,再整復橈骨頭脫位的原則進行復位[1]。選擇臂叢麻醉或全麻,患者仰臥位,肩外展,在肘關節伸直、前臂旋后位體位下,兩助手分別緊握患肢上臂下段及患肢手腕部做對抗牽引,術者雙手分別握住骨折斷端兩側,通過提按手法,用與尺骨骨折斷端間成角方向相反的力按壓尺骨兩斷端,糾正尺骨斷端間成角及重疊畸形。然后,術者雙手拇指用與橈骨頭脫位方向相反的力按壓橈骨頭,使橈骨頭復位。復位結束后,輕微屈伸肘,若橈骨頭不再脫位,則說明復位成功。對于尺、橈骨雙骨折的患者,術者先糾正尺、橈骨重疊、成角、旋轉移位,再整復橈骨頭脫位。對于一次手法復位失敗者,可再行手法復位,但不超過3次。
復位成功后,用石膏托將肘關節固定在屈曲90 °,前臂中立位,于尺骨斷端及橈骨頭脫位處放置襯墊,以防止骨折移位及橈骨頭再脫位,觀察末梢血液循環及感覺。第5、14天拍X線片復查,若有移位等情況,及時調整。8例患者在第5天X線片復查時,見尺骨骨折移位,經再次整復后糾正。石膏托固定6~8周,直至骨折脫位臨床愈合。
2.手術治療組(圖2):采用切開復位內固定進行治療。沿肘后外側Boyd切口,長10 cm,切開皮膚、皮下組織、筋膜,顯露尺骨、橈骨,解剖復位尺(橈)骨骨折斷端,鋼板進行內固定;復位橈骨頭,屈肘90 °,取一根直徑1.4 mm的克氏針,由肘后進入,沿橈骨髓腔貫穿固定肱橈關節,折彎、剪斷鋼針,尾部埋于皮下。術后前臂中立位屈肘90 °石膏托固定,術后6周拔出克氏針拆除石膏行肘關節主動功能鍛煉,術后3個月拆除鋼板。

圖1 患兒男性,5歲,右肘外傷6 h,診斷為右孟氏骨折,新分型Ⅰ型,行手法閉合復位治療。A、B圖示治療前肘關節X線正、側位圖像,顯示橈骨頭向前側脫位,上尺橈關節輕度分離,肱橈關節部分脫位;C、D圖示閉合手法整復后肘關節X線正、側位圖像,顯示尺骨斷端復位,橈骨頭復位;E、F圖示閉合手法整復4周后復查肘關節X線正、側位圖像,顯示尺骨斷端對位、橈骨頭復位尚可;G、H圖示手法整復8周后復查肘關節X線正、側位圖像,顯示尺骨斷端愈合,橈骨頭位置尚可

圖2 患兒女性,7歲,右肘外傷14 h,診斷為右孟氏骨折,新分型Ⅱ型,先行閉合手法復位石膏外固定治療,治療失敗后轉為手術治療。A、B圖示手法整復前肘關節X線正、側位圖像,顯片示橈骨頭向前側脫位,上尺橈關節重度分離,肱橈關節完全脫位;C、D圖示手法整復后肘關節X線正、側位圖像,顯示尺骨斷端復位欠佳,橈骨頭仍脫位;E、F圖示術后X線正、側位圖像,顯示橈骨頭復位,肱橈關節行克氏針固定,尺骨截骨行鋼板內固定;G、H圖示術后3個月取出內固定后X線正、側位圖像,顯示尺骨愈合良好,橈骨頭復位良好
3.橈神經損傷的處理:本次研究中,共12例患者治療前存在橈神經損傷癥狀,我們均未做神經探查術,常規給予促進神經損傷恢復的藥物1~2個療程,在橈骨頭復位后的8~12周內,橈神經損傷癥狀均開始恢復。
三、統計學處理方法

結 果
116例患者獲得隨訪(隨訪率92.8%),其中屬于新分型Ⅰ型的共61例,新分型Ⅱ型的共51例,新分型Ⅲ型的共4例,接受閉合手法整復的有60例,接受手術治療的有75例(包括閉合手法復位失敗的19例)。隨訪時間9~31個月(平均18.9個月)。12例合并橈神經損傷的患者,在橈骨頭復位后8~12周均開始恢復。治療6個月后,按HSS肘關節功能評分標準[2]對患者肘關節功能的優良率進行評價,閉合手法復位失敗者,肘關節功能優良率視為差。ⅠA組中優28例,良2例,可2例,差2例,優良率88.2%;ⅠB組中優25例,良2例,可2例,差0例,優良率93.1%;兩組患者優良率比較,差異無統計學意義(P=0.822)。ⅡA組中優1例,良3例,可5例,差15例,優良率16.7%;ⅡB組中優34例,良2例,可6例,差0例,優良率85.7%;兩組患者優良率比較,差異有統計學意義(P=0.000)。ⅢA組中優0例,良0例,可0例,差2例,優良率0%;ⅢB組中優2例,良1例,可1例,差0例,優良率75%;兩組患者優良率比較,差異無統計學意義(P=0.400)。見表2。
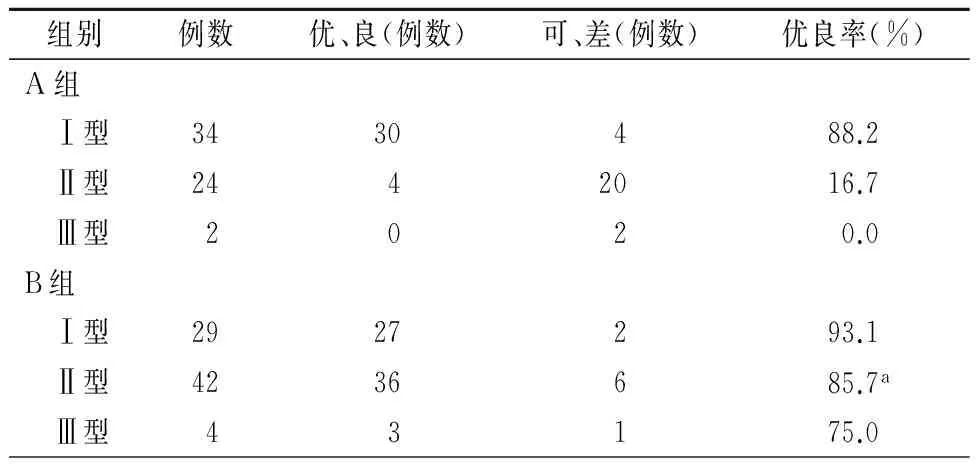
表2 新鮮兒童孟氏骨折患者治療6個月后肘關節功能優良率的比較
注:與ⅡA組比較,aP=0.000
討 論
一、Bado分型指導下新鮮兒童孟氏骨折的治療現狀
雖然目前臨床上存在多種孟氏骨折分型系統,但最常用的仍是Bado分型[3],該分型從影像學上以橈骨頭脫位方向作為分型依據將孟氏骨折分為四型,但其忽略了上尺橈關節的分離程度,進而未能指導臨床中首選閉合手法復位治療或是手術治療。國外學者Givon等[4]通過臨床觀察發現Bado分型能在新鮮兒童孟氏骨折閉合手法復位中指導手法復位方向的選擇,但Bado分型與患者預后之間的關系不具有統計學意義。國內學者朱付平等[5]回顧性研究了先行手法復位治療的66例新鮮兒童孟氏骨折的臨床資料,結果手法復位獲得成功者28例,其余38例患者均遭受不必要的手法整復。李明等[6]通過對50例行閉合手法復位治療的新鮮兒童孟氏骨折的回顧性研究發現,20例患者獲得閉合手法復位成功,30例閉合手法復位失敗。我們認為Bado分型僅考慮了橈骨頭脫位的方向,忽略了上尺橈關節分離的程度,不能指導臨床選擇合適的治療方式,使臨床治療中出現先采用閉合復位治療,若閉合復位失敗,再采用手術治療的現象,增加了部分患者的痛苦。因此,我們提出了以上尺橈關節分離的程度為標準的新分型,并根據新分型指導臨床治療方式的選擇。
我們通過長期臨床觀察發現,在肘關節X線正位片中,在尺骨冠狀突高度橈側緣與橈骨頭內側緣間距≥1個橈骨頭寬度,或在側位片上,橈骨頭下緣與尺骨上緣完全分離,即肱橈關節完全脫位時,手法復位多不能獲得成功,需行手術治療,我們稱之為上尺橈關節重度分離。而當肘關節X線正側位片不滿足以上條件,肱橈關節部分脫位時,手法復位多能獲得成功,我們稱之為上尺橈關節輕度分離。
二、新分型的理論依據
上尺橈關節為車軸關節,由尺骨橈側切跡及橈骨頭柱狀唇組成,并由環狀韌帶、方形韌帶、肘關節內外側副韌帶進行加強[7]。Abdelgawad等[8]認為上尺橈關節的穩定由肘關節囊、環狀韌帶和骨間膜3個因素共同維持,在前臂旋前至70 °及旋后至80 °左右時,斜索及骨間膜上部、骨間膜中下部纖維分別出現緊張,限制前臂過度旋前、旋后,防止上尺橈關節脫位。我們通過對部分患者行患側前臂MRI檢查發現,尺骨斷端間移位明顯的患者,前臂骨間膜多出現大范圍撕裂傷或斷裂,上尺橈關節出現重度分離,肱橈關節完全脫位;而對于尺骨青枝骨折或斷端移位不明顯的患者,前臂骨間膜多為小范圍撕裂傷,上尺橈關節出現輕度分離,肱橈關節部分脫位。許營民等[9]通過觀察發現,在前臂受到較小暴力時,環狀韌帶不發生完全斷裂,部分覆蓋于橈骨頭邊緣,似“歪戴帽”樣嵌頓在肱橈關節之間,在尺骨畸形獲得糾正后,手法整復可使橈骨頭獲得復位;而當前臂受到較強暴力時,環狀韌帶則出現完全斷裂,并嵌頓于上尺橈關節之間,肱橈關節完全脫位,手法不能將橈骨頭復位。對于閉合復位失敗的新鮮孟氏骨折患者,我們在術中發現橈骨頭脫位在關節囊外,甚至穿破關節囊,環狀韌帶完全斷裂,上尺橈關節內嵌頓有環狀韌帶及關節囊周圍軟組織,即使直視下將橈骨頭復位,在活動肘關節時,橈骨頭易現再次脫位,保守治療不能成功。而這種變化也恰能解釋部分患者在接受閉合手法整復后,雖然X線提示橈骨頭獲得復位,但復查時,橈骨頭又再次出現脫位的現象。
我們認為伴上尺橈關節重度分離的患者,多由于遭受較強暴力,使環狀韌帶完全破裂,失去對橈骨頭的約束,斷裂的環狀韌帶及肘關節周圍軟組織嵌頓于上尺橈關節內,阻礙橈骨頭的復位,使閉合手法復位困難,即使手法整復獲得成功,由于尺骨斷端間不穩定,行石膏或夾板外固定后,尺骨斷端間也極易發生移位,易引起橈骨頭再脫位,故應選擇手術治療。而上尺橈關節輕度分離的患者,由于遭受暴力較輕,加上兒童橈骨頭骨骺比韌帶脆弱,在外力作用下,橈骨頭從環狀韌帶下緣脫出,多數患者并不伴有環狀韌帶斷裂,在糾正尺骨青枝骨折畸形或骨折斷端間輕度移位后,整復橈骨頭,多能獲得橈骨頭復位,行石膏或小夾板固定后,尺骨斷端間發生再移位及橈骨頭再脫位的可能性也較低,因此能獲得不錯的臨床療效。
對于尺、橈骨雙骨折合并橈骨頭脫位的患者,由于尺、橈骨同時骨折,斷端間失去支撐,橈骨近端呈現漂浮改變,使閉合復位困難,即使閉合復位獲得成功,也極易出現斷端再移位及橈骨頭再脫位,加上兒童不配合治療,更不利于復位后穩定性的維持。
三、新分型的臨床意義
通過本次前瞻性研究,我們按新分型標準對符合納入條件的125例患者的病例進行了研究,共116例患者獲得隨訪,根據HSS肘關節功能評分標準[2]評價患者治療后6個月肘關節的優良率,發現對于上尺橈關節輕度分離者,閉合手法復位治療與手術治療的優良率差異不具有統計學意義,而閉合手法復位治療不僅可減少手術對患者的創傷,而且能降低患者的醫療開支,因此,對于新分型中的Ⅰ型患者,我們認為應首選閉合手法復位進行治療。對于上尺橈關節重度分離的患者,手術治療組的優良率明顯高于閉合手法復位組的優良率,因此,對于新分型中的Ⅱ型患者,我們認為應首選手術治療,以減少不必要的閉合手法復位給患者帶來的額外傷害。對于尺、橈骨雙骨折合并橈骨頭脫位的患者,2例閉合復位患者治療療效均為差,手術治療的4例患者,3例療效優,1例療效良,閉合手法復位治療組的優良率與手術治療組的優良率差異不具有統計學意義。我們認為對于尺、橈骨雙骨折患者,由于存在雙骨折,尺骨及橈骨失去對方的支持,極不穩定,閉合手法復位不易獲得成功,即使復位成功,也極易再次移位,因此應首選手術治療。
總之,在孟氏骨折新分型指導下選擇合適的治療方式,不僅能使患者獲得滿意的臨床療效,而且可使患者免遭不必要的醫源性創傷。但目前我們仍存在樣本量較小的問題,仍需要進一步研究和觀察。
參 考 文 獻
[1] Agarwal A.Type Ⅳ Monteggia fracture in a child[J].Can J Surg,2008,51(2):E44-E45.
[2] Figgie MP, Inglis AE, Mow CS, et al. Results of Reconstruction for failed total elbow arthroplasty[J]. Clin Orthop Relat Res,1990(253):123-132.
[3] Wenger DR,Pring ME.Rang小兒骨折[M].潘少川,譯.3版. 北京:人民衛生出版社,2006:112-115.
[4] Givon U, Pritsch M, Levy O, et al.Monteggia and equivalent lesions:a study of 41 cases[J].Clin Orthop Relat Res,1997 (337):208-215.
[5] 朱付平,熊光仲,王萬春,等.新鮮兒童孟氏骨折治療方法的選擇[J].中國骨與關節損傷雜志,2006,21(7):518-520.
[6] 李明,張德文,劉正全,等.兒童孟氏骨折的治療[J].中華骨科雜志,2004,24(6):342-345.
[7] 王亦璁.骨與關節損傷[M].4版.北京:人民衛生出版社,2007:887.
[8] Abdelgawad AA, Hussain A, Ebraheim NA. Screw fixation of the radial head:radiological assessment of the proximal radio-ulnar joint and average radial head diameter-an anatomic study[J]. Arch Orthop Trauma Surg,2010,130(4):465-467.
[9] 許營民,崔青,劉志波. 小兒孟氏骨折中環狀韌帶的損傷分類探討[J].中國矯形外科雜志,2000,7(2):119.
猜你喜歡
今日健康(2016年12期)2016-11-17 12:55:34
今日健康(2016年12期)2016-11-17 11:53:45
今日健康(2016年12期)2016-11-17 11:36:14
中國實用醫藥(2016年24期)2016-10-17 05:48:31
中國實用醫藥(2016年24期)2016-10-17 05:36:56
中國實用醫藥(2016年24期)2016-10-17 05:23:44
中國實用醫藥(2016年24期)2016-10-17 05:00:41
中國實用醫藥(2016年24期)2016-10-17 04:59:50
中國實用醫藥(2016年24期)2016-10-17 04:47:30
中國實用醫藥(2016年24期)2016-10-17 04:29:05