肩袖損傷MRI與關(guān)節(jié)鏡下表現(xiàn)對比的初步研究
2013-05-15 00:36:57劉佳超陳建海黃偉王天兵姜保國
中華肩肘外科電子雜志 2013年1期
劉佳超 陳建海 黃偉 王天兵 姜保國
通訊作者:姜保國,Email:jiangbaoguo@vip.sina.com
【摘要】目的研究MRI對肩袖損傷診斷的準確性和關(guān)節(jié)鏡檢查肩袖損傷的適應(yīng)證。方法回顧性分析2007年7月至2010年12月北京大學人民醫(yī)院創(chuàng)傷骨科行關(guān)節(jié)鏡檢查或治療患者的59例肩部疾病患者,將MRI表現(xiàn)與關(guān)節(jié)鏡檢查所見進行對照分析。結(jié)果59例患者中,術(shù)前MRI檢查明確診斷肩袖損傷36例;經(jīng)關(guān)節(jié)鏡檢查證實肩袖撕裂35例,未見明顯撕裂者1例。術(shù)前MRI檢查未發(fā)現(xiàn)肩袖撕裂而關(guān)節(jié)鏡下見撕裂7例,MRI檢查與關(guān)節(jié)鏡下均未見肩袖撕裂者16例。MRI對肩袖損傷診斷的敏感性為88.3%,特異性為94.1%,陽性預(yù)測值97.2%,陰性預(yù)測值69.6%,準確性86.4%。結(jié)論MRI是診斷肩袖損傷的有效輔助檢查手段,但仍存在一定程度的漏診情況;關(guān)節(jié)鏡檢查是診斷肩袖損傷最為可靠的輔助檢查手段。
【關(guān)鍵詞】 肩關(guān)節(jié); 肩袖; 關(guān)節(jié)鏡
【Abstract】BackgroundRotator cuff, a sleeve-like structure composed of supraspinatus, infraspinatus muscle, teres minor and subscapularis, is the major anatomical structure to maintain shoulder stability. Rotator cuff pathologies are frequently encountered in patients with pain at the shoulder. The rotator cuff can be visualized with different imaging techniques such as ultrasonography (US), arthrography, arthroscopy, computed tomography (CT) and magnetic resonance imaging (MRI). MRI had quickly become the favored method for preoperative diagnosis of the rotator cuff injury, with high soft tissue resolution ratio, sensitivity and accuracy. It is clinically significant to correctly understand the MRI manifestation of patients with the painful shoulder. We retrospectively analyzed the MRI examination and arthroscopy findings of 59 rotator cuff injuries treated in one hospital.Methods(1)Subjects:From July 2007 to December 2010, a total of 59 patients (25 males and 34 females, aged from 24 to 83 years old, mean age 54.33 years), who underwent arthroscopic surgery for their shoulder joint diseases, were selected. All the patients had shouder MRI examination before operation, we compared their preoperative MRI results with surgical findings.(2)Arthroscopic surgery:All arthroscopic surgical procedures were performed by experienced directors or deputy directors of physicians to obtain an accurate diagnosis of the rotator cuff injury. All patients were treated by Stryker (Stryker) arthroscopic systems for their diagnosis and treatment. Diagnosis was based on the surgical records or video records.(3)Magnetic resonance imaging:Multi-planar MR imaging of the shoulder was performed using coronal oblique, sagittal oblique and axial sequences. All MRIs were reported by a radiologist with special trained in musculoskeletal imaging. (4)Diagnosis of rotator cuff injury:Based on the lannotti classification criterion, according to their pathological changes, rotator cuff injuries can be classified as ① Tendinitis:increased tendon signal intensity, no morphological changes, and intact shoulder-deltoid bursa fat layer. ②Partial-thickness tear:the increased limitations of signal intensity at the tendon, morphological changes accompanied by the discontinuity of the shoulder-deltoid bursa fat layer. ③ Full thickness tear:the significantly increased tendon signal intensity, obvious morphological abnormalities such as discontinuity of the tendon, tendon-muscle belly retraction or obvious muscle atrophy, ie the increased signal intensity of the muscles, the discontinuity or disappearance of the acromion-the deltoid bursa fat layer.ResultsThirty-six out of 59 cases were diagnosed as the rotator cuff injury by MRI before operation,35 of which had been confirmed with tendinitis, partial-thickness tear or full thickness tear by arthroscopy during operation. One rotator cuff injury diagnosed before operation was proved to be intact arthroscopically. Seven cases with negative findings under MRI examination had been found to be rotator cuff injuries by arthroscopy. 16 cases (including fractures, shoulder instability or Bankart injury) of them presented intact in both MRI examination and arthroscopy operation. The sensitivity level of MRI examination for the rotator cuff injuries was 83.3%. The specificity level of MRI examination was 94.1%.The accuracy was 86.4%.The degree of positive prediction was 97.2%, and that of negative prediction was 69.6%. These rotator cuff injuries included 3 cases of tendinitis,13 cases of partial-thickness tear (10 of bursa side and 3 of articular side) and 22 cases of full-thickness tear.DiscussionPatients with rotator cuff injury are frequently encountered. As a hub of upper limb activities, rotator cuff determines the range of the shoulder activitivy and space accuracy. The rotator cuff muscles are main strength source of the shoulder, which play a vital role in the shoulder function. Therefore, rotator cuff injuries at the shoulder would produce different degrees of dysfunction and painfulness, and seriously affect the patient′s quality of life and activities of daily living.Firstly, we need to define that the rotator cuff injury is a partial-thickness tear or a full-thickness tear. Ellman divided the partial-thickness rotator cuff tears into three categories:synovial side partial-thickness tear,intra-tendon partial-thickness tear and articular side partial-thickness tear. Each category is divided into three degrees according to the depth of tear:degree Ⅰ (<3 mm),degree Ⅱ (3-6 mm),degrees Ⅲ (>6 mm), or more than 50% of the full-thickness at the tendon. Full-thickness tear classification is generally based on the size of tear:small tear (<1 cm), medium tear (1-3 cm), large tear (3-5 cm) and a massive tear (>5 cm).The imaging examination on the shoulder is indispensable in the diagnosis and classification of rotator cuff injuries, in addition to their detailed medical history and physical examination. The non-invasive and non-radioactive MRI, with excellent anatomy repeatability and organizational control comparability, can provide multi-angle, multi-plane and multi-level scan imaging, presenting a variety of normal and abnormal tissue structure imaging, which seems to be very important for the diagnose of shoulder diseases. In our study, the sensitivity level of MRI in diagnosis of the rotator cuff injury is 83.3%. Seven cases which were negatively diagnosed in MRI examination had been proved to be rotator cuff injuries by arthroscopy.Using arthroscopy, we can observe the rotator cuff directly to identify the scope, size, and shape of tears. And the shoulder joint synovitis, supraspinatus tendon degeneration and partial tears of the biceps tendon and other pathological changes can be also determined by arthroscopy, which can′t be comparable with other imaging techniques. Therefore, it is necessary to use arthroscopy for the patients who have long-term shoulder pain, functional limitation, long-term conservative treatment fails and other tests difficult to diagnose. Arthroscopy can provide not only the confirmation of the diagnosis, but also the treatment such as debridement of the shoulder joint synovial tissue and calcification of supraspinatus tendon and suture of the teared rotator cuff.ConclusionsAccording to our research and literature, generally speaking, MRI examination plays an important role for the diagnosis of rotator cuff injuries, which can provide the accurate determination of the extent, size and scope of rotator cuff injuries, as well as the signs associated. MRI can facilitate the development of treatment programs for the rotator cuff injuries, and eventually help patients to get timely and correct treatment.
【Keywords】 Shoulder; Rotator cuff; Arthroscopy
肩袖是由岡上肌、岡下肌、小圓肌及肩胛下肌的肌腱構(gòu)成的包裹肱骨頭的袖套樣結(jié)構(gòu),是維持肩關(guān)節(jié)穩(wěn)定的主要解剖結(jié)構(gòu)。肩袖損傷是臨床較為常見的引起肩關(guān)節(jié)疼痛的疾病,多為撕裂傷,大部分需行手術(shù)治療,術(shù)前明確診斷對手術(shù)適應(yīng)證及手術(shù)方案的制定都有重要意義。用于肩部影像學診斷方法有X線片、肩關(guān)節(jié)造影、肩關(guān)節(jié)CT及MRI。MRI以其對軟組織的高分辨率、對損傷的高敏感性和特異性等特點已成為肩關(guān)節(jié)檢查的首先考慮的影像學檢查[1-3]。對有臨床癥狀患者的MRI表現(xiàn)的正確理解無疑對肩關(guān)節(jié)鏡診療有重要意義和價值,我們對北京大學人民醫(yī)院創(chuàng)傷骨科59例肩關(guān)節(jié)鏡檢查患者的MRI資料進行回顧分析,旨在探討MRI與肩關(guān)節(jié)鏡診斷的準確性。
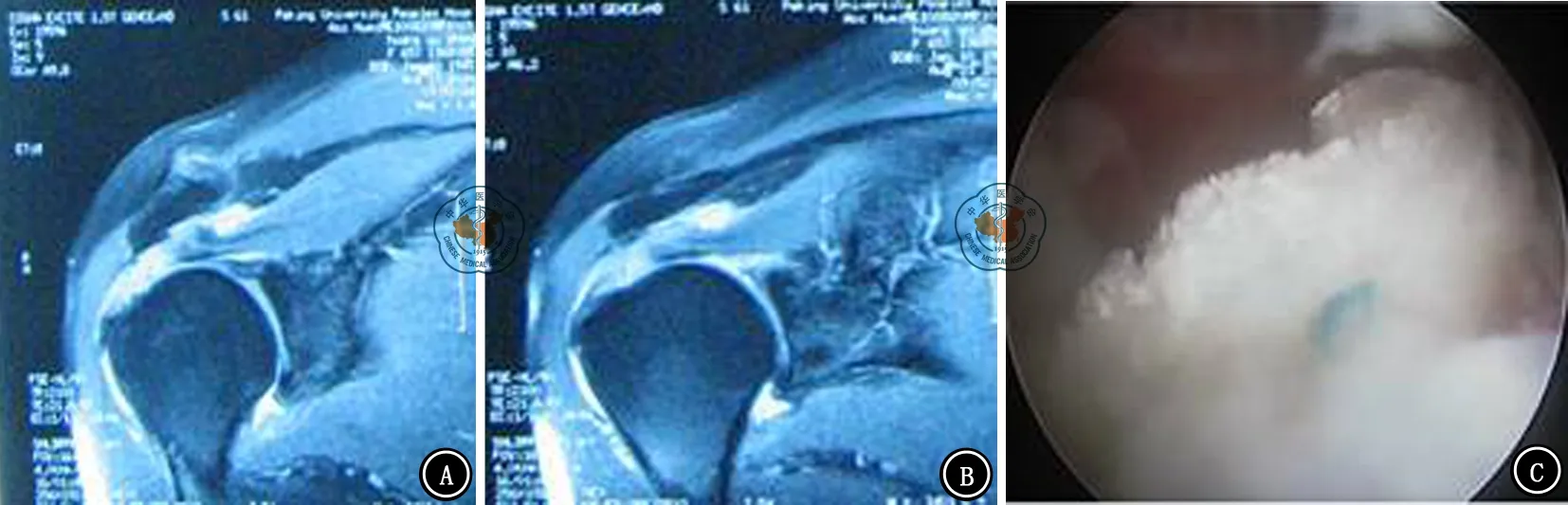
圖1 岡上肌腱全層撕裂MRI和關(guān)節(jié)鏡檢查圖像。A、B圖示全層撕裂MRI表現(xiàn);C圖示全層撕裂關(guān)節(jié)鏡下表現(xiàn)
材料和方法
一、一般資料
收集2007年7月至2010年12月59例因肩關(guān)節(jié)疾病而行肩關(guān)節(jié)鏡檢查或治療患者的MRI和手術(shù)資料。其中男性25例,女性34例;年齡24~83歲,平均56歲。患者均因肩關(guān)節(jié)疼痛就診,并入院行關(guān)節(jié)鏡檢查或治療。經(jīng)關(guān)節(jié)鏡檢查證實,肩袖損傷42例,其他肩部疾病17例。對59例肩關(guān)節(jié)的MRI表現(xiàn)和關(guān)節(jié)鏡手術(shù)記錄資料與影像進行對照分析。
二、關(guān)節(jié)鏡診療技術(shù)
所有病例均使用史賽克(Stryker)關(guān)節(jié)鏡系統(tǒng)進行診療。關(guān)節(jié)鏡手術(shù)操作由經(jīng)驗豐富的主任醫(yī)師或副主任醫(yī)師進行,以獲得肩袖撕裂的準確診斷。手術(shù)情況以手術(shù)記錄及影像記錄為準。
三、MRI技術(shù)及掃描位置
采用GE公司四肢關(guān)節(jié)專用掃描系統(tǒng),常規(guī)取橫軸位、斜冠狀位、斜矢狀位。
四、肩袖損傷的診斷
參考Lannotti等[4]分類方法,根據(jù)病理改變特征分類。(1)肌腱炎:肌腱信號強度均勻性增加,但無形態(tài)學改變,肩峰-三角肌下滑囊脂肪層完整;(2)不全斷裂:肌腱信號強度局限性增加,形態(tài)也發(fā)生改變,并伴有肩峰-三角肌下滑囊脂肪層連續(xù)性中斷;(3)完全斷裂:肌腱信號強度明顯增加,形態(tài)明顯異常,如肌腱連續(xù)性中斷、肌腱-肌腹連接處回縮或明顯的肌肉萎縮,即肌肉的信號強度增高。肩峰-三角肌下滑囊脂肪層連續(xù)性中斷或消失。
結(jié) 果
59例患者中,MRI檢查明確診斷肩袖損傷36例;經(jīng)關(guān)節(jié)鏡檢查證實肩袖損傷(包括肌腱炎、部分撕裂和全層撕裂)35例,肩袖組織完整1例。MRI檢查未證實肩袖撕裂而關(guān)節(jié)鏡下見撕裂7例,其他肩關(guān)節(jié)疾病(骨折、肩關(guān)節(jié)不穩(wěn)定、Bankart損傷)經(jīng)MRI檢查與關(guān)節(jié)鏡檢查證實無肩袖損傷17例。MRI診斷肩袖損傷的敏感度為83.3%,特異度為94.1%,準確性為86.4%,陽性預(yù)測值97.2%,陰性預(yù)測值69.6%。經(jīng)關(guān)節(jié)鏡檢查證實肩袖損傷者中,肌腱炎7例,部分肩袖撕裂13例,其中滑囊側(cè)10例,關(guān)節(jié)側(cè)3例。全層撕裂(圖1)22例。
討 論
肩袖損傷是肩關(guān)節(jié)外科的常見病。作為上肢的活動樞紐,肩關(guān)節(jié)決定了整個上肢的活動范圍和活動的空間精確度。而肩袖肌群作為肩關(guān)節(jié)空間位置精確控制的主要動力因素之一,對肩關(guān)節(jié)的功能發(fā)揮起著至關(guān)重要的作用。因此肩袖損傷會使肩關(guān)節(jié)產(chǎn)生不同程度的功能障礙,并伴有疼痛,嚴重影響患者的日常生活和生活質(zhì)量。
我們首先需要明確的是肩袖撕裂是部分撕裂還是全層撕裂。Ellman等[4]將肩袖部分撕裂分三類,即滑囊側(cè)部分撕裂、肌腱間部分撕裂和關(guān)節(jié)側(cè)部分撕裂。每一類根據(jù)撕裂深度分為三度:Ⅰ度,<3 mm;Ⅱ度,3~6 mm;Ⅲ度,>6 mm或超過肌腱厚度50%。在全層斷裂一般根據(jù)斷裂的大小分為:小斷裂(<1 cm)、中斷裂(1~3 cm)、大斷裂(3~5 cm)和巨大斷裂(>5 cm)[5]。
在肩袖損傷的診斷和鑒別診斷上除了詳細詢問病史和查體外,肩關(guān)節(jié)的影像學檢查也是必不可少的診斷手段。其中MRI以其非侵入性、非放射性、解剖重復(fù)性和優(yōu)良的組織對照可比性可進行多角度、多平面、多層次的掃描顯像,能夠同時提供多種組織結(jié)構(gòu)的正常和異常的影像學圖像,成為診斷肩部疾病非常重要的影像學檢查之一[6]。MRI診斷肩袖損傷的敏感度為83.3%,在本組病例中經(jīng)MRI檢查未證實肩袖撕裂而關(guān)節(jié)鏡下可見肩袖撕裂有7例患者。關(guān)節(jié)鏡可清楚的直接觀察到岡上肌腱滑囊側(cè)和關(guān)節(jié)側(cè)肩袖淺層磨損及全層損傷情況,了解肩袖斷裂的范圍、大小和形態(tài);顯示肩關(guān)節(jié)內(nèi)滑膜炎、岡上肌腱退變和肱二頭肌腱部分斷裂等病理改變,其效果是影像學檢查無法比擬的。因此,對肩關(guān)節(jié)疼痛、功能受限、長期保守治療無效、其他檢查方法難以確診患者,采用關(guān)節(jié)鏡檢查十分必要。關(guān)節(jié)鏡不僅能明確診斷,同時也可以進行鏡下手術(shù)治療,如肩關(guān)節(jié)滑膜組織增生、鈣化和岡上肌腱滑膜側(cè)及關(guān)節(jié)側(cè)肩袖淺層磨損的清理、縫合修補等[7]。
綜上所述,MRI檢查對肩袖損傷的診斷價值較高,可以較準確地判斷肩袖損傷程度、大小、范圍及伴發(fā)的合并征象,為臨床制定治療方案提供幫助,最終使患者得到及時正確的治療。
參 考 文 獻
[1] 劉玉杰,盧世璧,張伯勛.肩關(guān)節(jié)撞擊征與肩袖損傷[J].軍醫(yī)進修學院學報,1999,20(1):64-66.
[2] 朱慶生,橋本淳,信原克哉.MRI在常見肩關(guān)節(jié)疾病診斷中的應(yīng)用[J].中華骨科雜志,1999,19(2):103-105.
[3] Chaipat L, Palmer WE.Shoulder magnetic resonance imaging[J].Clin Sports Med,2006,25(3):371-386.
[4] Iannotti JP, Zlatkin MB, Esterhai JL,et al.Magnetic resonance imaging of the shoulder. Sensitivity, specificity, and predictive value[J].J Bone Joint Surg Am,1991,73(1):17-29.
[5] Ellman H.Diagnosis and treatment of incomplete rotator cuff tears[J].Clin Orthop Relat Res,1990,(254):64-74.
[6] Kuhn JE, Dunn WR, Ma B, et al. Interobserver agreement in the classification of rotator cuff tears[J]. J Sports Med,2007,35(3):437-441.
[7] 朱慶生,信原克哉.肩關(guān)節(jié)相關(guān)結(jié)構(gòu)正常與異常的MRI影像學特征[J].中華外科雜志,2000,38(4):259-262.
[8] 劉玉杰,王志剛,王巖,等.肩袖損傷影像學及關(guān)節(jié)鏡診療價值[J].中華創(chuàng)傷雜志,2004,20(1):33-35.