代謝綜合征與泌尿系結石尿液危險因素的相關性
2015-06-01 12:30:16星郭劍明王國民徐志兵王
復旦學報(醫學版) 2015年5期
陳 星郭劍明王國民△徐志兵王 杭
(1復旦大學附屬中山醫院泌尿外科 上海 200032;2中日友好醫院泌尿外科 北京 100029)
代謝綜合征與泌尿系結石尿液危險因素的相關性
陳 星1,2郭劍明1王國民1△徐志兵1王 杭1
(1復旦大學附屬中山醫院泌尿外科 上海 200032;2中日友好醫院泌尿外科 北京 100029)
目的研究代謝綜合征與泌尿系結石尿液危險因素的相關性。方法選取2013年4月至2013年12月在復旦大學附屬中山醫院泌尿外科住院治療的泌尿系結石患者。收集其一般資料、現病史、既往史、血液及尿液檢查結果。比較伴有與不伴有代謝綜合征者之間血液、尿液指標的差異,并進一步采用多因素分析研究代謝綜合征與尿液成分的關系。結果共納入188例泌尿系結石患者,其中50例伴有代謝綜合征。伴有代謝綜合征者的尿液p H值小于不伴有代謝綜合征者,24 h尿液中鈣、磷、尿酸、草酸、鈉、鉀均多于不伴有代謝綜合征者。多因素分析顯示,相比較于不伴有代謝綜合征者,伴有代謝綜合征者的尿液p H值偏低0.4(95%CI:-0.7~-0.1,P=0.014),24 h尿液中鈣偏高1.03 mmol(95%CI:0.08~1.99,P=0.034),尿酸偏高608μmol(95% CI:133~1 083,P=0.012),草酸偏高7.00 mg(95%CI:2.52~11.47,P=0.002)。結論代謝綜合征與尿液中鈣、草酸、尿酸含量增多和尿液酸性程度增加等泌尿系結石的危險因素相關。
代謝綜合征; 泌尿系結石; 危險因素; 尿液成分
腎結石是泌尿外科的常見病,世界范圍內腎結石的患病率為2%~20%[1]。隨著泌尿系結石病因研究的不斷深入,結石的代謝性危險因素越來越被泌尿外科醫師所重視。各種代謝異常導致尿液成分發生變化,尿液危險因素增加是形成泌尿系結石的直接原因,研究人員通過分析結石患者的24 h尿液成分來對代謝狀況進行評估。西方國家有流行病學研究顯示,泌尿系結石的尿液危險因素與肥胖、糖尿病、高血壓、高脂血癥等代謝性疾病相關[2-5],而肥胖、糖尿病、高血壓、高脂血癥均為代謝綜合征(metabolic syndrome,MS)的組成部分[6]。我國與西方國家人種及生活飲食習慣等方面存在一些差異,MS與結石患者尿液成分的關系可能也有區別。為此,本研究分析國人MS與泌尿系結石患者尿液危險因素之間的關系。
資料和方法
研究對象連續收集2013年4月至2013年12月在復旦大學附屬中山醫院泌尿外科住院治療的泌尿系結石患者。符合標準的共188例,男109例(58.0%),女79例(42.0%)。年齡30~76歲,平均(54±8)歲。根據其有無MS分為MS+泌尿系結石(urinary stone disease,USD)組(MS+USD組)和泌尿系結石組(USD組)。
通過病史、體征和術前影像學檢查,包括腹部平片、泌尿系彩超和(或)泌尿系CT,以及術后取出結石明確泌尿系結石。納入標準:采用2007年中國成人血脂異常防治指南制訂聯合委員會在2004年中華醫學會糖尿病學分會建議的基礎上,對MS的組分量化指標修訂后的診斷標準[6],具備以下3項或更多:(1)血三酰甘油(triglyceride,TG)≤1.70 mmol/L(150 mg/d L);(2)血高密度脂蛋白膽固醇(high density lipoprotein cholesterol,HDL-C)<1.04 mmol/L(40 mg/d L);(3)血壓(blood pressure,BP)≤130/85 mm Hg(1 mm Hg=0.133 kPa,下同)或有高血壓史;(4)空腹血糖(fasting blood glucose,FBG)≤6.1 mmol/L(110 mg/d L)或糖負荷后2 h血糖(blood glucose,BG)≤7.8 mmol/L(140 mg/d L)或有糖尿病史;(5)肥胖:男性腰圍>90 cm,女性腰圍>85 cm。由于回顧性研究的限制,本次研究無法獲得研究對象的腰圍數據。根據我國的人口學資料分析顯示,中國人身體質量指數(body mass index,BMI)為25 kg/m2的人群相應的腰圍在男性中約為90 cm,女性約為85 cm[7]。故本研究采用BMI>25 kg/m2作為肥胖的指標。由于BMI和腰圍的關聯非常密切,BMI被認為是腰圍的可靠的替代指標。既往MS診斷標準中,肥胖項目采用BMI作為診斷指標[8]。在一些研究中,BMI也代替了腰圍作為MS的診斷指標[9-12]。排除標準:未滿18歲的未成年人、急慢性腎功能衰竭、腎小管性酸中毒、慢性腹瀉、原發性甲狀旁腺功能亢進癥、甲狀腺功能亢進癥和泌尿系統先天畸形者。
研究方法記錄患者的人口資料、現病史、既往史、身高、體重、生命體征。入院次日清晨采集外周靜脈血并留取清潔中段尿,將之后的24 h尿液全部留存在放置有防腐劑的容器內。以上血液和尿液標本全部由復旦大學附屬中山醫院檢驗科檢測,包括:尿p H值、24 h尿液成分(尿量、鈉、鉀、鈣、磷、鎂、肌酐、尿酸、枸櫞酸、草酸)、腎功能(肌酐、尿素、尿酸)、FBG、空腹血脂(膽固醇、TG、HDL-C、LDL-C)。
統計學方法應用SPSS 19.0統計軟件處理數據。連續性變量以±s表示,對所有連續性變量進行正態性檢驗。符合正態性分布的連續性變量采用t檢驗檢測兩組間的差異;不符合正態性分布的連續性變量采用Mann-Whitney U秩和檢驗檢測兩組間的差異;χ2檢驗檢測兩組間分類變量的差異。采用多因素線性回歸分析對性別、年齡、血肌酐、24 h尿量進行校正,比較兩組間尿液成分的差異。P <0.05為差異有統計學意義。
結 果
188例患者中,來我院初次就診時已是復發性泌尿系結石者有85例(45.2%)。根據有無MS進行分組,(MS+USD)組50例,USD組138例。兩組間性別、年齡的差異無統計學意義(P>0.05)。兩組間BP、BMI、FBG、TG、HDL-C、血尿酸的差異有統計學意義(P<0.05),而血尿素、血肌酐的差異無統計學意義(P>0.05)(表1)。
表1 伴與不伴代謝綜合征的泌尿系結石患者的一般資料和血液指標Tab 1 Demographic,anthropometric and serum characteristics of urinary stone formers with and without metabolic syndrome(±s)
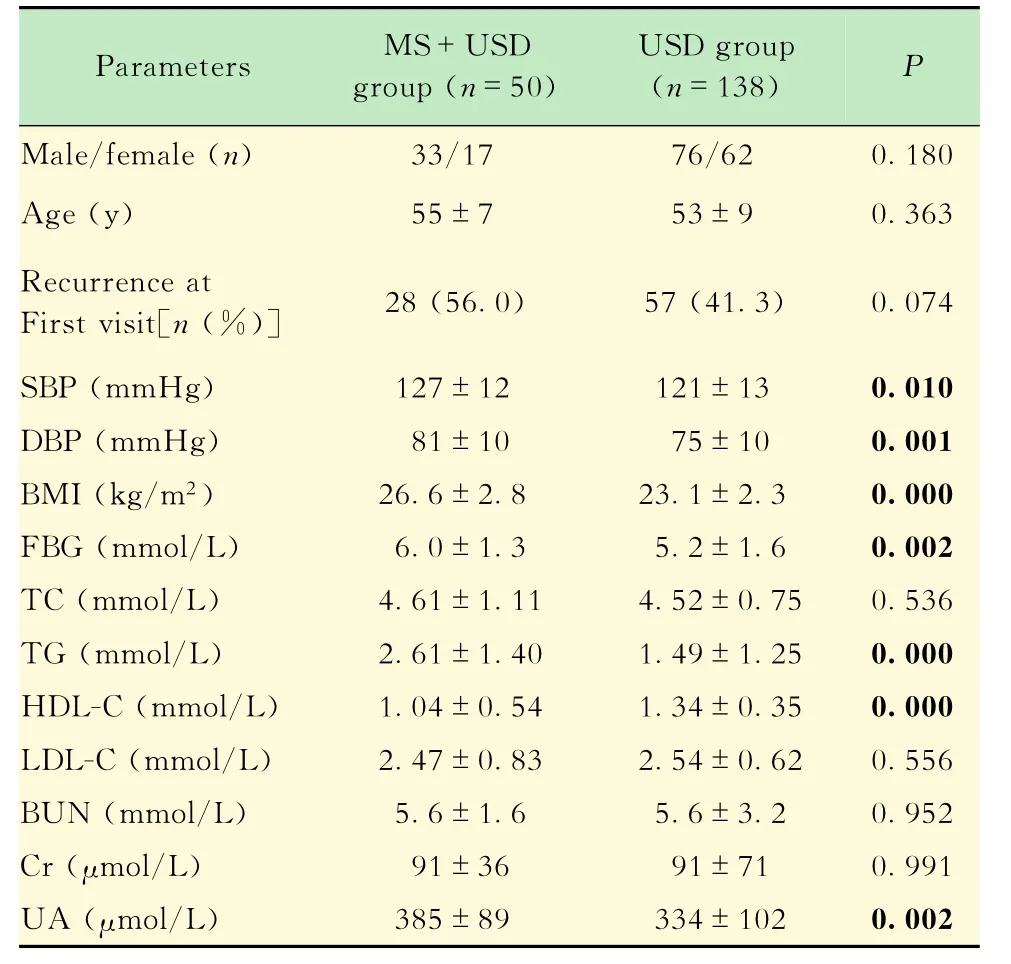
表1 伴與不伴代謝綜合征的泌尿系結石患者的一般資料和血液指標Tab 1 Demographic,anthropometric and serum characteristics of urinary stone formers with and without metabolic syndrome(±s)
MS:Metabolic syndrome;USD:Urinary stone disease;SBP:Systolic blood pressure;DBP:Diastolic blood pressure;BMI:Body mass index;FBG:Fasting blood glucose;TC:Total cholesterol;TG:triglyceride;HDL-C:High density lipoprotein cholesterol;LDL-C:Low density lipoprotein cholesterol;BUN:Blood urea nitrogen;Cr:Creatinine;UA:Uric acid.1 mm Hg=0.133 k Pa.
(MS+USD)組尿p H值低于USD組(P= 0.000)。(MS+USD)組的24 h尿液中,肌酐(P= 0.001)、尿酸(P=0.000)、鈉(P=0.001)、鉀(P= 0.004)、鈣(P=0.001)、磷(P=0.003)、草酸(P= 0.000)的含量均分別高于USD組。而兩組間24 h尿量(P=0.345)、24 h尿鎂(P=0.074)、24 h尿枸櫞酸(P=0.340)的差異均無統計學意義(表2)。
表2 伴與不伴代謝綜合征的泌尿系結石患者的尿液指標Tab 2 Urinary characteristics of urinary stone formers with and without metabolic syndrome(±s)

表2 伴與不伴代謝綜合征的泌尿系結石患者的尿液指標Tab 2 Urinary characteristics of urinary stone formers with and without metabolic syndrome(±s)
MS:Metabolic syndrome;USD:Urinary stone disease;Cr:Creatinine;UA:Uric acid;Na:Sodium;K:Potassium;Ca:Calcium;P:Phosphorus;Mg:Magnesium.
對性別、年齡、血肌酐、24 h尿量進行校正后,MS+USD組患者的尿p H值比USD組低0.4 (95%CI:-0.7~-0.1,P=0.014)。MS+USD組患者比USD組排泄更多的尿酸(608μmol/24 h,95%CI:133~1083,P=0.012)、更多的鈣(1.03 mmol/24 h,95%CI:0.08~1.99,P=0.034)和更多的草酸(7.00 mg/24 h,95%CI:2.52~11.47,P=0.002)。兩組間其余的尿液指標的差異無統計學意義(表3)。
討 論
既往文獻綜述顯示,MS及其組成部分(高血壓、糖尿病、肥胖等)與泌尿系結石相關[13-14]。本研究結果顯示,在泌尿系結石患者中,伴有MS者尿液p H值更低,而24 h尿液中排泄出的鈣、磷、尿酸、草酸、鈉和鉀都高于不伴有MS者;進一步對性別、年齡、血肌酐、24 h尿量等混雜因素進行校正后,伴有MS者的尿液p H值比不伴有MS者低0.4,并且在24 h內多排泄608μmol尿酸、1.03 mmol鈣和7.00 mg草酸。
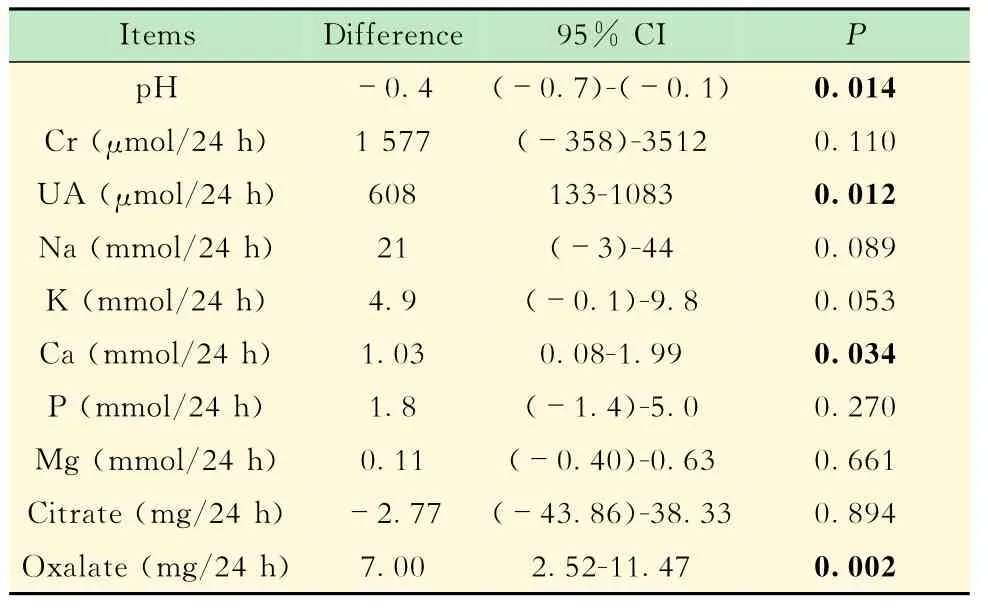
表3 多因素校正后伴與不伴代謝綜合征的泌尿系結石患者尿液指標的差異Tab 3 Multivariate adjusted differences in urinary characteristics of urinary stone formers with and without metabolic syndrome
有研究顯示,泌尿系結石患者中,伴有高血壓者比血壓正常者24 h內多排泄25.6 mg尿鈣[15]。Taylor等[16]認為,糖尿病患者中由于存在著胰島素抵抗,會出現代償性的高胰島素血癥,進而增加尿鈣的排泄量。在肥胖的泌尿系結石患者中,其24 h尿液中的鈣和草酸分別比體重正常者高71 mg和9 mg[17]。Eisner等[18]調查發現,伴有糖尿病的泌尿系結石患者中,24 h尿液中草酸含量比無糖尿病的結石患者多6.43 mg。伴高三酰甘油血癥的結石患者比三酰甘油正常者24 h尿鈣偏多25 mg[5]。本研究與既往研究結果類似,在泌尿系結石患者中,伴有MS者尿鈣和尿草酸排泄量更高。尿液中存在過多的鈣和草酸會導致草酸鈣的過飽和,容易沉積而形成結晶。若晶體在1 min之內相互聚集形成大結晶體,則在腎小管內停留,晶體逐漸生長形成草酸鈣結石[15]。另外,尿液中的尿酸等物質增多后,由于尿酸結晶的晶體特點與草酸鈣結晶相似,草酸鈣結石可能以尿酸為核心進行異質成核[19]。因此,MS者尿鈣和尿草酸的偏高,會增加草酸鈣結石的風險。
有研究發現,酸性尿液是尿酸結石形成的主要危險因素,而MS與此獨立相關[20]。Kim等[21]發現伴有高血壓的泌尿系結石患者的尿液p H值偏低0.23。Eisner等[18]的流行病學調查顯示,伴有糖尿病的泌尿系結石患者的尿液p H值比無糖尿病者低0.34。Powell等[22]對數千名腎結石患者的病史資料回顧性分析后發現,肥胖患者的24 h尿液尿酸與體重正常者的差值在男性中為205.2 mg,在女性中為190.7 mg;肥胖的腎結石患者的尿液p H值低于體重正常者。Taylor等[23]的調查發現,尿液p H值隨著BMI的升高而降低,即使不是肥胖患者,BMI越大的人患泌尿系結石的危險度越高。高脂血癥也與低尿液p H值和尿酸分泌增多相關[24]。本研究同樣證實了這一點,在泌尿系結石患者中,伴有MS者的尿液p H值更低,尿酸排泄更多。細胞實驗和動物模型的研究結果顯示,代謝綜合征與低尿液p H值之間潛在的病理生理學基礎是胰島素抵抗,導致腎近端小管內脂肪酸增多,產生脂毒性,腎臟銨的合成與分泌減少,造成尿液p H值下降[25-26]。尿酸在酸性環境中溶解度降低,析出沉淀增多,容易形成尿酸結晶,進而不斷聚集形成尿酸結石。對糖尿病大鼠應用胰島素增敏劑后,其尿液p H值會升高[27],可見改善胰島素抵抗可以改善尿液的酸性環境,從而降低尿酸結石的風險。
受回顧性研究的限制,未能對研究對象的飲食習慣進行調查,而高鹽、高動物蛋白、高草酸等的攝入是泌尿系結石形成的危險因素;同時,患者既往是否患有炎癥性腸病、是否存在基因異常也未知,這些因素的缺失可能會對研究結果造成偏倚[28]。
尿液中鈣、草酸、尿酸含量增多和尿液p H值降低均為泌尿系結石的危險因素。本研究的結果表明,在泌尿系結石患者中,MS與這些危險因素獨立相關。對于伴有MS的泌尿系結石患者,在處理結石的同時,應重視MS的治療,以減少泌尿系結石的尿液危險因素。
[1]Antonelli JA,Maalouf NM,Pearle MS,et al.Use of the National Health and Nutrition Examination Survey to calculate the impact of obesity and diabetes on cost and prevalence of urolithiasis in 2030[J].Eur Urol,2014,66 (4):724-729.
[2]Taylor EN,Stampfer MJ,Curhan GC.Obesity,weight gain,and the risk of kidney stones[J].JAMA,2005,293 (4):455-462.
[3]Zimmerer T,Weiss C,Hammes HP,et al.Evaluation of urolithiasis:a link between stone formation and diabetes mellitus?[J].Urol Int.2009,82(3):350-355.
[4]Obligado SH,Goldfarb DS.The association of nephrolithiasis with hypertension and obesity:a review [J].Am J Hypertens,2008,21(3):257-264.
[5]Kang HW,Seo SP,Kim WT,et al.Hypertriglyceridemiais associated with increased risk for stone recurrence in patients with urolithiasis[J].Urology,2014,84(4):766 -771.
[6]中國成人血脂異常防治指南制訂聯合委員會.中國成人血脂異常防治指南[J].中華心血管病雜志,2007,35 (5):390-419.
[7]陳蕾,賈偉平,陸俊茜,等.上海市成人代謝綜合征流行調查[J].中華心血管病雜志,2003,31(12):909-912.
[8]中華醫學會糖尿病學分會代謝綜合征研究協作組.中華醫學會糖尿病學分會關于代謝綜合征的建議[J].中華糖尿病雜志,2004,12(3):156-161.
[9]Sundstrom J,Riserus U,Byberg L,et al.Clinical value of the metabolic syndrome for long term prediction of total and cardiovascular mortality:prospective,population based cohort study[J].BMJ,2006,332(7546):878 -882.
[10]Malik S,Wong ND,Franklin SS,et al.Impact of the metabolic syndrome on mortality from coronary heart disease,cardiovascular disease,and all causes in United States adults[J].Circulation,2004,110(10):1245 -1250.
[11]Kadlec AO,Greco K,Fridirici ZC,et al.Metabolic syndrome and urinary stone composition:what factors matter most?[J].Urology,2012,80(4):805-810.
[12]Sakhaee K,Capolongo G,Maalouf NM,et al.Metabolic syndrome and the risk of calcium stones[J].Nephrol Dial Transplant,2012,27(8):3201-3209.
[13]陳星,郭劍明.代謝綜合征與腎結石關系的研究進展[J].復旦學報:醫學版,2013,40(6):752-756.
[14]楊婷,陸澤元.代謝綜合征與腎結石的關系[J].醫學綜述,2014,20(19):3567-3568.
[15]Eisner BH,Porten SP,Bechis SK,et al.Hypertension is associated with increased urinary calcium excretion in patients with nephrolithiasis[J].J Urol.2010,183(2):576-579.
[16]Taylor EN,Stampfer MJ,Curhan GC.Diabetes mellitus and the risk of nephrolithiasis[J].Kidney Int,2005,68 (3):1230-1235.
[17]Ekeruo WO,Tan YH,Young MD,et al.Metabolic risk factors and the impact of medical therapy on the management of nephrolithiasis in obese patients[J].J Urol,2004,172(1):159-163.
[18]Eisner BH,Porten SP,Bechis SK,et al.Diabetic kidney stone formers excrete more oxalate and have lower urine p H than nondiabetic stone formers[J].J Urol,2010,183 (6):2244-2248.
[19]Grases F,Sanchis P,Perello J,et al.Role of uric acid in different types of calcium oxalate renal calculi[J].Int J Urol,2006,13(3):252-256.
[20]陳穎,楊枝,黃飛,等.尿液p H值與代謝綜合征的相關性研究[J].內科理論與實踐,2012,7(6):448-451.
[21]Kim YJ,Park MS,Kim WT,et al.Hypertension influences recurrent stone formation in nonobese stone formers[J].Urology,2011,77(5):1059-1063.
[22]Powell CR,Stoller ML,Schwartz BF,et al.Impact of body weight on urinary electrolytes in urinary stone formers[J].Urology,2000,55(6):825-830.
[23]Taylor EN,Curhan GC.Body size and 24-hour urine composition[J].Am J Kidney Dis,2006,48(6):905 -915.
[24]Li WM,Chou YH,Li CC,et al.Association of body mass index and urine p H in patients with urolithiasis[J].Urol Res,2009,37(4):193-196.
[25]Bobulescu IA,Dubree M,Zhang J,et al.Effect of renal lipid accumulation on proximal tubule Na+/H+exchange and ammonium secretion[J].Am J Physiol Renal Physiol,2008,294(6):F1315-F1322.
[26]Bobulescu IA,Dubree M,Zhang J,et al.Reduction of renal triglyceride accumulation:effects on proximal tubule Na+/H+exchange and urinary acidification[J].Am J Physiol Renal Physiol,2009,297(5):F1419-F1426.
[27]Iba A,Kohjimoto Y,Mori T,et al.Insulin resistance increases the risk of urinary stone formation in a rat model of metabolic syndrome[J].BJU Int,2010,106(10):1550 -1554.
[28]魏勃,安瑞華,腎結石危險因素的研究進展[J].現代泌尿外科雜志,2014,19(12):832-835.
Relationship betweet urinary risk factors of urolithiasis and metabolic syndrome
CHEN Xing1,2,GUO Jian-ming1,WANG Guo-min1△,XU Zhi-bing1,WANG Hang1
(1Department of Urology,Zhongshan Hospital,Fudan University,Shanghai 200032,China;2Department of Urology,China-Japan Friendship Hospital,Beijing 100029,China)
ObjectiveTo investigate the relationship between metabolic syndrome and urinary risk factors of urolithiasis.MethodsAn analysis was performed in urinary stone formers from Apr.,2013,to Dec.,2013,in department of urology,Zhongshan Hospital,Fudan University.The general conditions,history of present illness,past medical history,serum and urinary characteristics were collected.The differences of serum and urinary characteristics were compared between individuals with and without metabolic syndrome.Multivariate analysis was performed to investigate the relationship between metabolic syndrome and urine composition.ResultsOne hundred and eighty-eight patients with urinary stone disease were included,in which 50 cases had metabolic syndrome.Compared with stone formers without metabolic syndrome,those with metabolic syndrome had lower urine p H,and higher calcium,phosphorus,uric acid,oxalate,sodium and potassium in 24-hour urine.On adjusted multivariate analysis compared with stone formers without metabolic syndrome,urine p H ofthose with metabolic syndrome was 0.4 lower[95%CI:(-0.7)-(-0.1),P=0.014].Stone formers with metabolic syndrome excreted 1.03 mmol more calcium(95%CI:0.08-1.99,P= 0.034),608μmol more uric acid(95%CI:133-1 083,P=0.012)and 7.00 mg more oxalate (95%CI:2.52-11.47,P=0.002)in 24-hour urine.ConclusionsMetabolic syndrome was associated with risk factors of urolithiasis such as significantly increased calcium,oxalate,uric acid and acidity of urine.
metabolic syndrome; urolithiasis; risk factor; urinary component
R 692.4
A
10.3969/j.issn.1672-8467.2015.05.006
2015-03-25;編輯:王蔚)
△Corresponding author E-mail:wang.guomin@zs-hospital.sh.cn
猜你喜歡
中老年保健(2022年5期)2022-08-24 02:35:42
中老年保健(2022年1期)2022-08-17 06:14:56
體育科技文獻通報(2022年3期)2022-05-23 13:46:54
中老年保健(2021年5期)2021-08-24 07:07:20
中老年保健(2021年9期)2021-08-24 03:51:04
中老年保健(2021年7期)2021-08-22 07:42:16
中老年保健(2021年11期)2021-08-22 03:15:16
天津外國語大學學報(2021年3期)2021-08-13 08:32:18
遼金歷史與考古(2021年0期)2021-07-29 01:06:54
科技傳播(2019年22期)2020-01-14 03:06:54