營養狀況對阿爾茨海默病與輕度認知功能障礙患者的影響
2015-09-11 19:11:20劉蔚萱
中國當代醫藥 2015年24期
關鍵詞:相關性
劉蔚萱

[摘要] 目的 觀察阿爾茨海默病(AD)和輕度認知功能障礙(MCI)患者臨床營養狀況指標,探討營養因素對AD患者認知功能障礙嚴重程度的影響。 方法 研究納入2013年1月~2014年12月入院確診的50例AD患者,51例MCI患者,另選取50例健康人群作為對照組。所有患者均填寫營養評價量表(MNA)、精神智能量表(MMSE)和社會生活量表(ADL),所有患者清晨空腹靜脈取血,測定葉酸、維生素B12水平。 結果 AD組患者BMI(20.12±5.03)kg/m2顯著低于MCI組的(23.45±4.51)kg/m2和對照組的(24.87±4.43)kg/m2,差異有統計學意義(P<0.05),3組其他營養指標比較,差異無統計學意義(P>0.05);AD組患者葉酸(7.64±2.29)ng/ml和維生素B12水平(408.9±283.2)pg/ml均顯著低于MCI組和對照組(P<0.05);AD組患者和MCI組患者葉酸和維生素B12水平與MMSE及ADL評分無顯著相關性(P>0.05)。 結論 AD患者BMI指數較低,一定程度存在營養障礙,雖然AD患者葉酸和和維生素B12水平下降,但與AD嚴重程度無相關。
[關鍵詞] 阿爾茨海默病;輕度認知功能障礙;營養狀況;葉酸;維生素B12;相關性
[中圖分類號] R742 [文獻標識碼] A [文章編號] 1674-4721(2015)08(c)-0027-04
[Abstract] Objective To observe the clinical nutritional status index of patients with Alzheimer disease (AD) and mild cognitive impairment (MCI),and explore the influence of nutritional factors on severity of MCI in AD patients. Methods 50 AD patients and 51 MCI patients after definite diagnosis from January 2013 to December 2014 were selected into the study.Another group of 50 healthy people was chosen into control group.All participants were asked to fill in mini nutritional assessment(MNA),mini memal state examination(MMSE),and activities of daily living(ADL).The levels of folic acid and vitamin B12 among three groups were determined by venous blood drawing in empty stomach in the morning. Results The body mass index (BMI) in AD group was (20.12±5.03)kg/m2,much lower than that in the MCI group and control group,(23.45±4.51)kg/m2 and (24.87±4.43)kg/m2 respectively(P<0.05).There was no significant difference in other nutritional status index among three groups (P>0.05).The levels of folic acid and vitamin B12 was (7.64±2.29)ng/ml and (408.9±283.2 )pg/ml respectively in AD group, greatly lower than the other two groups (P<0.05).The levels of folic acid and vitamin B12 in AD group and MCI group were not in close correlations with MMSE or ADL(P>0.05). Conclusion The BMI index is lower in AD patients,which indicates nutritional disorder in certain degree.The levels of folic acid and vitamin B12 are decreased in AD patients,but they are not related with the severity of AD.
[Key words] Alzheimer disease;Mild cognitive impairment;Nutritional status;Folic acid;Vitamin B12;Correlation
阿爾茨海默病(Alzheimer disease,AD)是進行性中樞神經系統退行性疾病,因其高患病率、高致殘率及高死亡率引起世界各國的廣泛關注[1]。2010年全世界有3560萬人罹患癡呆(dementia),2010年流行病學調查顯示,我國AD患者為569萬,年發病率為6.25‰,其中女性發病率較男性略高,AD高發人群為>55歲的中老年人,且隨年齡增加,患病率逐漸上升[2]。目前臨床研究表明,晚期AD患者存在不同程度的營養障礙,但營養障礙發生因素尚不明確[3]。本研究通過測定AD、輕度認知功能障礙(mild cognitive impairment,MCI)患者及健康人群的營養狀況和葉酸、維生素B12水平,探討營養因素對AD患者病情發展的影響,分析影響AD患者認知功能障礙的相關因素。
1 資料與方法
1.1 一般資料
研究納入2013年1月~2014年12月入院確診的50例AD患者,51例MCI患者,另選取50例健康人群作為對照組。所有AD、MCI患者均符合2011年美國INA(National Institute of Aging)和阿爾茨海默病協會(Alzheimer Association,AA)診斷標準[4],所有患者參與研究前3個月無維生素服用史。排除抑郁癥、精神病史、血管性癡呆和帕金森病等。AD患者男27例,女23例,年齡55~84歲,平均(69.4±5.7)歲;MCI患者男26例,女25例,年齡50~81歲,平均(68.4±5.1)歲;健康人群男25例,女25例,年齡53~83歲,平均(69.1±5.5)歲。3組人群性別分布、平均年齡等比較,差異無統計學意義(P>0.05),具有可比性。
1.2 方法
所有患者入院后均填寫營養評價量表(MNA)、精神智能量表(MMSE)和社會生活量表(ADL),測量身高、體重,計算體重指數(BMI),簡易營養評估表[5](mini nutritional assessment short-form,MNA-SF)包括6個項目:①BMI;②體重下降程度;③急性疾病或應激;④臥床不起;⑤癡呆或抑郁;⑥食欲下降或進食困難。MNA-SF評分標準:總分30分,≥24分為良好,17~24分為潛在營養不良,<17分為營養不良。所有患者清晨空腹抽取肘靜脈血2 ml,采用全自動化學分析儀(美國貝克曼庫爾特,AU5800)測定葉酸和維生素B12水平。
營養指標包括上臂和小腿周徑,體重下降,總體評價包括是否住院、每日藥物是否3種以上、近3個月疾病、活動能力等;飲食問卷包括每日餐數和飲水量、蛋白質攝入量等,自評包括有無營養障礙,熟人評價等。
1.3 統計學分析
采用SPSS 15.0統計軟件對數據進行分析,計量資料以x±s表示,采用t檢驗,計數資料用百分率(%)表示,采用χ2檢驗,各項指標與阿爾茨海默病進展相關性采用多元Logistic回歸分析,以P<0.05為差異有統計學意義。
2 結果
2.1 3組患者營養狀況的比較
AD患者BMI顯著低于MCI組和對照組,差異有統計學意義(P<0.05),3組患者其他測量指標比較差異無統計學意義(P>0.05)(表1)。
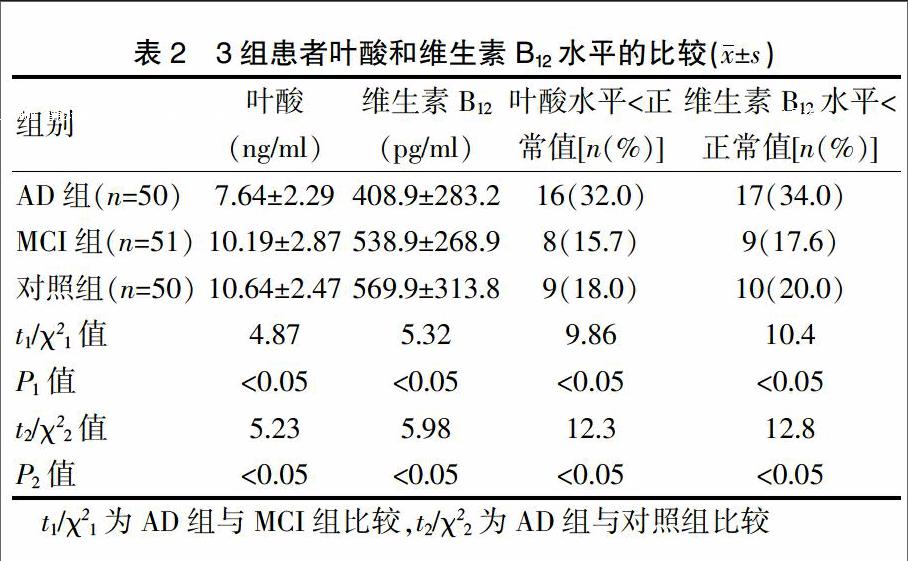
2.2 3組患者葉酸和維生素B12水平的比較
AD組患者葉酸和維生素B12水平均顯著低于MCI組和對照組,差異有統計學意義(P<0.05);32.0%AD組患者葉酸低于正常值,顯著高于MCI組及對照組,差異有統計學意義(P<0.05);34.0%AD組患者維生素B12水平低于正常值,顯著高于MCI組及對照組,差異有統計學意義(P<0.05);MCI組患者較對照組患者各項指標比較,差異無統計學意義(P>0.05)(表2)。
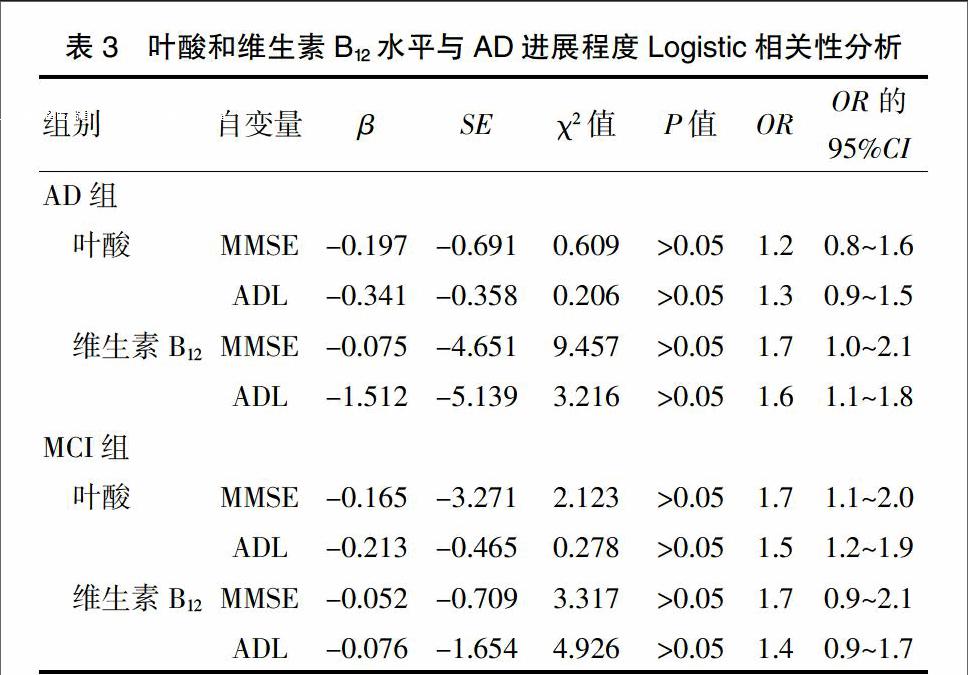
2.3 葉酸和維生素B12水平與AD進展程度相關性
AD患者和MCI患者葉酸和維生素B12水平與MMSE和ADL評分無顯著相關性(P>0.05),提示雖然AD患者葉酸和和維生素B12水平下降,但與AD嚴重程度無相關(表3)。
3 討論
AD是老年癡呆常見類型,由于神經退行性變、腦血管病變、感染、外傷、腫瘤、營養代謝障礙等多種原因引起的疾病,臨床表現為以記憶損害首發的認知功能障礙[6]、日常生活自理能力下降及精神行為異常,AD患者在疾病的整個過程中出現的情感精神行為癥狀,侵擾著高達90%的AD患者及照料者[7]。由于老年癡呆患者認知能力降低,存在不同程度吞咽功能障礙,自我控制力較差,語言溝通能力下降等原因較其他疾病住院的老年患者更易發生營養不良。國外報道癡呆患者營養不良檢出率約為16%,營養風險檢出率約為44%[8]。李玉梅等[9]用MNA-SF篩查某養老院60例AD患者存在營養不良的比例為66.67%。AD發病機制目前尚無定論,有觀點認為,營養及代謝障礙造成了腦組織及其功能受損而導致癡呆,如維生素B1、B12及煙酸、葉酸缺乏癥均可導致癡呆[8]。
目前已有多項研究表明,充足、優質的飲食營養干預可改善AD患者認知功能。2013年由美國醫師醫藥責任協會(Physicians Committee for Responsible Medicine,PCRM)制訂的《飲食預防阿爾茨海默病指南》推薦避免食用飽和脂肪酸和反式脂肪酸,多食用植物性食物,增加維生素E和維生素B的攝入[9]。將飲食與體育鍛煉相結合,避免含有鐵、銅的復合維生素,以最大限度地保護大腦。本研究通過測定AD患者、MCI患者及健康人群的營養狀況和葉酸、維生素B12水平,結果顯示,AD患者BMI顯著低于MCI患者和對照組(P<0.05),AD患者較健康人群存在明顯營養障礙,但本研究中AD患者其他營養指標較MCI患者和健康人群均無明顯差異,推測MNA不適用于進行AD患者營養障礙篩查。
有研究認為,大劑量補充葉酸和(或)維生素B12有助于改善AD患者認知功能障礙[10],也有研究認為,大劑量B族維生素的補充不能抑制AD患者認知功能減退,相反會提高抑郁的發生率[11]。研究指出,缺乏葉酸和維生素B12可升高Hcy水平,Hcy對神經血管具有毒性作用[12-16]。本研究結果顯示,AD患者葉酸和維生素B12水平較MCI患者和健康人群顯著下降,但統計學分析AD患者和MCI患者葉酸和維生素B12水平與MMSE和ADL評分無顯著相關性(P>0.05),提示AD患者葉酸和和維生素B12水平下降與AD嚴重程度無相關。
本研究結果發現,AD患者較健康人群存在顯著營養障礙,但在MCI患者中除BMI指數外,其他營養指標不受影響,提示可能有更敏感的營養監測方法可用于AD患者營養監測。AD患者葉酸和和維生素B12水平下降,與AD嚴重程度無相關,但AD患者仍需注意飲食。
[參考文獻]
[1] Gehrman P,Marler M,Martin JL,et al.The relationship between dementia severity and rest/activity circadian rhythms[J].Neuropsychiatr Dis Treat,2005,1(2):155-163.
[2] Zhang G,Ding H,Chen H,et al.Thiamine nutritional status and depressive symptoms are inversely associated among older Chinese adults[J].J Nutr,2013,143(1):53-58.
[3] Cunnane SC,Schneider JA,Tangney C,et al.Plasma and brain fatty acid profiles in mild cognitive impairment and Alzheimer′s disease[J].J Alzheimers Dis,2012,29(3):691-697.
[4] McKhann GM,Knopman DS,Chertkow H,et al.The diagnosis of dementia due to Alzheimer′s disease:recommendations from the National Institute on Aging-Alzheimer′s Association workgroups on diagnostic guidelines for Alzheimer′s disease[J].Alzheimers Dement,2011,7(3):263-269.
[5] Guigoz Y,Vellas B,Garry PJ.Assessing the nutritional status of the elderly:The Mini Nutritional Assessment as part of the geriatric evaluation[J].Nutr Rev,1996,54(1 Pt 2):59-65.
[6] 尹又,黃流清,李澎,等.阿爾茨海默病與輕度認知障礙患者的營養狀況分析[J].卒中與神經疾病,2010,17(4):217-219.
[7] Pivi GA,da Silva RV,Juliano Y,et al.A prospective study of nutrition education and oral nutritional supplementation in patients with Alzheimer′s disease[J].J Nutr,2011,(10):98.
[8] Guigoz Y.The mininutritional assessment(MNA) review of the literature-what does it tell us?[J].J Nutr Health Aging,2006,10(6):466-485.
[9] 李玉梅,鄧永萍,黃紹寬,等.老年性癡呆患者的營養狀況研究[J].中國老年學雜志,2005,25(5):502-503.
[10] Herrmann N,Gauthier S.Diagnosis and treatment of dementia:6.Management of severe Alzheimer disease[J].CMAJ,2008,179(12):1279-1287.
[11] Goes VF,Mello-Carpes PB,Oliveira LO,et al.Evaluation of dysphagia risk,nutritional status and caloric intake in elderly patients with Alzheimer′s[J].Rev Lat Am Enfermagem,2014,22(2):317-324.
[12] Jyvakorpi SK,Puranen T,Pitkala KH,et al.Nutritional treatment of aged individuals with Alzheimer disease living at home with their spouses: study protocol for a randomized controlled trial[J].Trials,2012,(13):66.
[13] Thaipisuttikul P,Galvin JE.Use of medical foods and nutritional approaches in the treatment of Alzheimer′s disease[J].Clin Pract(Lond),2012,9(2):199-209.
[14] Morris MC,Evans DA,Schneider JA,et al.Dietary folate and vitamins B-12 and B-6 not associated with incident Alzheimer′s disease[J].J Alzheimers Dis,2006,9(4):435-443.
[15] Hu N,Yu JT,Tan L,et al.Nutrition and the risk of Alzheimer′s disease[J].Biomed Res Int,2013(2013):524820.
[16] 何穎,王超,王德才.阿爾茨海默病的非治療藥物及新靶點研究進展[J].中國醫藥導報,2014,11(6):162-166.
(收稿日期:2015-04-24 本文編輯:王紅雙)
猜你喜歡
商情(2016年42期)2016-12-23 14:25:52
商情(2016年42期)2016-12-23 13:35:35
東方教育(2016年4期)2016-12-14 22:15:13
財經界·學術版(2016年19期)2016-11-16 16:28:33
科技視界(2016年21期)2016-10-17 17:37:34
中國實用醫藥(2016年24期)2016-10-17 04:31:12
中國實用醫藥(2016年24期)2016-10-17 03:37:40
中國實用醫藥(2016年24期)2016-10-17 03:35:06
科學與財富(2016年28期)2016-10-14 21:58:50
