初診伴有脊柱轉移的前列腺癌生存相關因素分析
2015-12-21 08:46:08單露玲韓秀鑫張超任志午梁守磊王國文
中國腫瘤臨床 2015年17期
單露玲 韓秀鑫 張超 任志午 梁守磊 王國文
·臨床研究與應用·
初診伴有脊柱轉移的前列腺癌生存相關因素分析
單露玲 韓秀鑫 張超 任志午 梁守磊 王國文
目的:探討初診時伴有脊柱轉移的前列腺癌患者與生存相關的因素。方法:收集2005年1月至2010年12月天津醫科大學腫瘤醫院接受內分泌治療的前列腺癌脊柱轉移患者49例,針對患者的堿性磷酸酶(ALP)、治療前有無骨相關事件(SREs)、Gleason評分、治療后PSA最低值、激素敏感持續時間、有無化療行單因素分析,并對存在統計學意義者進行多因素分析。結果:平均隨訪時間64.1個月,死亡41例,中位生存時間為27個月,1、3、5年生存率分別是81.6%、40.8%、20.4%。單因素分析結果顯示,有無聯合化療、ALP水平、治療前是否出現SRE、Gleason評分、治療后PSA最低值及激素敏感持續時間與總生存率(OS)有關(P<0.05)。Cox回歸模型多因素分析顯示,激素敏感持續時間≥19個月及聯合化療是較長生存時間的獨立預后因素(P<0.05)。結論:激素敏感持續時間及進展為去勢抵抗性前列腺癌(castration resistant prostate cancer,CRPC)后是否聯合化療是前列腺癌脊柱轉移患者的預后獨立因素。
前列腺癌 脊柱轉移 化療 內分泌治療 預后因素
世界范圍內,前列腺癌是男性中第二大常見惡性腫瘤[1],且發病率呈上升趨勢。在西方國家,早期診斷未有遠處轉移的前列腺癌患者,其5年生存率可達100%,若診斷時即出現遠處轉移,5年生存率僅為33%[2]。在我國很多前列腺癌患者在就診時即為晚期,并伴有脊柱轉移,對這一患者群體缺乏統一規范的治療策略。
對于轉移性去勢抵抗性前列腺癌(metastatic castration resistant prostate cancer,mCRPC)患者生存相關的預后因素的分析顯示血清ALP水平、激素敏感持續時間、治療前PSA值、首次骨轉移出現時間、血紅蛋白等是mCRPC的獨立預后因素[3-4],但對于初診即伴有脊柱轉移的前列腺癌患者的預后因素分析報道較少。本研究回顧性分析初診時伴有脊柱轉移的前列腺癌患者的臨床資料,探討影響其生存時間的因素。
1 材料與方法
1.1 臨床資料
收集2005年1月至2010年12月天津醫科大學腫瘤醫院初診伴有脊柱轉移的前列腺癌患者49例,年齡54~81歲,平均為(70.27±7.13)歲,其中年齡<60歲患者為5例,60~70歲患者為17例,年齡>70歲患者為27例。13例在進展為CRPC后給予多西他賽化療,22例以劇烈疼痛就診,20例行脊柱轉移病灶放療,2例行椎體穿刺活檢+椎體成形術,本研究中未納入病理性骨折或截癱的患者。
確診時ALP為53~1 141 U/L,中位數為179 U/L,治療前即出現骨相關事件(SRE)的為17例,Gleason評分5~6分為14例,7分為8例,8~10分為27例,治療后PSA最低值為0.03~5 328 μg/L,激素敏感持續時間為0~49個月,中位數為19個月。
1.2 方法
1.2.1 納入標準 1)前列腺或轉移病灶病理結果確診;2)影像學或組織活檢確診脊柱轉移;3)經治療后轉變為CRPC。排除標準:1)伴有骨外遠處轉移;2)伴有全身其他影響生存的其他疾病,如心臟病、其他癌癥等。
1.2.2 治療 26例行雙側睪丸切除術,23例給予亮丙瑞林或戈舍瑞林,同時均輔助應用抗雄激素藥物,其中13例在病情進展后給予多西他賽化療。
1.3 統計學方法
應用SPSS 19.0統計軟件對隨訪結果進行分析。采用Kaplan-Meier法行生存相關單因素分析,并行Log-rank檢驗,采用Cox模型行多因素分析。P<0.05為差異有統計學意義。
2 結果
2.1 生存分析
平均隨訪時間64.1個月,至隨訪截止。死亡41例,中位生存時間為27個月,1、3、5年生存率分別是81.6%、40.8%、20.4%。
2.2 單因素生存分析
合并化療、確診時ALP值<179 U/L、治療前未出現SRE、Gleason評分<7分、PSA最低值<10 μg/L以及激素敏感持續時間≥19個月與較長OS有關(P<0.05,表1)。
2.3 多因素生存分析
Cox回歸模型多因素生存分析結果顯示,疾病進展后合并化療及激素敏感持續時間≥19個月是較長生存時間的獨立預后因素(P<0.05,表1,圖1,2)。

表1 變量的生存相關分析Table 1 Survival-related analysis of the variables

圖1 不同治療方式的生存曲線Table 1 Survival curves of various treatment methods
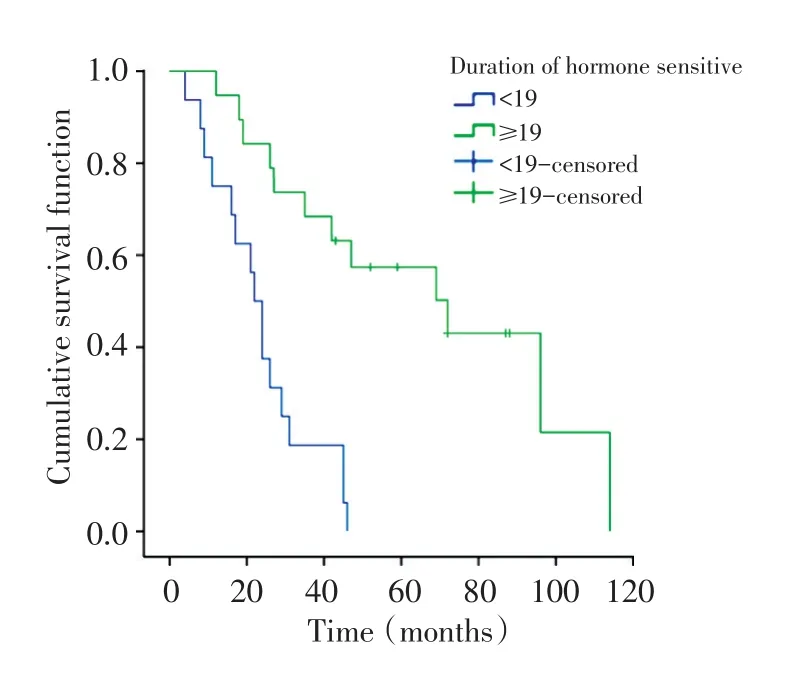
圖2 PSA敏感時間相關生存曲線Table 2 PSA sensitization time-related survival curves
3 討論
前列腺是骨轉移瘤的第二大原發病灶,是男性骨轉移瘤最常見的原發病,其中脊柱是骨轉移的高發部位。與脊柱外骨轉移相比,前列腺癌脊柱轉移往往更早出現癥狀,且能夠造成劇烈疼痛、麻木、癱瘓等不良后果,同時由于前列腺癌對內分泌治療敏感,生存期相對較長,為改善患者生活質量,一部分患者需要外科干預,而脊柱外骨轉移則多以前列腺癌綜合治療為主。在我國,很大一部分前列腺癌患者以脊柱轉移癥狀起病,目前缺乏對這些患者的標準治療,研究影響這一患者群的預后因素可以有效指導臨床治療。
脊柱轉移瘤包括成骨型、溶骨型與混合型。溶骨型X線平片表現為椎體骨質破壞、變扁,但椎間隙多保持正常、椎弓根多受侵蝕;CT表現為低密度缺損區,常伴有軟組織腫塊。成骨型X線片表現為斑片狀或結節樣高密度影、椎體不壓縮變扁,CT表現為松質骨內的高密度灶,一般無軟組織腫塊。MRI表現以T1加權像最為明顯,表現為與正常骨髓脂肪高信號高度對比的低信號。混合型兼有成骨型與溶骨型的表現。
前列腺癌脊柱轉移以成骨型病變為主,臨床上晚期前列腺癌脊柱轉移以混合型病變為主。而其他來源的脊柱轉移,如肺癌、腎癌、肝癌等多以溶骨型病變為主,且相對于前列腺癌脊柱轉移,局灶病變進展較快。內分泌治療是激素依賴型前列腺癌骨轉移患者主要的治療手段,內分泌治療引起的骨丟失會促進轉移性前列腺癌細胞在骨內生長[5],這會加速引起SRE的發生,增加死亡風險并降低生活質量,因此需要對骨轉移病灶行針對性治療。作為重要的骨保護劑,唑來膦酸可降低SREs的發生率[6-7],地諾單抗被證實可延緩非轉移性去勢抵抗性前列腺癌(non-metastatic castration resistant prostate cancer, nm-CRPC)患者發生骨轉移[8]。對于出現頑固性疼痛、骨折及脊髓壓迫癥狀的患者可選擇局部放療或手術,放療可緩解骨轉移引起的骨痛,手術可緩解疼痛、預防/固定骨折、提高生存質量等[9]。20世紀80年代以前手術治療脊柱轉移瘤尚未得到認可,放療是脊柱轉移的標準治療。Nguyen等[10]研究顯示傳統的放療可以在治療3個月后有效緩解疼痛,并對患者的心理變化有積極影響。最新研究顯示單純立體定向放療或聯合開放手術可有效控制局灶病變,改善神經功能[11]。本研究中20例患者進行了轉移病灶放療,2例患者行姑息性手術,但均與OS無關。臨床上部分伴有截癱的前列腺癌脊柱轉移患者經手術治療后可恢復或改善神經功能,同時可明顯緩解疼痛。
自2004年以來多西他賽聯合潑尼松已成為轉移性CRPC的標準一線治療方案[12],但臨床中轉移性前列腺癌的治療仍不規范。本研究顯示初診伴有脊柱轉移的前列腺癌患者經綜合治療后中位生存期為27個月,內分泌治療后約19個月進展為去勢抵抗性前列腺癌,進展為mCRPC后給予多西他賽化療可有效延長患者生存期,對于多西他賽治療失敗的mCRPC患者,多項臨床試驗進行相關研究證實卡巴他賽可延長多西他賽耐藥患者的總生存期(OS)及無進展生存期(PFS),阿比特龍可延長OS及增加PSA反應率[13-14]。此外,轉移性前列腺癌經一線內分泌治療進展后可選擇二線內分泌治療,包括更換/暫停抗雄激素藥物,使用雌激素等。Narimoto等[15]的研究指出CRPC患者治療時,將抗雄激素藥物由比卡魯胺更換為氟他胺后,PSA反應率達87.5%。本研究中單純內分泌治療相對于內分泌治療聯合化療死亡風險增加了3.9倍。
骨是前列腺癌最常見轉移部位,90%以上的CRPC患者會出現骨轉移[6,16],一部分患者在內分泌治療之前即出現骨轉移。前列腺癌骨轉移引起成骨與破骨活性紊亂,造成血清ALP升高。本研究認為Gleason評分、ALP水平、治療前有無合并SRE、經內分泌治療后PSA達到的最低值均與患者生存時間相關,但僅是否聯合化療及激素敏感持續時間是與OS相關的獨立預后因素。Fizazi等[3]對1 901例mCRPC患者進行分析,結果顯示ALP、骨特異性堿性磷酸酶(BSAP)、有無疼痛、既往SRE、首次骨轉移出現時間與生存時間相關。對于mCRPC患者化療后生存相關因素的多因素分析中,化療前ALP濃度、Hb濃度、激素敏感時間及化療周期是與生存相關的獨立預后因素[17]。有研究顯示內分泌治療后PSA最低值是轉移性前列腺癌預后獨立因素[18]。
[1] Ferlay J,Shin HR,Bray F,et al.Estimates of worldwide burden of cancer in 2008:GLOBOCAN 2008[J].Int J Cancer,2010,127 (12):2893-2917.
[2] Muralidharan A,Smith MT.Pathobiology and management of prostate cancer-induced bone pain:recent insights and future treatments[J].Inflammopharmacology,2013,21(5):339-363.
[3] Fizazi K,Massard C,Smith M,et al.Bone-related Parameters are the Main Prognostic Factors for Overall Survival in Men with Bone Metastases from Castration-resistant Prostate Cancer[J]. Eur Urol,2014,68(1):42-50.
[4] Halabi S,Lin CY,Small EJ,et al.Prognostic model predicting metastatic castration-resistant prostate cancer survival in men treated with second-line chemotherapy[J].J Natl Cancer Inst, 2013,105(22):1729-1737.
[5] Ottewell PD,Wang N,Meek J,et al.Castration-induced bone loss triggers growth of disseminated prostate cancer cells in bone[J]. Endocr Relat Cancer,2014,21(5):769-781.
[6] Nilsson S,Franzen L,Parker C,et al.Bone-targeted radium-223 in symptomatic,hormone-refractory prostate cancer:a ran?domised,multicentre,placebo-controlled phaseⅡstudy[J].Lan?cet Oncol,2007,8(7):587-594.
[7] Ryan CJ,Saylor PJ,Everly JJ,et al.Bone-targeting radiopharma?ceuticals for the treatment of bone-metastatic castration-resis?tant prostate cancer:exploring the implications of new data[J].On?cologist,2014,19(10):1012-1018.
[8] Smith MR,Saad F,Coleman R,et al.Denosumab and bone-me?tastasis-free survival in men with castration-resistant prostate cancer:results of a phase 3,randomised,placebo-controlled trial [J].Lancet,2012,379(9810):39-46.
[9] Han XX,Wang GW,Zhang C,et al.Survival analysis of 121 pa?tients with spinal metastases accepted spinal surgery[J].Chinese Journal of Orthopaedics,2014,34(11):1127-1133.[韓秀鑫,王國文,張 超,等.121例脊柱轉移瘤手術治療的療效分析[J].中華骨科雜志,2014,34(11):1127-1133]
[10]Nguyen J,Chow E,Zeng L,et al.Palliative response and func?tional interference outcomes using the Brief Pain Inventory for spinal bony metastases treated with conventional radiotherapy[J]. Clin Oncol(R Coll Radiol),2011,23(7):485-491.
[11]Bate BG,Khan NR,Kimball BY,et al.Stereotactic radiosurgery for spinal metastases with or without separation surgery[J].Neuro?surg Spine,2015,22(4):409-415.
[12]Horwich A,Hugosson J,de Reijke T,et al.Prostate cancer:ES?MO Consensus Conference Guidelines 2012[J].Ann Oncol,2013, 24(5):1141-1162.
[13]de Bono JS,Oudard S,Ozguroglu M,et al.Prednisone plus caba?zitaxel or mitoxantrone for metastatic castration-resistant pros?tate cancer progressing after docetaxel treatment:a randomised open-label trial[J].Lancet,2010,376(9747):1147-1154.
[14]de Bono JS,Logothetis CJ,Molina A,et al.Abiraterone and in?creased survival in metastatic prostate cancer[J].N Engl J Med, 2011,364(21):1995-2005.
[15]Narimoto K,Mizokami A,Izumi K,et al.Adrenal androgen lev?els as predictors of outcome in castration-resistant prostate can?cer patients treated with combined androgen blockade using fluta?mide as a second-line anti-androgen[J].Int J Urol,2010,17(4): 337-345.
[16]Hotte SJ,Saad F.Current management of castrate-resistant pros?tate cancer[J].Curr Oncol,2010,17(Suppl 2):S72-S79.
[17]Qu YY,Dai B,Kong YY,et al.Survival analysis of patients with metastatic castration-resistant prostate cancer treated with docetaxel plus prednisone[J].Chinese Journal of Urology,2013,34(7):505-509.[瞿元元,戴 波,孔蘊毅,等.多西他賽聯合潑尼松治療轉移性去勢抵抗性前列腺癌的臨床分析[J].中華泌尿外科雜志,2013,34(7):505-509.]
[18]Miyamoto S,Ito K,Miyakubo M,et al.Impact of pretreatment factors,biopsy Gleason grade volume indices and post-treatment nadir PSA on overall survival in patients with metastatic prostate cancer treated with step-up hormonal therapy[J].Prostate Can?cer Prostatic Dis,2012,15(1):75-86.
(2015-05-07收稿)
(2015-07-13修回)
(編輯:楊紅欣)
Analysis of prognostic factors associated with survival in men with prostate cancer accompanied by spinal metastases at first diagnosis
Luling SHAN,Xiuxin HAN,Chao ZHANG,Zhiwu REN,Shoulei LIANG,Guowen WANG
Department of Bone and Soft Tissue Oncology,Tianjin Medical University Cancer Institute and Hospital,National Clinical Research Center for Cancer,Key Laboratory of Cancer Prevention and Therapy,Tianjin 300060,China
Objective:Prostate cancer frequently metastasizes to the spine.In this study,we investigate the prognostic factors associated with survival in patients with prostate cancer accompanied by spinal metastases at their preliminary diagnosis.Methods:Clinical data of 49 patients who were diagnosed with spinal metastasis from prostate cancer between January 2005 and December 2010 were analyzed.Variables including alkaline phosphatase(ALP),previous skeletal-related event,Gleason score,prostate-specific antigen(PSA)nadir,and time to castration resistance were obtained.Moreover,the relationship between these variables and overall survival(OS)was analyzed.Survival analysis was performed by using Kaplan-Meier curves.Furthermore,the differences among the OS rates were assessed by using the log rank test.The variables were statistically significant in the univariate analysis(P<0.05)and were included in the multivariate model.Results:The average follow-up time was 64.1 months among the 49 patients.By the end of the follow-up,41 of these patients were dead;the mean survival was 27 months.The 1-,3-,and 5-year survival rate was 81.6%,40.8%, and 20.4%,respectively.Univariate analysis identified that 6 variables were statistically significant prognostic factors of OS:with or without chemotherapy,ALP,previous skeletal-related event,Gleason score,PSA nadir,and time to castration resistance.The multivariate analysis showed that the time to castration resistance of≥19 months and the addition of chemotherapy after disease progression are independent prognostic factors for a high OS.Conclusion:With or without chemotherapy and the time to castration resistance are the independent prognostic factors associated with survival in patients with prostate cancer accompanied by spinal metastases at first diagnosis.
prostate cancer,spinal metastasis,chemotherapy,endocrine therapy,prognosis

10.3969/j.issn.1000-8179.2015.17.515
天津醫科大學腫瘤醫院骨與軟組織腫瘤科,國家腫瘤臨床醫學研究中心,天津市腫瘤防治重點實驗室(天津市300060)
王國文 wgwhrb@163.com
單露玲 專業方向為骨與軟組織腫瘤臨床治療與基礎研究。
E-mail:945490577@qq.com
猜你喜歡
民用飛機設計與研究(2020年4期)2021-01-21 09:15:02
家庭醫學(下半月)(2020年3期)2020-05-30 12:42:02
家庭醫學(下半月)(2020年3期)2020-05-30 12:42:00
家庭醫學(下半月)(2020年3期)2020-05-30 12:42:00
家庭醫學(下半月)(2020年3期)2020-05-30 12:42:00
中國生殖健康(2019年7期)2019-01-06 09:27:34
電子制作(2018年18期)2018-11-14 01:48:24
山東工業技術(2016年15期)2016-12-01 05:31:22
中國男科學雜志(2016年5期)2016-12-01 05:20:23
中國中醫藥現代遠程教育(2014年11期)2014-08-08 13:23:44
