靜脈溶栓治療以頻發TIA為臨床表現的急性腦梗死療效觀察
2015-12-22 06:37:28張春陽張會嶺石秋艷李艷玲
中國實用神經疾病雜志 2015年10期
張春陽 張會嶺 石秋艷 李艷玲
1)河北聯合大學附屬醫院神經重癥科 唐山 063000 2)河北遷安市中醫醫院 遷安 064400
靜脈溶栓治療以頻發TIA為臨床表現的急性腦梗死療效觀察
張春陽1)張會嶺2)石秋艷1)李艷玲1)
1)河北聯合大學附屬醫院神經重癥科 唐山 063000 2)河北遷安市中醫醫院 遷安 064400
目的 觀察靜脈溶栓治療頻發TIA為臨床表現的急性腦梗死患者的療效及預后。方法 選擇我院2008-01-01—2013-12-31以頻發TIA為臨床表現的急性腦梗死靜脈溶栓患者56例為治療組,選擇同期未行溶栓治療的患者30例為對照組,采用NIHSS評分及改良的Rankin評分評價早期療效及遠期預后。結果 2組患者溶栓前ABCD2評分(6.12±3.49 vs 5.78±4.13,P=0.23)、DWI陽性率(39.28%vs 36.67%,P=0.19)差別無統計學意義。溶栓后早期治療有效率(51.78% vs 30.00%,P=0.001)、遠期預后預后良好率(48.21%vs 33.33%,P=0.003)差別具有統計學意義。在出血轉化率方面(8.93%vs 6.67%,P=0.07)差異無統計學意義。結論 以頻發TIA為臨床表現的急性腦梗死患者靜脈溶栓治療安全有效。
短暫性腦缺血發作;急性腦梗死;靜脈溶栓;預后
短暫性腦缺血發作(transient ischemic attack,TIA)是一種常見的缺血性腦血管疾病,部分患者可以進展為腦梗死,是神經科主要的急癥疾病之一[1]。近年來,TIA的定義有很大轉變,2009年ASA發布TIA新定義:腦、脊髓或視網膜局灶性缺血所致的、未伴急性腦梗死的短暫性神經功能障礙[2]。由傳統的以時間基礎(time-based)過渡到目前以組織完整性為基礎(tissue-based),也就是說TIA的診斷更加注重是否存在腦組織損傷。短暫性腦缺血發作定義的重新界定,有可能使溶栓治療的適應證進一步放寬。頻發TIA是指24h內TIA發作2次或2次以上者,其特殊性在于發作頻繁及更高的腦梗死風險[3]。在此,我們回顧性研究了以頻繁短暫性腦缺血發作為臨床表現的急性腦梗死患者溶栓治療的預后,以期對臨床具有一定的指導作用。
1 對象與方法
1.1 對象 本項研究為回顧性研究,收集我院2008-01-01—2013-12-31以頻發TIA住院患者共68例,所有患者入院后24h內均行顱腦DWI檢查,并進行ABCD2評分。依據是否行靜脈溶栓治療分為治療組(42例)和對照組(26例)。入選標準:(1)年齡18~80歲;(2)腦功能損害的體征持續存在>1h,且癥狀最重時NIHSS(美國國立衛生研究院卒中量表)評分>4分;(3)腦CT已排除顱內出血,且無早期腦梗死低密度改變及其他明顯的早期腦梗死改變;(4)血壓控制在180/110mmHg(1mmHg=0.133kPa)以下;(5)無出血傾向及出血性疾病;(6)無嚴重的重要臟器功能障礙或衰竭;(7)患者或家屬簽署知情同意書。對照組符合上述1~6條,但未進行溶栓治療。
1.2 方法
1.2.1 靜脈溶栓治療:給予rt-PA 0.9mg/kg(總量不超過90mg),其中的10%靜脈推注,時間大于1min,余下的90%溶于適量溶液中,1h內靜脈輸入。溶栓24h后復查頭顱CT排除顱內出血后給予阿司匹林片抗血小板聚集治療。未進行溶栓治療的患者直接給予抗血小板聚集治療。
1.2.2 療效評價:早期療效評價:神經功能缺損評分采用美國國立衛生研究院卒中量表(NIHSS),在靜脈溶栓治療7d 后NIHSS評分降低4分認為早期治療有效,NIHSS評分升高4分或死亡認為是無效或惡化[4]。
遠期預后:應用90d改良Rankin量表(mRS)評分評價預后,90d時mRS 0~2分者為預后良好,3~6分包括死亡為預后不良。
1.3 統計學方法 采用SPSS 17.0統計學軟件進行統計分析,計量資料以±s表示,采用t檢驗,計數資料以率(%)表示,采用卡方檢驗,P<0.05為差異有統計學意義。
2 結果
2組患者入院時ABCD2評分、DWI陽性率及治療后出血轉化率差異無統計學意義(P>0.05)(表1)。治療組有效29例(51.78%),預后良好27例(48.21%),對照組有效9例(30.00%),預后良好10例(33.33%),2組療效差異具有統計學意義(P<0.05)。
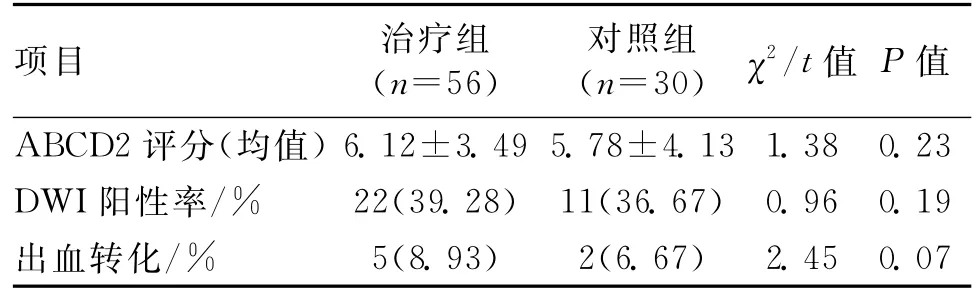
表1 2組患者基本資料比較
3 討論
腦卒中是目前世界上最主要的致殘致死疾病之一[5],短暫性腦缺血發作具有刻板性、發作性及可逆性特點,雖然有時表現癥狀輕微,卻是腦梗死出現前的高預警信號。有研究[6]表明,不經處理的短暫性腦缺血發作具有早期卒中及遠期預后不良的高風險。按照傳統定義,TIA主要關注發作時間,忽略了組織損害,這與近幾年很多的臨床研究存在矛盾之處。Kono等[7]研究發現,TIA患者24h內行DWI檢查陽性率高達35%。但此項研究樣本量較小,似乎說服力不強。Brazzelli等[8]總結了47篇文獻9 078名患者,結果表明34.3%的TIA患者行DWI檢查發現了梗死病灶,與Kono的結果相近,說明即使是臨床癥狀完全恢復的TIA患者仍然有可能存在不可逆的神經細胞壞死。尤其是頻繁發作的TIA患者,因其特殊的發作形式,這種風險更高。有研究表明[9],相對于發作癥狀較為單一的TIA患者,反復發作及發作形式多樣更容易進展成腦梗死。一些研究同時總結了TIA患者發展為腦梗死的可能危險因素。Al-Khaled等[10]認為,TIA發展為急性腦梗死與運動障礙、失語以及入院時NIHSS評分≥10分有關。而Sato等[11]則考慮梗死風險與頸動脈狹窄、高ABCD2評分及DWI早期顯影高度相關。因此,對于頻發TIA的患者應該作為神經科急癥給予積極處理。
溶栓治療是目前唯一能夠使閉塞血管再通的治療方法,雖然對于以短暫性腦缺血發作為首要臨床表現的急性腦梗死患者溶栓療效存在不同看法,但多數研究給予肯定結論。Uchino等[12]在一項回顧性研究中發現,短暫性腦缺血發作患者在梗死前給予溶栓治療減少了嚴重卒中的發生。Ji等[13]的研究對象為年輕的TIA患者,發病年齡18~45歲,其中29例在院內給予溶栓治療,超過一半的患者預后良好且無顱內出血的發生。有研究[14]指出,雖然卒中發作前伴TIA的患者能夠更早獲得處理,但相對于不伴TIA的卒中患者,其發作的嚴重性、給予溶栓治療后mRS評分及出血轉化差異均無統計學意義。而Sobolewski等[15]把卒中發作前24h內發生TIA的患者作為研究對象,似乎得到了不一樣的結果:卒中發作前24h內發生TIA的患者溶栓后具有更高的顱內出血傾向,預后可能更差。
在我們的研究中,2組患者入院時ABCD2評分差異不明顯,說明2組患者具有可比性;DWI陽性率39.28%vs 36.67%,這與既往的研究相比比率似乎更高,考慮與患者反復發作缺血造成組織損傷更加明顯有關。相對于未溶栓的TIA患者,給予溶栓治療的患者不管是在早期療效還是在遠期預后均明顯優于對照組(P<0.05)。在出血轉化方面,2組患者間差異無統計學意義,說明頻發TIA患者進展為腦梗死后積極進行阿替普酶靜脈溶栓治療安全有效。頻發的短暫性腦缺血發作進展為急性腦梗死的風險極高,對于住院患者要仔細觀察病情變化,每次發作前都應該嚴格重新計時[16],一旦發病時間超過1h,應積極給予溶栓治療。
[1]Okada Y.Transient ischemic attack as a medical emergency [J].Front Neurol Neurosci,2014,33(4):19-29.
[2]Easton JD,Saver JL,Albers GW,et al.Definition and evalua-tion of transient ischemic attack:a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association Stroke Council;Council on Cardiovascular Surgery and Anesthesia;Council on Cardiovascular Radiology and Intervention;Council on Cardiovascular Nursing;and the Interdisciplinary Council on Peripheral Vascular Disease[J].Stroke,2009,40(6):2 276-2 293.
[3]Ferrero E,Ferri M,Viazzo A,et al.A retrospective study on early carotid endarterectomy within 48hours after transient ischemic attack and stroke in evolution[J].Ann Vasc Surg,2014,28(1):227-238.
[4]Kerr DM,Fulton RL,Lees KR.Seven-Day NIHSS is a sensitive outcome measure for exploratory clinical trials in acute stroke:evidence from the Virtual International Stroke Trials Archive[J].Stroke,2012,43(5):1 401-1 403.
[5]Donnan GA,Fisher M,Macleod M,et al.Stroke[J].Lancet,2008,371(6):1 612-1 623.
[6]Chatzikonstantinou A,Willmann O,J ger T,et al.Transient ischemic attack patients with fluctuations are at highest risk for early stroke[J].Cerebrovasc Dis,2009,27(6):594-598.
[7]Kono Y,Shimoyama T,Sengoku R,et al.Clinical characteristics associated with abnormal diffusion-weighted images in patients with transient cerebralischemic attack[J].Stroke Cerebrovasc Dis,2014,23(5):1 051-1 055.
[8]Brazzelli M,Chappell FM,Miranda H,et al.Diffusion-weighted imaging and diagnosis of transient ischemic attack[J].Ann Neurol,2014,75(1):67-76.
[9]Phan TG,Sanders L,Srikanth V.Recent advances in the management of transient ischaemic attack:a clinical review[J].Intern Med,2013,43(4):353-360.
[10]Al-Khaled M,Matthis C,Münte TF,et al.The incidence and clinical predictors of acute infarction in patients with transient ischemic attack using MRI including DWI[J].Neuroradiology,2013,55(2):157-163.
[11]Sato S,Minematsu K.Transient ischemic attack:past,present,and future[J].Brain Nerve,2013,65(7):729-738.
[12]Uchino K,Massaro L,Hammer MD.Transient ischemic attack after tissue plasminogen activator:aborted stroke or unnecessary stroke therapy[J].Cerebrovasc Dis,2010,29(1):57-61.
[13]Ji R,Schwamm LH,Pervez MA,et al.Ischemic stroke and transient ischemic attack in young adults:risk factos,diagnostic yield,neuroimaging,and thrombolys-is[J].JAMA Neurol,2013,70(1):51-57.
[14]Alonsode Leciana M,Fuentes B,Masjuan J,et al.Thrombolytic therapy for acute ischemic stroke after recent transient ischemic attack[J].Int J Stroke,2012,7(3):213-218.
[15]Sobolewski P,Brola W,Wiszniewska M,et al.Intravenous thrombolysis with rt-PA for acute ischemic stroke within 24h of a transient ischemic attack[J].Neurol Sci,2014,340(1/2):44-49.
[16]Tsivgoulis G,Sharma VK,Mikulik R,et al.Intraveno us thro mbolysis for acute ischemic stroke occurring during hospitalization for transient ischemic at-tack[J].Int J Stroke,2014,9(4):413-418.
(收稿2014-07-26)
Observation of intravenous thrombolytic therapy for acute cerebral infarction patients with main manifestation of clustering TIA
Zhang Chunyang*,Zhang Huiling,Shi Qiuyan,Li Yanling
*Department of Neurology,the Affiliated Hospital of Hebei Union University,Tangshan 063000,China
Objective To observe the effect and prognosis of acute cerebral infarction patients with main manifestation of clustering TIA treated by intravenous thrombolytic therapy.Methods 56with acute cerebral infarction patients with clustering TIA as clinical manifestation treated by intravenous thrombolytic therapy in our hospital from 2008to 2013were collected as treatment group,and 30patients without thrombolytic therapy in the corresponding period were selected as control group.NIHSS and modified Rankin Scale were used to evaluate early therapeutic effect and long-term prognosis.Results There were no significant differences between the two groups in ABCD2scale(6.12±3.49vs 5.78±4.13,P=0.23)and positive rate of DWI(39.28%vs 36.67%,P=0.19)before treated by thrombolysis.The differences were statistically significant in the effective rate of in early stage after thrombolytic therapy(51.78%vs 30.00%,P=0.001)and the rate of benign prognosis(48.21% vs 33.33%,P=0.003).The rate of hemorrhagic transformation showed no statistical difference between two groups(8.93% vs 6.67%,P=0.07).Conclusion It is safe and effective of intravenous thrombolytic therapy for acute cerebral infarction patients with clustering TIA as clinical manifestation.
Transient ischemic attack;Acute cerebral infarction;Intravenous thrombolysis;Prognosis
R743.33
A
1673-5110(2015)10-0003-02
唐山市科技局課題(課題編號13130206a)