耐多藥結核病快速診斷技術對耐二線藥結核菌診斷價值的Meta分析*
2016-06-06 05:32:36馬峻郭毅
微循環學雜志 2016年2期
關鍵詞:研究
馬 峻 郭 毅
guoyi@whu.edu.cn
?
耐多藥結核病快速診斷技術對耐二線藥結核菌診斷價值的Meta分析*
馬峻1郭毅2,#
guoyi@whu.edu.cn
【摘要】目的:Meta分析耐多藥結核病快速診斷技術(Genotype MTBDRsl)對耐二線藥結核菌研究中的臨床診斷效能。方法:檢索Pubmed、Embase和Cochrane圖書館等數據庫從建庫至2015-01有關Genotype MTBDRsl技術對耐二線藥結核菌應用診斷的研究文獻,采用QUADAS-2條目進行質量評估,符合納入標準的研究應用Meta-Disc軟件進行異質性檢驗,計算其合并靈敏度、特異度、陽性似然比、陰性似然比、診斷比值比及95%可信區間,建立受檢者工作特征曲線(SROC),通過曲線下面積(AUC)評估Genotype MTBDRsl技術在診斷耐二線藥結核菌中的價值,比較其對臨床樣本和培養株樣本耐二線藥的敏感度和特異度,并評價文獻發表偏倚。結果:共納入22篇文獻,其整體研究的異質性較高,病例選擇偏倚風險較高;耐氟喹諾酮類合并靈敏度、特異度和AUC分別為0.87、0.97和0.9690;耐阿米卡星分別為0.87、1.00和0.9944;耐卷曲霉素分別為0.88、0.97和0.9791;耐卡那霉素分別為0.50、0.99和0.9814;耐乙胺丁醇分別為0.69、0.87和0.7349,除耐阿米卡星特異度分布差異無統計學意義外(P>0.05),其它均有統計學意義(P<0.01)。Genotype MTBDRsl技術檢測不同樣本耐二線藥的敏感度和特異度無統計學差異(P>0.05)。各研究不存在發表偏倚。結論:Genotype MTBDRsl技術在耐氟喹諾酮類,阿米卡星與卷曲霉素研究中具有較高診斷價值,但對耐卡那霉素和乙胺丁醇的診斷效能有待進一步提高。
【關鍵詞】耐多藥結核病快速診斷技術;二線藥;結核菌;Meta分析
目前,結核病仍是威脅全球公共衛生安全的嚴重疾病之一,在我國的流行與傳播更不容樂觀,耐多藥結核病(Multi-Drug Resistant Tuberculosis,MDR-TB)是導致疫情居高不下的重要原因[1],成為結核病防控難題。研究常用二線抗結核藥物氟喹諾酮類、阿米卡星、卷曲霉素、卡那霉素和乙胺丁醇對多耐藥、耐多藥、泛耐藥結核分枝桿菌感染的防治有極其重要的作用。由于傳統藥敏試驗耗時耗力[2],給臨床早期治療與診斷帶來諸多困難,采用分子生物學方法快速檢測抗結核二線藥耐藥基因突變,快速報告結核臨床株耐藥情況受到臨床歡迎。本文Meta分析國外使用耐多藥結核病快速診斷技術(Genotype MTBDRsl)對耐二線藥結核菌診斷效能,進一步評價臨床應用價值。
1資料與方法
1.1檢索方法
檢索策略采用主題詞與自由詞結合,并根據具體數據庫調整檢索方法。為了減少漏查文獻,由兩名評價員單獨檢索并對納入研究的參考文獻進行再次檢索。計算機檢索Pubmed、Embase和Cochrane圖書館數據庫。檢索年限從建庫至2015-01。檢索語種為英語,檢索詞為“Genotype MTBDRsl” and “Tuberculosis” or “TB” or “TB Infection” or “TB Disease” or “Mycobacterium tuberculosis” or “Mycobacterium tuberculosis complex”。
1.2納入和排除標準
納入標準:(1)所有研究均以藥敏結果作為“金標準”;(2)研究對象均應用Genotype MTBDRsl技術診斷耐二線藥結核菌;(3)納入研究的Genotype MTBDRsl檢測和“金標準”檢查的間隔時間不超過一個月;(4)納入文獻原始數據能夠直接或間接計算出真、假陽性率等。
排除標準:(1)未使用Genotype MTBDRsl技術診斷耐二線藥結核菌文獻;(2)述評、文摘、講座和綜述等二次文獻。
1.3質量評價
由兩位評價者單獨評價所納入文獻質量,當意見不一致時討論解決。根據QUADAS-2條目[3]進行質量評價,每個研究逐條按照“是”、“否”、“不清楚”進行評價。“是”為滿足該條目標準,“否”為不滿足標準或文中未提及該標準,“不清楚”表示部分滿足標準或者無法從該文獻中得到充足的資料。
1.4統計學處理
使用MetaDisc 1.4和Stata 13.0軟件進行數據分析。如I2>50%,提示異質性較高,則采用隨機效應模型(D-L法)進行Meta分析;I2≤50%采用固定效應模型(M-H法)進行Meta分析。計算耐藥真陽性值(True Resistance, TR)、真陰性值(True Susceptibility, TS)、假陽性值(False Resistance, FR)、假陰性值(False Susceptibility, FS),分析檢測技術的靈敏度、特異度,陽性似然比(Positive Likelihood Ratio, PLR)、陰性似然比(Negative Likelihood Ratio,NLR)、診斷比值比(Diagnostic Odds Ratio,DOR)以及95%可信區間(Confidence Interval,CI),然后建立受檢者工作特征曲線(Summary Receiver Operating Curve,SROC),并計算曲線下面積(AUC)以及Q值評估診斷價值。并分析檢測技術對不同類型樣本(臨床樣本和培養株)的靈敏度和特異度。通過Begg’s值定量分析發表偏倚。
2結果
2.1入選文獻特征
預檢出43篇英文文獻,根據納入標準和排除標準,審讀各文獻摘要后篩選得到25篇文獻,最后通讀全文納入19篇文獻[4-22],6篇為檢測臨床樣本[4, 10, 11, 15, 16, 22]、13篇為檢測臨床培養株[5-9, 12-14, 17-21],其中3篇檢測了兩種樣本[4,10,11],因此后文按納入22篇文獻進行分析。其基本特征見表1。

表1 納入文獻的基本特征
注:NA為不清楚
2.2納入研究的質量評價
QUADAS-2 工具包括4項內容(圖1A):病例選擇、待評價試驗、金標準和病例進展情況,用于評估偏倚風險;臨床適用性評估不包括病例進展情況。納入研究的偏倚風險和臨床適用性評估結果為:病例選擇和病例進展情況有較高偏倚風險,而待評價試驗和金標準的偏倚風險較低。見表2和圖1B。
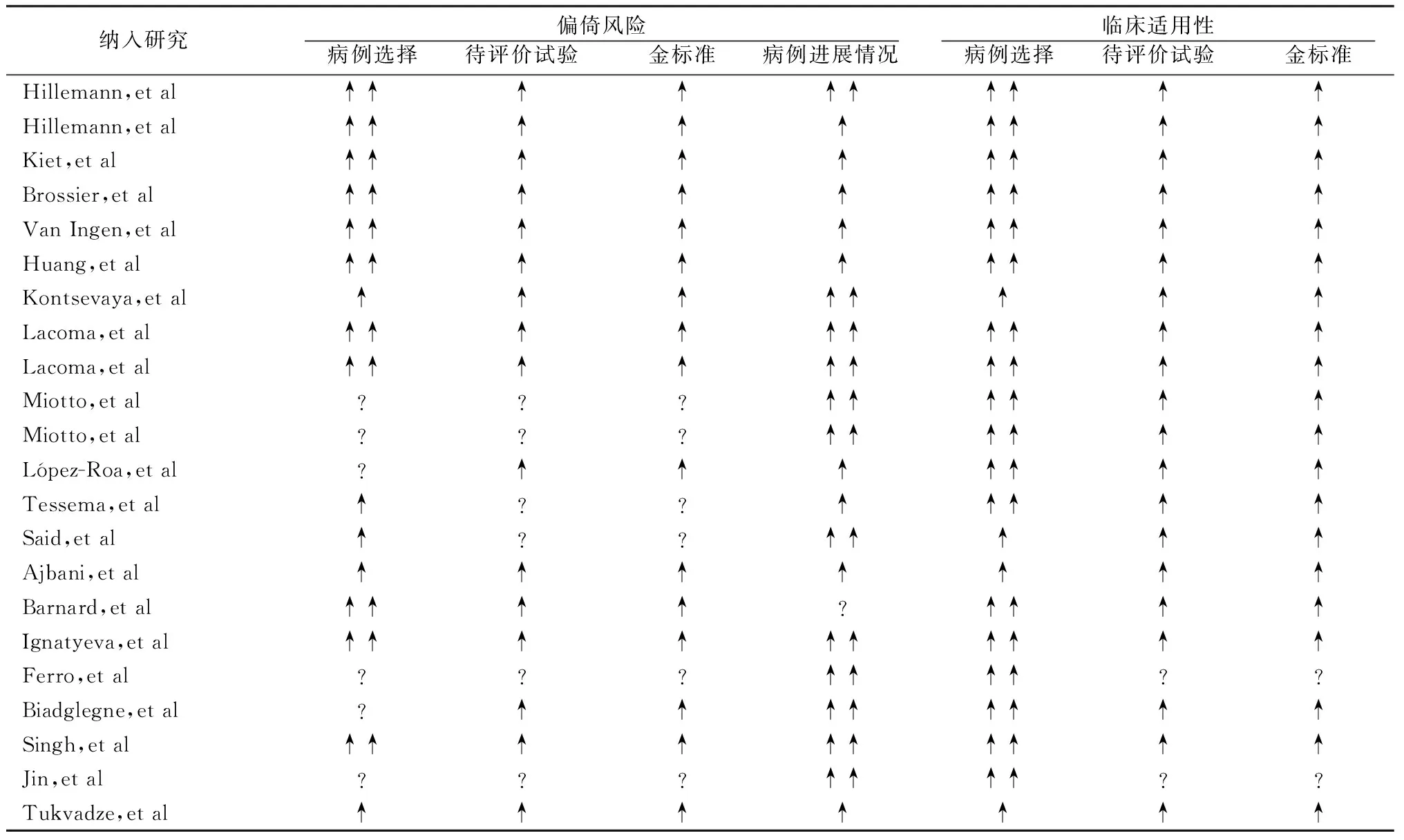
表2 納入文獻質量評價
注:“↑”為低風險;“↑↑”為高風險;“?”為不清楚
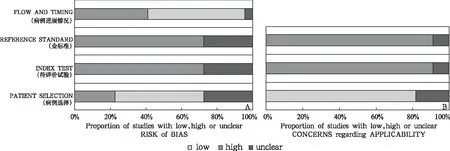
圖1 文獻質量評價結果
2.3Meta分析
2.3.1異質性分析:應用MetaDisc 1.4軟件分析所有納入研究耐氟喹諾酮類、阿米卡星、卷曲霉素、卡那霉素及乙胺丁醇數據的靈敏度差異均有統計學意義(χ2值分別為58.39、30.59、33.03、111.14、94.37,P<0.01),特異度除耐阿米卡星(χ2=11.49,P>0.05)外,其它差異均有統計學意義(χ2值分別為68.64、25.76、40.77、368.19,P<0.01);同時只有耐阿米卡星I2<50%,其余I2≥50%;提示整體研究的異質性較高。通過TR、TS、FR、FS計算的各研究采用Genotype MTBDRsl技術診斷耐二線抗結核藥的靈敏度和特異度見圖2。

注:圖中橫線長短表示95%可信區間范圍的大小,線條中間大小各異的圓點表示靈敏度、特異度值的位置,圓點的大小為
2.3.2SROC的AUC分析:如圖3,耐氟喹諾酮類、阿米卡星、卷曲霉素、卡那霉素和乙胺丁醇AUC分別為0.9690、0.9944、0.9791、0.9814和0.7349,Q值分別為0.9182、0.9707、0.9356、0.9398和0.6810。即耐乙胺丁醇AUC最小,診斷敏感度和特異度最低。
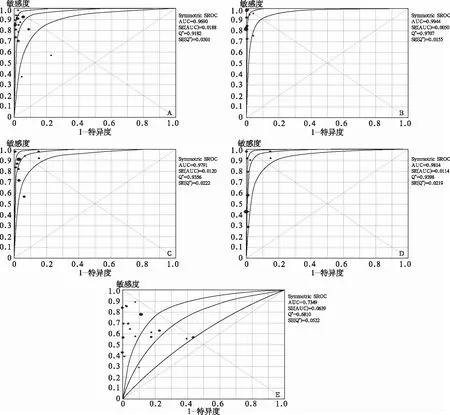
注:圖A、B、C、D、E分別為耐氟喹諾酮類、阿米卡星、卷曲霉素、卡那霉素和乙胺丁醇SROC曲線
2.3.3不同類型樣本耐二線藥效能分析:采用Genotype MTBDRsl檢測兩種類型樣本耐氟喹諾酮類、阿米卡星、卷曲霉素、卡那霉素和乙胺丁醇的特異度均高于0.94,敏感度除耐卡那霉素較低(0.44-0.67),其它均高于0.75。其中耐氟喹諾酮類、阿米卡星和卡那霉素以臨床樣本檢測的靈敏度較高,耐卷曲霉素以培養株檢測的敏感度較高;耐氟喹諾酮類特異度以臨床樣本較高,而耐阿米卡星、卷曲霉素和卡那霉素的特異度以培養株較高,但差異均無統計學意義(P>0.05)。見表3。
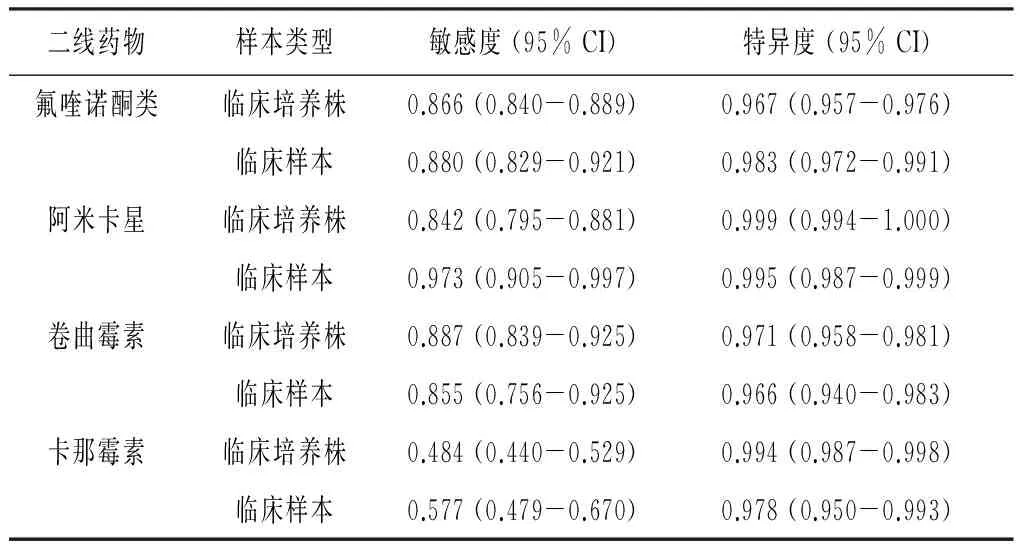
表3 兩種樣本耐二線藥敏感度和特異度分析
2.3.4發表偏倚:使用Stata 13.0軟件計算耐氟喹諾酮類、阿米卡星、卷曲霉素、卡那霉素和乙胺丁醇Begg’s值分別為0.43、-2.02、-0.42、0.18和0.49,對應P值均>0.05,表明各研究不存在明顯發表偏倚。
3討論
Genotype MTBDRsl技術來自德國Hain Lifescience公司,用于結核分枝桿菌對二線藥物的耐藥性檢測,其原理是應用多重PCR結合反向雜交技術,與固定在硝化纖維膜條帶上的特異耐藥基因進行雜交后,根據顯色條帶判讀耐藥性及耐藥突變位點,可在6h內獲得結果,實現了結核分枝桿菌耐藥性的快速檢測。但該技術的應用評價不盡一致。循證醫學方法可通過綜合小樣本數據,達到擴大樣本量、減少抽樣誤差,增加分析結果的可靠性。本文通過選擇較高質量文獻Meta分析Genotype MTBDRsl技術診斷耐二線藥結核菌的臨床價值。
臨床診斷性試驗廣泛使用QUADAS-2條目進行文獻質量評估,主要從偏倚風險與臨床適用性兩方面評價異質性和偏倚的產生。偏倚風險包括病例選擇、待評價試驗、金標準、疾病進展情況,而臨床適用性主要由前三者組成。本文納入研究的偏倚風險包括:(1)病例選擇偏倚,只有22.7%的研究為低風險,50.0%為高風險,這可能由于沒有連續或隨機納入病例所致;(2)待評價試驗偏倚,72.7%的研究為低風險,未出現高風險,說明大部分納入研究的結果判讀是在不知曉金標準試驗結果的情況下進行的;(3)金標準偏倚,與待評價試驗偏倚風險一樣,72.7%文獻為低風險,未出現高風險,說明大部分研究的診斷金標準可以正確區分是否耐二線結核藥以及金標準結果判讀采用了盲法;(4)疾病進展偏倚,54.5%的研究為高風險,提示不是所有病例都被納入分析。臨床適用性偏倚分析顯示,81.8%的研究存在病例選擇高風險,待評價試驗與金標準不存在高風險。
本Meta分析表明,Genotype MTBDRsl技術除了診斷耐阿米卡星合并特異度不存在明顯異質性外,其它耐二線藥合并靈敏度和特異度均存在較大的異質性。異質性來源主要有:(1)Genotype MTBDRsl技術所檢測樣本類型不同;(2)納入研究受試者來自不同國家、種族,其生活狀況、疾病發生率等均有差異;(3)納入研究受試者結核治療方式、治療時間長短不一;(4)檢測人員經驗與技術水平存在差異。本研究還表明Genotype MTBDRsl技術診斷耐氟喹諾酮類、阿米卡星、卷曲霉素、卡那霉素SROC的AUC和Q值均大于0.90,而耐乙胺丁醇SROC的AUC及Q值僅在0.70左右,提示Genotype MTBDRsl技術用于診斷耐乙胺丁醇結核菌不是一種很好的選擇。Genotype MTBDRsl技術診斷耐卡那霉素及乙胺丁醇的合并靈敏度分別為0.50(95%CI 0.46-0.54)和0.69(95%CI 0.66-0.71),明顯低于其它耐二線藥的合并靈敏度(>0.80),這可能導致耐卡那霉素與乙胺丁醇結核菌漏診;而且,Genotype MTBDRsl技術診斷耐乙胺丁醇的合并特異度也較低(0.87),有可能將乙胺丁醇敏感結核菌診斷為耐乙胺丁醇結核菌,引起誤診。本文根據樣本類型分析了Genotype MTBDRsl技術對耐二線藥的靈敏度和特異度,結果表明,臨床樣本和培養株樣本類型不會影響Genotype MTBDRsl技術的診斷價值。但考慮本文納入研究中只有6篇文獻采用了臨床樣本,這可能缺乏說服力,需要納入更多臨床樣本研究來進一步驗證上述結論。Begg’s檢驗未發現本文納入的各研究間存在顯著發表偏倚,提示文獻質量較高,結果具有一定的可信度。
本研究存在以下局限:各研究間樣本數量差異較大,相關分析時可能得出假陽性結果;檢索策略中雖然使用多種方法提高檢索的全面性,但依然可能由于檢索不全面而漏檢一些有價值的文獻;另外,納入文獻中只有6篇為臨床樣本,其余均為培養株樣本,可能會導致各研究間檢測價值差異較大。
綜上所述,Genotype MTBDRsl技術診斷耐氟喹諾酮類、阿米卡星、卷曲霉素結核菌敏感度和特異度較高,但對耐卡那霉素和乙胺丁醇藥診斷價值還需進一步提高。同時還需納入更多針對臨床樣本檢測的研究來進一步評估Genotype MTBDRsl技術檢測臨床樣本的診斷價值。
?
馬峻(1971-),男,漢族,主管技師,主要從事結核菌耐藥機制及分子診斷研究
參考文獻
1Abubakar I, Zignol M, Falzon D, et al. Drug-resistant tuberculosis: time for visionary political leadership[J]. Lancet Infect Dis, 2013, 13(6):529-539.
2Garrigo M, Aragon LM, Alcaide F, et al. Multicenter laboratory evaluation of the MB/BacT Mycobacterium detection system and the BACTEC MGIT 960 system in comparison with the BACTEC 460TB system for susceptibility testing of Mycobacterium tuberculosis[J]. J Clin Microbiol, 2007, 45(6):1 766-1 770.
3Whiting PF, Rutjes AW, Westwood ME, et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies[J]. Ann Intern Med, 2011, 155(8):529-536.
4Hillemann D, Rusch-Gerdes S, Richter E. Feasibility of the GenoType MTBDRsl assay for fluoroquinolone, amikacin-capreomycin, and ethambutol resistance testing of Mycobacterium tuberculosis strains and clinical specimens[J]. J Clin Microbiol, 2009, 47(6):1 767-1 772.
5Kiet VS, Lan NT, An DD, et al. Evaluation of the MTBDRsl test for detection of second-line-drug resistance in Mycobacterium tuberculosis[J]. J Clin Microbiol, 2010, 48(8):2 934-2 939.
6Brossier F, Veziris N, Aubry A, et al. Detection by GenoType MTBDRsl test of complex mechanisms of resistance to second-line drugs and ethambutol in multidrug-resistant Mycobacterium tuberculosis complex isolates[J]. J Clin Microbiol, 2010, 48(5):1 683-1 689.
7van Ingen J, Simons S, de Zwaan R, et al. Comparative study on genotypic and phenotypic second-line drug resistance testing of Mycobacterium tuberculosis complex isolates[J]. J Clin Microbiol, 2010, 48(8):2 749-2 753.
8Huang WL, Chi TL, Wu MH, et al. Performance assessment of the GenoType MTBDRsl test and DNA sequencing for detection of second-line and ethambutol drug resistance among patients infected with multidrug-resistant Mycobacterium tuberculosis[J]. J Clin Microbiol, 2011, 49(7):2 502-2 508.
9Kontsevaya I, Mironova S, Nikolayevskyy V, et al. Evaluation of two molecular assays for rapid detection of mycobacterium tuberculosis resistance to fluoroquinolones in high-tuberculosis and -multidrug-resistance settings[J]. J Clin Microbiol, 2011, 49(8):2 832-2 837.
10Lacoma A, Garcia-Sierra N, Prat C, et al. GenoType MTBDRsl for molecular detection of second-line-drug and ethambutol resistance in Mycobacterium tuberculosis strains and clinical samples[J]. J Clin Microbiol, 2012, 50(1):30-36.
11Miotto P, Cabibbe AM, Mantegani P, et al. GenoType MTBDRsl performance on clinical samples with diverse genetic background[J]. Eur Respir J, 2012, 40(3):690-698.
12Lopez-Roa P, Ruiz-Serrano MJ, Alcala L, et al. Susceptibility testing to second-line drugs and ethambutol by GenoType MTBDRsl and Bactec MGIT 960 comparing with agar proportion method[J]. Tuberculosis, 2012, 92(5):417-421.
13Tessema B, Beer J, Emmrich F, et al. First- and second-line anti-tuberculosis drug resistance in Northwest Ethiopia[J]. Int J Tuberc Lung Dis, 2012, 16(6):805-811.
14Said HM, Kock MM, Ismail NA, et al. Evaluation of the GenoType(R) MTBDRsl assay for susceptibility testing of second-line anti-tuberculosis drugs[J]. Int J Tuberc Lung Dis, 2012, 16(1):104-109.
15Ajbani K, Nikam C, Kazi M, et al. Evaluation of genotype MTBDRsl assay to detect drug resistance associated with fluoroquinolones, aminoglycosides and ethambutol on clinical sediments[J]. PLoS One, 2012, 7(11):e49433.
16Barnard M, Warren R, Gey Van Pittius N, et al. Genotype MTBDRsl line probe assay shortens time to diagnosis of extensively drug-resistant tuberculosis in a high-throughput diagnostic laboratory[J]. Am J Respir Crit Care Med, 2012, 186(12):1 298-1 305.
17Ignatyeva O, Kontsevaya I, Kovalyov A, et al. Detection of resistance to second-line antituberculosis drugs by use of the genotype MTBDRsl assay: a multicenter evaluation and feasibility study[J]. J Clin Microbiol, 2012, 50(5):1 593-1 597.
18Ferro BE, Garcia PK, Nieto LM, et al. Predictive value of molecular drug resistance testing of Mycobacterium tuberculosis isolates in Valle del Cauca, Colombia[J]. J Clin Microbiol, 2013, 51(7):2 220-2 224.
19Biadglegne F, Tessema B, Rodloff AC, et al. Magnitude of gene mutations conferring drug resistance in mycobacterium tuberculosis isolates from lymph node aspirates in ethiopia[J]. Int J Med Sci, 2013, 10(11):1 589-1 594.
20Singh AK, Maurya AK, Kant S, et al. Rapid detection of drug resistance and mutational patterns of extensively drug-resistant strains by a novel GenoType(R) MTBDRsl assay[J]. J Postgrad Med, 2013, 59(3):179-185.
21Jin J, Shen Y, Fan X, et al. Underestimation of the resistance of Mycobacterium tuberculosis to second-line drugs by the new GenoType MTBDRsl test[J]. J Mol Diagn, 2013, 15(1):44-50.
22Tukvadze N, Bablishvili N, Apsindzelashvili R, et al. Performance of the MTBDRsl assay in Georgia[J]. Int J Tuberc Lung Dis, 2014, 18(2):233-239.
The Diagnosis of Mycobacterium Tuberculosis Resistant to Second-Line Drugs with Genotype MTBDRsl Assay: A Meta-Analysis*
MA Jun1, GUO Yi2,#
1Department of Clinical Laboratory, Wuhan Medical Treatment Center, Wuhan 430000, China;2Department of Epidemiology, Wuhan University School of Public Health, Wuhan 430071, China;#Corresponding author
【Abstract】Objective: To investigate the clinical value of multi-drug resistant tuberculosis(MDR-TB) rapid diagnostic technique genotype MTBDRsl assay in diagnosing mycobacterium tuberculosis resistant to second-line drugs with meta-analysis. Method: We searched Pubmed, Embase and the Cochrane Librar until January 2015. The Meta-Disc software was used to calculate sensitivity, specificity, positive likelihood ratio (PLR), negative likelihood ratio (NLR), diagnostic odds ratio (DOR), corresponding 95% confidence interval (CI), as well as summary receiver operating curve (SROC). The diagnosis value of MTBDRsl assay was evaluated by area under the curve (AUC), and compare the sensitivity and specificity between clinical samples and culture strains. meanwhile we assess the publish bias of included studies.Results: We identified 22 English literatures involving five different drugs (fluoroquinolones, amikacin, capreomycin, kanamycin and ethambutol). The overall heterogeneity of study was high, and the risk of selection bias was higher. The summarized sensitivity, specificity, and AUC were 0.87, 0.97 and 0.9690 for fluoroquinolones, 0.87, 1.00 and 0.9944 for amikacin, 0.88, 0.97 and 0.9791 for capreomycin, 0.50, 0.99 and 0.9814 for kanamycin and 0.67, 0.87 and 0.7349 for ethambutol, respectively. In addition to the specificity of amikacin resistance had no significant difference (P> 0.05), others were statistically significant (P<0.01). The sensitivity and specificity of different samples had no statistical significance (P>0.05). There were no publish bias in all included studies.Conclusion: Genotype MTBDRsl demonstrate excellent accuracy for detecting drug resistance to fluoroquinolones, amikacin and capreomycin, but it may not be an appropriate choice for kanamycin and ethambutol.
【Key words】Genotype MTBDRsl; Second-line drugs; Mycobacterium tuberculosis; Meta-analysis
*[基金項目]武漢市衛生局臨床醫學科研項目(WX12C02)
[中圖分類號]R446.5
[文獻標識碼]A
[文章編號]1005-1740(2016)02-0031-08
第一作者簡介:本文
本文2015-11-25收到,2016-04-14修回
猜你喜歡
體育科技文獻通報(2022年3期)2022-05-23 13:46:54
天津外國語大學學報(2021年3期)2021-08-13 08:32:18
遼金歷史與考古(2021年0期)2021-07-29 01:06:54
科技傳播(2019年22期)2020-01-14 03:06:54
遼金歷史與考古(2019年0期)2020-01-06 07:45:20
民用飛機設計與研究(2019年4期)2019-05-21 07:21:24
電子制作(2018年11期)2018-08-04 03:26:04
汽車工程學報(2017年2期)2017-07-05 08:13:02
國際商務財會(2017年8期)2017-06-21 06:14:14
電子制作(2017年23期)2017-02-02 07:17:19