體素內不相干運動對前列腺癌和前列腺增生結節的鑒別診斷
2016-11-19 03:20:15孫美玉劉愛連李燁陳麗華宋清偉徐斌
放射學實踐 2016年10期
孫美玉, 劉愛連, 李燁, 陳麗華, 宋清偉, 徐斌
?
·腹部影像學·
體素內不相干運動對前列腺癌和前列腺增生結節的鑒別診斷
孫美玉, 劉愛連, 李燁, 陳麗華, 宋清偉, 徐斌
目的:分析前列腺癌(PCa)和前列腺增生(BPH)的體素內不相干運動(IVIM)參數,旨在評價IVIM對PCa和BPH的鑒別診斷價值。方法:回顧性分析72例經病理證實PCa(n=32)和BPH(n=40)患者的3.0T MR圖像,掃描序列包括常規T2WI、DWI、LAVA平掃及動態增強和IVIM。IVIM成像,掃描采用EPI-STIR序列,b值=0、20、50、100、200、400、600、800、1000和1200 s/mm2。利用GE Functool 4.5工作站的MADC軟件,測量PCa和BPH組的標準ADC、慢ADC、快ADC和快ADC分數值,PCa和BPH組的各參數比較采用獨立樣本t檢驗。采用受試者工作曲線(ROC)分析標準ADC值、慢ADC值對PCa和BPH的鑒別效能,獲得相應曲線下面積(AUC)、診斷PCa的閾值以及相應靈敏度、特異度、陽性預測值(PPV)、陰性預測值(NPV)和準確度。結果:PCa的標準ADC值和慢ADC值分別為(6.21±2.35)×10-4和(7.11±2.49)×10-4mm2/s,BPH的標準ADC值和慢ADC值分別為(11.11±2.62)×10-4和(12.65±1.81)×10-4mm2/s,PCa者明顯低于BPH者,二者之間的差異具有統計學意義。PCa和BPH的快ADC值和快ADC值分數之間的差異無統計學意義。標準ADC值、慢ADC值AUC分別為0.912和0.947。以8.325×10-4mm2/s作為標準ADC值的閾值,其診斷PCa的敏感度為78.13%,特異度為97.50%,PPV為96.15%,NPV為84.78%,準確率為88.89%。以10.03×10-4mm2/s作為慢ADC值的閾值,其診斷PCa的敏感度為87.50%,特異度為95.00%,PPV為93.33%,NPV為90.48%,準確率為91.67%。結論:IVIM的定量參數標準ADC和慢ADC值對PCa和BPH鑒別診斷效能好,可作為前列腺增生基礎上PCa檢出良好的指標。
前列腺腫瘤; 前列腺增生; 磁共振成像
目前臨床上診斷前列腺癌(prostate cancer,PCa)的金標準是經直腸前列腺穿刺活檢或術后病理,但對臨床疑似的PCa患者,假陰性率高達66%~71%。中老年男性,PCa和良性前列腺增生(benign prostatic hyperplasia,BPH)常合并存在,但二者治療方案和臨床預后完全不同[1,2]。部分PCa和BPH的臨床表現、實驗室檢查(PSA水平)存在重疊,常規MR影像鑒別診斷亦存在困擾[3,4]。
磁共振擴散加權成像(diffusion weighted imaging,DWI)獲得的ADC圖在Pca和BPH的診斷和鑒別診斷中發揮重要作用[5]。常規DWI上PCa與BPH相比,因細胞外間隙減小、彌散受限而表現為高信號,ADC圖呈低信號;但既往的一些研究[6-8]顯示以高斯彌散為數學模型(單指數)計算的ADC值受不同b值選擇的影響。體素內不相干運動(intra-voxel incoherent motion,IVIM)MR成像除了考慮分子熱運動所致的分子擴散外,還考慮到基于灌注的假彌散[9],無需對比劑,可無創檢測并提取活體組織的擴散(高b值)和灌注(低b值)信息,反映疾病的病理生理改變[9,10]。既往的研究多集中在Pca和正常前列腺組織之間的IVIMMR成像的差別[11-15],對PCa和BPH的IVIM參數的對比研究鮮見。本研究通過對PCa和BPH的IVIM成像及參數分析,旨在評價IVIM成像參數對PCa和BPH的鑒別診斷價值。
材料與方法
1.臨床資料
該研究獲得大連醫科大學附屬第一醫院倫理委員會核準并免除患者的知情同意。回顧性分析我院2012年11月-2015年7月行前列腺MRI檢查且進行手術確診為PCa和BPH男性患者,納入標準為:①能配合MRI檢查,前列腺成像清晰;②患者在完成MRI檢查后一個月內進行超聲引導下經直腸前列腺穿刺活檢或前列腺切除手術病理證實。排除標準:①MRI檢查前進行過活檢或相關治療者;②既往前列腺手術者;③腸道偽影重,圖像質量影響分析者。最后共納入72例,其中PCa組32例,年齡53~88歲,平均年齡71.41歲;BPH組40例,年齡51~90歲,平均年齡68.73歲。
2.成像方法
采用GE Signa 3.0T磁共振掃描儀,梯度場強40 mT·m,切換率為150 T/ms。患者仰臥位,以體線圈為射頻發射線圈,8通道腹部相控陣線圈為接收線圈。檢查前患者適量飲水,膀胱中度充盈,防止過度充盈引起波動偽影及檢查時間過長致患者無法耐受。盆腔置于線圈內,線圈中心對恥骨聯合上緣,采用橫斷面掃描,包括前列腺及精囊腺。
T2WI序列參數:TR 3820 ms,TE 140 ms,層厚4 mm,層間距2 mm,視野30×30,矩陣320×224,激勵次數4;DWI序列參數:TR 3575 ms,TE 87 ms,b=0,1000 s/mm2,層厚5 mm,層間距1 mm,視野30×30,矩陣128×128,激勵次數8。LAVA動態增強序列參數:TR 3 ms,TE 2 ms,層厚5.2 mm,層間距1.3 mm,矩陣288×180,視野38×30,連續掃描30個期相; IVIM-MR成像具體參數:橫斷面二維掃描,平面回波成像-短時反轉恢復(echo planar imaging-short time inversion recovery,EPI-STIR)序列;TR 3000 ms,TE 86 ms,翻轉角90°,視野40 cm×40 cm,層厚5 mm,層間距1 mm,矩陣96×128,激勵次數8,方向:所有,b值范圍0~1200 s/mm2,分別為b=0、20、50、100、200、400、600、800、1000和1200 s/mm2,掃描時間240 s。
3.病理學檢查及圖像后處理
72例患者前列腺穿刺、部分或全部切除術后標本由兩位(分別有12年和7年前列腺疾病診斷經驗)病理醫生對病變進行定位和診斷,他們在病理診斷前不知曉MRI檢查結果。
IVIM成像一次掃描獲得b值0~1200 s/mm2的10組圖像,利用GE Functool 4.5工作站的MADC軟件,由2位前列腺MRI讀片經驗分別為14年和6年的放射科醫師對MR圖像分別進行評估和測量,確定每例PCa和BPH病灶的區域。PCa組癌區為T2WI抑脂序列呈低信號、DWI呈高信號和/或增強掃描明顯強化且病理結果為前列腺癌的區域,如果有多個病灶,則選取最大的病灶入組進行測量。BPH組結節性增生者,感興趣區(region of interest,ROI)覆蓋結節 2/3 以上,彌漫性增生者,于中央腺體區(CZ)選取 ROI 進行測量,ROI大小約為50~70 mm2,ROI位于病灶的實性部分,盡量避開囊變、尿道區域,每次測量繪制3個大小相等的ROI,分別測量并記錄IVIM的標準表觀彌散系數(apparent diffusion coefficient,ADC)值、慢ADC、快ADC和快ADC分數,取3次測量值的平均值用于統計學分析。
4.統計學方法
分別記錄兩位觀察者測量的PCa和BPH的標準ADC、慢ADC、快ADC和快ADC分數,用均數±標準差的方式表示,使用組內相關系數(intra-class correlation coefficients,ICC)檢驗兩觀察者測量數據的一致性(ICC值>0.75為一致性很好,ICC在0.5~0.75為一致性良好,<0.5為一致性很差)。選擇標準差小的數據進行下一步的統計分析。應用SPSS 17.0軟件對相應數據進行獨立樣本的t檢驗,P<0.05為差異有統計學意義,使用受試者工作特征曲線(receiver operating characteristic curve,ROC)分析標準ADC值、慢ADC值、快ADC值和快ADC分數對PCa和BPH的鑒別效能,獲得相應曲線下面積(area under the curve,AUC)(AUC>0.9為診斷效能高、AUC介于0.7~0.9為診斷效能中等,AUC介于0.5~0.7為診斷效能低),利用約登指數最大原則,對診斷效能高的參數診斷PCa的閾值以及相應靈敏度、特異度、陽性預測值(positive predictive value,PPV)、陰性預測值(negative predictive value,NPV)和準確度。

表1 PCa和BPH 組ADC值(mm2/s)

表2 標準ADC值及慢ADC值診斷閾值、敏感度、特異度、PPV、NPV及準確率
結 果
1.兩位觀察者之間定量數據比較
兩觀察者所測量標準ADC值、慢ADC值、快ADC值和快ADC分數的ICC值分別為:0.915、0.937、0.853及0.770,一致性均良好。使用標準差較小的數據進行以下比較。
2.PCa和BPH的IVIM參數比較
PCa組的標準ADC值、慢ADC值明顯低于BPH組,二者之間的差異有統計學意義。PCa組的快ADC值及快ADC分數與BPH組之間無顯著性差異(表1、圖1~6)。
3.ROC曲線分析
PCa組和BPH組的標準ADC值、慢ADC值、快ADC值和快ADC分數的ROC曲線見圖7,其中標準ADC值、慢ADC值、快ADC值和快ADC值分數的AUC分別為0.912、0.947、0.504和0.706(表1),其中標準ADC值和慢ADC值的診斷效能高,快ADC值的診斷效能低,而快ADC值分數的診斷效能中等。以8.325×10-4mm2/s作為標準ADC值的閾值,其診斷PCa的敏感度為78.13%,特異度為97.50%,陽性預測值為96.15%,陰性預測值為84.78%,準確率為88.89%。以10.03×10-4mm2/s作為慢ADC值的閾值,其診斷PCa的敏感度為87.50%,特異度為95.00%,陽性預測值為93.33%,陰性預測值為90.48%,準確率為91.67%(表2)。
討 論
臨床上Pca常發生在有BPH基礎的前列腺內,中老年男性多見,多需穿刺活檢確診,該方法有較高的假陰性[16],同時會引起疼痛、出血等并發癥,因不能多次重復進行而使部分患者無法接受。
在生物組織內,DWI檢測到的微觀運動既包括水分子的彌散,還包括組織結構成分的影響以及毛細血管網的微循環(灌注),傳統的單指數模型忽略了低b值時微灌注造成的快速的信號衰減,使得測得的ADC值受b值的影響[17]。在前列腺組織中,由于細胞內屏障,如細胞膜和細胞器分隔的存在,導致高b值時并不符合Gaussian單指數彌散特點[18,19]。IVIM成像技術通過將DWI技術采集的水分子彌散數據進行雙指數模型的后處理分析,提取彌散系數和灌注分數,在無需對比劑的條件下對病變的灌注和彌散信息進行評估[19-21]。
本組研究中PCa標準ADC值和慢ADC值分別為(6.21±2.35)×10-4和(7.11±2.49)×10-4mm2/s,BPH的標準ADC值和慢ADC值分別為(11.11±2.62)×10-4和(12.65±1.81)×10-4mm2/s,PCa者明顯低于BPH者,與既往對PCa的研究結果[13,17,20,21]相一致,即PCa的ADC值明顯減低。前列腺腫瘤與良性組織相比,擴散系數減低,在病理學上,PCa細胞排列緊密,腺管及腺泡結構紊亂或消失,水分子彌散明顯受限,ADC值顯著下降;BPH中腺管和腺泡的增生可伴有分泌物增多,彌散相對不受限而表現為相對高的ADC值。慢ADC反映的是組織在高b值時組織的彌散特性,減少了低b值條件下灌注對彌散的影響,更能反映組織的彌散特點。本組研究中慢ADC值診斷前列腺癌AUC為0.947,較標準ADC值的AUC(0.912)略高,二者均體現良好的診斷效能,以8.325×10-4mm2/s為標準ADC值的閾值,其診斷PCa的特異度為97.50%,PPV為96.15%,準確率為88.89%。以10.03×10-4mm2/s為慢ADC值的閾值,其診斷PCa的特異度為95.00%,PPV為93.33%,NPV為90.48%,準確率為91.67%。
本組研究中PCa的快ADC值(D*-假彌散系數)為(12.97±11.27)×10-3mm2/s,較BPH者增高,但二者之間的差異無統計學意義。雖然對前列腺癌DCE-MRI的研究[22,23]表明前列腺癌與正常前列腺組織相比有著更高的血流量,但我們的結果與Kuru等[24]的研究結果相似,即PCa與非癌組織的快ADC值無顯著性差異,分析可能與BPH亦會改變組織的灌注,而且不同的增生程度可能對灌注的影響亦不同[25]有關。本組研究中PCa的快ADC分數(f-灌注分數)與BPH者無顯著性差異;既往對PCa快ADC值分數的研究得到不同的結果。PCa組織血供豐富,其內的微血管密度、血流量和血管通透性等血流灌注指標高于非癌組織,而快ADC值分數體現的是病灶的灌注因素對總擴散的影響比例,有學者[26-28]研究認為b<200s/mm2時能更好的體現f值的差異,本組研究中的低b值選擇為0、20、50、100、200s/mm2,數值間隔范圍略大,可能使灌注因素的體現受到一定的影響。Kuru等[24]的研究b值選擇為0、50、100、150、200、250和800s/mm2,其結果與我們的結果相一致。部分學者[29,30]分析認為快ADC分數除了反映微血管內水分子假隨機運動呈現的血容量,可能還與腔室的橫向弛豫時間及其它的大分子(如腺體分泌和導管內液體)流動有關。
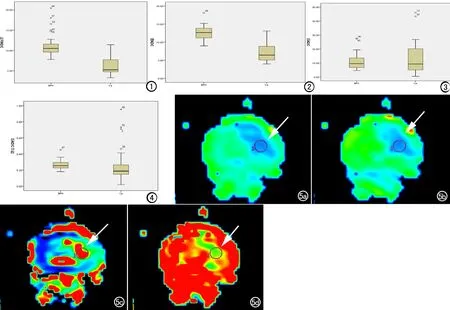
圖1 PCa組和BPH組的標準ADC值箱式圖。
圖2 PCa組和BPH組的慢ADC值箱式圖。
圖3 PCa組和BPH組的快ADC值箱式圖。
圖4 PCa組和BPH組的快ADC值分數箱式圖。
圖5 患者,男,72歲,前列腺癌(Gleason3+4,箭)。a) 標準ADC為4.82×10-4mm2/s; b) 慢ADC為4.94×10-4mm2/s; c) 快ADC為19.6 ×10-3mm2/s; d) 快ADC分數為0.243。
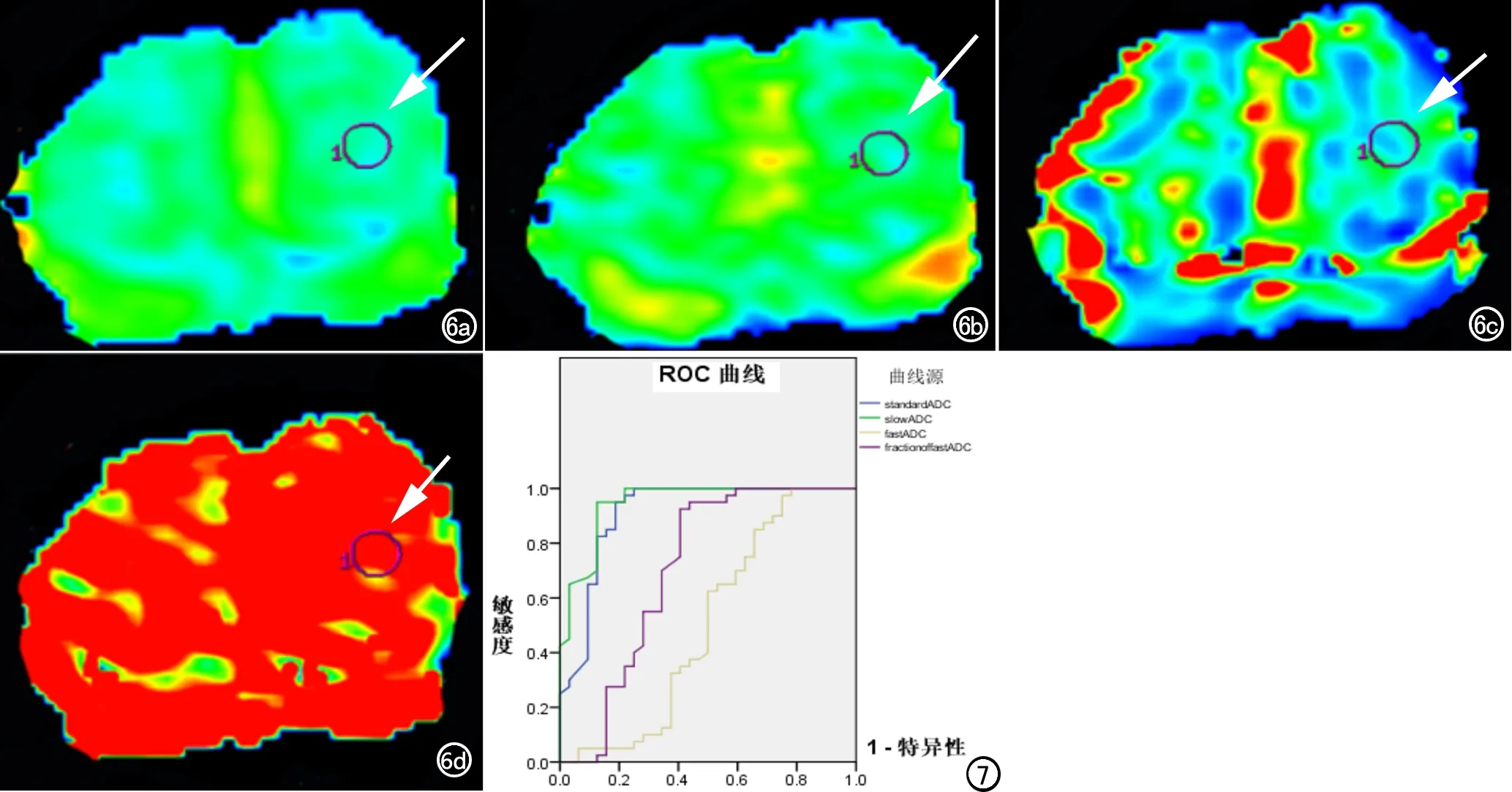
圖6 患者,男,64歲,良性前列腺增生(箭)。a) 標準ADC為9.74×10-4mm2/s; b) 慢ADC為10.55×10-4mm2/s; c) 快ADC為7.95×10-3mm2/s; d) 快ADC分數為 0.307。 圖7 PCa組和BPH組的標準ADC、慢ADC、快ADC和快ADC分數的ROC曲線。
IVIM可提供標準ADC、慢ADC、快ADC和快ADC分數的多參數成像,同時反映組織的彌散和灌注信息,其中的標準ADC和慢ADC值對PCa和BPH診斷效能好,可作為PCa和BPH鑒別的良好指標。
[1] Ferlay J,Shin HR,Bray F,et al.Estimates of worldwise burden of cancer in 2008:GLOBOCAN 2008[J].Int J Cancer,2010,127(12):2893-917.
[2] Jemal A,Siegel R,Ward E,et al.Cancer statistics 2009[J].CA Cancer J Clin,2009,59(4):225-249.
[3] 陳昌毅,黃滿華,王遠梅,等.前列腺癌ADC值與PSA濃度的相關性研究[J].放射學實踐,2013,28(1):71-74.
[4] 閆晨宇,程敬亮,高雪梅.3.0T磁共振平掃和DWI在前列腺癌診斷中的應用[J].實用放射學雜志,2013,29(1):72-76.
[5] 李鵬,楊文君,陳志強,等.3.0T擴散加權成像對前列腺中央腺體癌和增生的鑒別診斷[J].臨床放射學雜志,2013,23(10):1458-1461.
[6] 楊棟,余深平,郭燕,等.標準化ADC值鑒別移行帶前列腺癌與間質為主增生結節[J].中山大學學報(醫學科學版),2013,34(2):287-291.
[7] 駱眾星,郭寧,謝斯棟.多b值DWI在前列腺癌和前列腺增生鑒別診斷中的應用研究[J].湖北民族學院學報(醫學版),2013,3(1):5-8.
[8] Peng YH,Jiang YL,Antic T,et al.Apparent diffusion coefficient for prostate cancer Imaging:impact of b values[J].AJR,2014,202(3):w247-253.
[9] Le Bihan D,Breton E,Lallemand D,et al.Separation of diffusion and perfusion in intravoxel incoherent motion MR imaging[J].Radiology,1988,168(2):497-505.
[10] Le Bihan D.Intravoxel incoherent motion perfusion MR imaging:a wake-up call[J].Radiology,2008,249(3):748-752.
[11] Pang Y,Turkbey B,Bernardo M,et al.Intravoxel incoherent motion MR imaging for prostate cancer:an evaluation of perfusion fraction and diffusion coefficient derived from different b-value combinations[J].Magn Reson Med,2013,69(2):553-562.
[12] Shinmoto H,Tamura C,Soga S,et al.An intravoxel incoherent motion diffusion-weighted imaging study of prostate cancer[J].AJR,2012,199(4):W496-W500.
[13] Riches SF,Hawtin K,Charles-Edwards EM,et al.Diffusion-weighted imaging of the prostate and rectal wall:comparison of biexponential and monoexponential modelled diffusion and associated perfusion coefficients[J].NMR Biomed,2009,22(3):318-325.
[14] Luczyńska E,Heinze-Paluchowska S,Domalik A,et al.The utility of diffusion weighted imaging (DWI).Using apparent diffusion coefficient (ADC) values in discriminating between prostateca ncer and normal tissue[J].Pol J Radiol,2014,79(12):450-455.
[15] Wang SY,Peng YH,Medved M,et al.Hybrid multidimensional T2and diffusion-weighted MRI for prostate cancer detection[J].J Magn Reson Imaging,2014,39(4):781-788.
[16] Roehl KA,Antenor JA,Catalona WJ,et al.Serial biopsy results in prostate cancer screening study[J].J Urol,2002,167(6):2435-2439.
[17] Mazaheri Y,Vargas HA,Akin O,et al.Reduction the influence of b-value selection on diffusion-weighted imaging of the prostate:evaluation of a revised monoexponential model within a clinical setting[J].J Magn Reson Imaging,2012,35(3):660-668.
[18] Quentin M,Blondin D,Klasen J,et al.Comparison of different mathematical models of diffusion-weighted prostate MR imaging[J].Magn Reson Imaging,2012,30(10):1468-1474.
[19] Pang Y,Turkbey B,Bernardo M,et al.Intravoxel incoherent motion MR imaging for prostate cancer:an evaluation of perfusion fraction and diffusion coefficient derived from different b-value combinations[J].Magn Reson Med,2013,69(2):553-562
[20] Dopfert J,Lemke A,Weidner A,et al.Investigation of prostate cancer using diffusion-weighted intravoxel incoherent motion imaging[J].Magn Reson Imaging,2011,29(8):1053-1058.
[21] Xu J,Humphrey PA,Kibel AS,et al.Magnetic resonance diffusion characteristics of histologically defined prostate cancer in humans[J].Magn Reson Med,2009,61(4):842-850.
[22] Farniel T,Ludemann L,Rudolph B,et al.Evaluation of normal prostate tissue,chronic prostatitis,and prostate cancer by quantitative perfusion analysis using a dynamic contrast-enhanced inversion-prepared dual-contrast gradient echo sequence[J].Invest Radiol,2008,43(7):481-487.
[23] McDonald DM,Choyke PL.Imaging of angiogenesis:from microscope to clinic[J].Nat Med,2003,9(6):713-725.
[24] Kuru TH,Roethke MC,Stieltjes B,et al.Intravoxel incoherent motion (IVIM) diffusion imaging in prostate cancer-what does it add?[J].J Comput Assist Tomogr,2014,38(4):558-564.
[25] De Marzo AM,Platz EA,Sutcliffe S,et al.Inflammation in prostate carcinogenesis[J].Nat Rev Cancer,2007,7(4):256-269.
[26] Klauss M,Lemke A,Grunberg K,et al.Intravoxel incoherent motion MRI for the differentiation between mass forming chronic pancreatitis and pancreatic carcinoma[J].Invest Radiol,2011,46(1):57-63.
[27] Sumi M,Van Cauteren M,Sumi T,et al.Salivary gland tumors:use of intravoxel incoherent motion MR imaging for assessment of diffusion and perfusion for the differentiation of benign from malignant tumors[J].Radiology,2012,263(3):770-777.
[28] Sigmund EE,Vivier PH,Sui D,et al.Intravoxel incoherent motion and diffusion-tensor imaging in renal tissue under hydration and furosemide flow challenges[J].Radiology,2012,263(3):758-776.
[29] Patel J,Sigmund EE,Rusinek H,et al.Diagnosis of cirrhosis with intravoxel incoherent motion diffusion MRI and dynamic contrast-enhanced MRI alone and in combination:preliminary experience[J].J Magn Reson Imaging,2010,31(3):589-600.
[30] Lemke A,Laun FB,Simon D,et al.An in vivo verification of the intravoxel incoherent motion effect in diffusion-weighted imaging of the abdomen[J].Magn Reson Med,2010,64(6):1580-1585.
Utility of Intravoxel Incoherent Motion Imaging in Differentiating Prostate Cancer from Benign Prostatic Hyperplasia
SUN Mei-yu,LIU Ai-lian,LI Ye,et al.
Department of Radiology,the First Affiliated Hospital of Dalian Medical University,Niaoning 116011,China
Objective:To analyze the intra-voxel incoherent motion (IVIM) imaging on differentiation of prostate cancer (PCa) and benign prostate hyperplasia (BPH).Methods:This retrospective study was approved by IRB.Seventy-two patients were divided into group PCa (n=32) and group BPH (n=40).Axial T2WI、DWI、LAVA dynamic contrast enhancement and IVIM imaging with EPI-STIR sequence was obtained from GE Signa 3.0T MR scanner with 10 b values of 0,20,50,100,200,400,600,800,1000,1200s/mm2,respectively.The standardADC,slowADC,fastADCand fraction of fastADCwere measured with MADC software in GE Functool 4.5 workstation.These four parameters from PCa and BPH groups were compared using the independent t test.Cut-off values of standard ADC and slowADCwere evaluated with receiver operator characteristic (ROC) analysis.Results:The mean standardADCand slowADCvalues were (6.21±2.35)×10-4mm2/s and (7.11±2.49)×10-4mm2/s for the PCa group,and (11.11±2.62)×10-4mm2/s and (12.65±1.81)×10-4mm2/s for the BPH group.The mean standard ADC and slow ADC values for PCa group were significantly lower than that of BPH group.The AUC of standardADCand slowADCwas 0.912 and 0.947.A threshold of 8.325×10-4mm2/s for the maximum standardADCvalue in the diagnosis of PCa resulted in a sensitivity of 78.13%,and a specificity of 97.50%.The positive predictive value (PPV),negative predictive value (NPV) and diagnostic accuracy for PCa were 96.15%,84.78% and 88.89%,respectively.A threshold of 10.03×10-4mm2/s for the maximum slowADCvalue in the diagnosis of PCa resulted in a sensitivity of 87.50%,and a specificity of 95.00%.The PPV,NPV and diagnostic accuracy for PCa were 93.33%,90.48% and 91.67%,respectively.Conclusion:The standardADCand slowADCvalues are significant IVIM index to differentiate PCa from BPH with satisfying sensitivity and specificity.
Prostatic neoplasms; Prostatic hyperplasia; Magnetic resonance imaging
116011 遼寧,大連醫科大學附屬第一醫院放射科
孫美玉(1975-),女,遼寧大連人,博士,副主任醫師,主要從事腹部影像診斷工作。
R445.2; R697.32; R737.25
A
1000-0313(2016)10-0947-05
10.13609/j.cnki.1000-0313.2016.10.010
2015-12-14
2016-04-25)
猜你喜歡
城市道橋與防洪(2022年4期)2022-07-01 06:04:12
體育科技文獻通報(2022年3期)2022-05-23 13:46:54
遼金歷史與考古(2021年0期)2021-07-29 01:06:54
家庭醫學(下半月)(2020年3期)2020-05-30 12:42:02
家庭醫學(下半月)(2020年3期)2020-05-30 12:42:00
家庭醫學(下半月)(2020年3期)2020-05-30 12:42:00
科技傳播(2019年22期)2020-01-14 03:06:54
民用飛機設計與研究(2019年4期)2019-05-21 07:21:24
當代陜西(2019年8期)2019-05-09 02:22:48
動漫星空(興趣百科)(2019年3期)2019-03-07 07:23:10
