認知刺激治療不同反應者的神經心理和功能比較*
2017-04-20 03:26:48郭愛紅王丙聚韓曉芳
陜西醫學雜志 2017年4期
郭愛紅, 王丙聚,韓曉芳
延安大學咸陽醫院神經內科(咸陽 712000)
認知刺激治療不同反應者的神經心理和功能比較*
郭愛紅, 王丙聚,韓曉芳△
延安大學咸陽醫院神經內科(咸陽 712000)
目的:比較不同阿爾茨海默病患者經認知刺激(CS)治療后的神經心理和功能指標。方法:回顧性分析60例輕度阿爾茨海默病患者的臨床資料,所有患者接受12個月的CS療法,比較治療前后的認知能力和機能指標。采用MMSE量表評估患者的治療反應。結果:治療前所有患者的社會人口變量、醫療條件、焦慮或抑郁癥狀、膽堿酯酶抑制劑(ChEIs)治療、理解水平、精神狀態或認知功能方面無差異。治療12個月后,31例患者治療有效(R,51.7%),29例患者治療無效(NR,48.3%)。R組患者在精神狀態,方向感,意識喚起方面,顯著優于NR組(P<0.05)。結論:CS治療后,R組病情優于NR組,患者治療前的認知能力和機能指標可預測治療效果,這有助于制定和優化AD患者在CS治療前的神經心理干預措施。
認知刺激(Cognitive stimulation,CS)療法可用于阿爾茨海默病(Alzheimer’s disease,AD)干預階段,具有與藥物相當的療效[1],但是CS療效的影響因素至今尚未發現。故本文探討輕度AD患者的CS治療效果及其影響因素。
資料和方法
1 一般資料 回顧性分析2014年1月至2016年12月符合研究標準的60例輕度AD患者的臨床資料。納入標準:臨床確診AD癥;完成12個月的CS治療。排除標準:文盲;嚴重語言障礙或持久性感覺障礙;腦血管意外、腦瘤、癲癇、創傷性腦損傷或嚴重精神障礙患者。
2 分組及評價指標 治療前/基線期(T0期)和CS治療后隨訪期(T1)的認知功能和機能指標由臨床神經心理學家和神經內科醫師評估并記錄。收集所有患者T0期和T1期的數據:社會人口數據(年齡、性別、教育程度),病史 (心臟病、高血壓、飲酒焦慮或抑郁癥狀,膽堿酯酶抑制劑(ChEIs)治療史等。MMSE量表用于評估方向感、注意力、工作記憶力、學習記憶力、語義理解能力、執行能力。IADL量表和Barthel指數(BI)評估工具性日常生活活動能力。
3 CS治療法 CS療法為期12個月。一個CS療程為2~3周。MMSE分數差值區分不同反應者。分數差=0判為無效NR,分數差>0判為有效R。
4 統計學方法 采用SPSS 20.0統計學軟件分析。卡方檢驗比較定性變量,t檢驗比較定量變量,Cohen’s d衡量組間差異,多元線性回歸分析療效影響因素,P<0.05認為差異具有統計學意義。
結 果
1 臨床特征比較 治療前57%的患者急性高血壓,42%的患者血脂異常,47%的患者抑郁癥,55%的患者接受膽堿酯酶抑制劑(ChEIs)治療。治療12個月后,31例患者治療有效(R,51.7%),29例患者治療無效(NR,48.3%)。
2 兩組認知功能比較 T0期:兩組MMSE及大多數神經心理學指標無差異,但數字順背、數字倒背、瞬間記憶存在組間差異;R組各項測試結果均優于NR組。T1期:兩組測試結果存在顯著差異。R組MMSE、時間感t(58)、語義理解各項測試結果均優于NR組。
3 兩組內治療前后指標比較 R組T1期方向感優于T0期;T1期時間感和MMSE均優于T0期。但是T1期BI值顯著降低。NR組T1期方向感優于T0期;但時間感、MMSE和BI均下降,見表1。
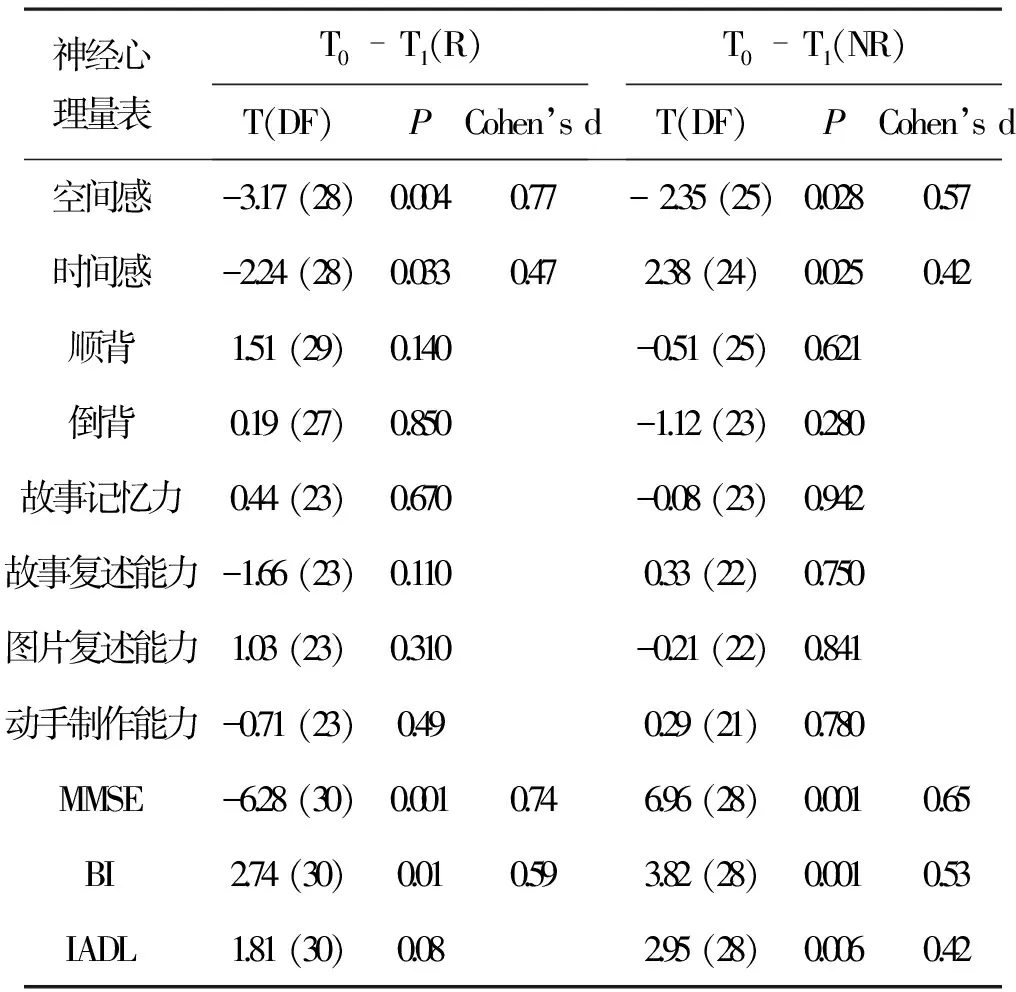
表1 兩組不同時期的神經功能指標比較
注:DF為自由度。
4 多元線性回歸分析 多元回歸分析發現,注意力、記憶力可更好的預測療效,β=-0.37,t(60) =-2.62,P= 0.012 (R2= 0.14)。
討 論
AD患者中,病感失認癥與疾病晚期、認知功能障礙及冷漠相關[2]。已有證據表明非藥物干預是治療阿爾茲海默病的重要補充措施[3]。本研究旨在探究輕度AD患者的認知和功能指標,是否可預測CS療效。研究結果發現,經過CS治療,51.7%患者治療有效,該結果與以住研究結果相一致[4]。此外,R組經CS治療后,機能水平提高的更明顯。兩組T0期的機能水平無差異,但CS治療后存在差異,說明CS治療可減緩輕度AD患者的病情。治療后,所有患者空間感都顯著改善。
多元回歸分析發現,年齡、性別、教育程度不是CS療效的預測因子,此結果與Aguirre等[5]的研究結果高齡、女性的CS療效更佳相反。注意力,學習記憶力和工作記憶力可更好的預測療效,與Saumier等[6]的研究結果相似。可能是由于認知功能在CS療法中占據主導地位。
綜上所述,CS治療后,R組病情改善情況優于NR組,患者治療前的認知能力和機能指標可預測治療效果,這有助于制定和優化AD患者在CS治療前的神經心理干預措施。
[1] 王瑋荻. 癡呆患者認知刺激療法研究進展[J]. 中國護理管理, 2016 (6): 851-854.
[2] 林 琳, 王昌在, 趙 贊. 鹽酸多奈哌齊聯合奧拉西坦治療老年癡呆 41 例[J]. 陜西醫學雜志, 2016 ,45(6): 749-750.
[3] 曹 飛, 況榮華, 李譞超, 等. 老年性癡呆非藥物干預的研究進展[J]. 南昌大學學報: 醫學版, 2013, 53(6): 84-88.
[4] Bottini G, Berlingeri M, Basilico S,etal. GOOD or BAD responder? Behavioural and neuroanatomical markers of clinical response to donepezil in dementia[J]. Behavioural Neurology, 2012, 25(2): 61-72.
[5] Aguirre E, Hoare Z, Streater A,etal. Cognitive stimulation therapy (CST) for people with dementia-who benefits most [J]. International Journal of Geriatric Psychiatry, 2013, 28(3): 284-290.
[6] Saumier D, Murtha S, Bergman H,etal. Cognitive predictors of donepezil therapy response in Alzheimer disease[J]. Dementia and Geriatric Cognitive Disorders, 2007, 24(1): 28-35.
(收稿:2016-08-15)
Comparison of neuropsychological and functional outcomes in Alzheimer’s disease patients with good or bad response to a cognitive stimulation treatment
Guo Aihong,Wang Bingju,Han Xiaofang.
Department of Neurology,Xianyang Hospital of Yan′an University(Xianyang 712000)
Objective: This study has sought to identify cognitive and functional measurements before and after the treatment which awere indicative of a better response to a one-year CS program. Method: A retrospective observational study was conducted in a sample of 60 users diagnosed with mild Alzheimer’s disease (AD) who followed a one-year CS program and underwent a cognitive and functional assessment before and after the intervention. As a primary measure of treatment response, we used the annual change of the Mini-Mental State Examination (MMSE) scores, which distinguished good responders (R) from non-responders (NR). Results: 51.7% of patients classified as R at baseline had a higher cognitive performance in attention, immediate verbal memory, language, and working memory compared to NR. No initial statistically significant differences were found between R and NR in any sociodemographic variables, medical conditions, anxiety and/or depressive symptoms, treatment with cholinesterase inhibitors (ChEIs), level of insight, global cognitive function (MMSE), or functional capacity. After 12 months of treatment, R had significantly better results than NR on MMSE, temporal orientation, category evocation. Conclusion: The response to a CS treatment of some subjects over others is linked to cognitive and functional capacity. This research contributes to characterize the neuropsychological profile that differentiates subjects who respond better than others before and after the treatment. This should contribute to customize and optimize neuropsychological interventions in patients with AD.
Dementia Cognitive Therapy Aged
*陜西省科學研究發展計劃項目(2016KJXX-28)
癡呆 認知療法 老年人
R749.16
A
10.3969/j.issn.1000-7377.2017.04.007
△通訊作者
猜你喜歡
中華詩詞(2022年6期)2022-12-31 06:41:24
音樂探索(2022年2期)2022-05-30 21:01:37
中華養生保健(2020年1期)2020-11-16 00:47:38
小天使·一年級語數英綜合(2019年8期)2019-08-27 02:23:00
中國中醫急癥(2019年10期)2019-05-21 07:20:30
小學科學(學生版)(2018年7期)2018-08-13 09:33:04
中國醫藥指南(2017年3期)2017-11-13 02:57:31
中國科技論壇(2017年7期)2017-07-25 08:49:53
鄭州大學學報(醫學版)(2015年2期)2015-02-27 14:50:46
中國中醫藥現代遠程教育(2014年22期)2014-03-01 04:32:55