不同劑量右美托咪定對室間隔缺損修補術患兒腦氧代謝的影響
2017-09-27 11:51:07蘇孟勤
實用藥物與臨床 2017年9期
鐘 巍,蘇孟勤
不同劑量右美托咪定對室間隔缺損修補術患兒腦氧代謝的影響
鐘 巍*,蘇孟勤
目的觀察不同劑量右美托咪定對室間隔缺損修補術患兒腦氧代謝的影響。方法120例室間隔缺損修補術患兒隨機分為4組,A、B、C組分別于麻醉誘導前10 min靶控輸注右美托咪定0.3、0.5、0.7 μg/kg,D組作為對照組,泵注等量生理鹽水;泵注完畢后四組均行麻醉誘導,術中維持腦電雙頻指數(BIS) 40~60。記錄四組患者圍術期不同時刻血流動力學相關指標變化,并于不同時刻抽取患者頸內靜脈球部血及橈動脈血行血氣分析,計算動脈-頸內靜脈球部血氧差(AV-DO2)及腦氧攝取率(cO2ER)。結果B組、C組氣管插管后、開胸后5 min、轉流結束時刻的MAP低于D組、A組(P<0.05)。A組、B組、C組氣管插管后、開胸后5 min、轉流5 min、轉流結束時刻及手術結束即刻AV-DO2及cO2ER均低于D組(P<0.05)。B組非轉流期間不良反應低于C組、D組(P<0.05),不良反應發生率更低。結論右美托咪定可降低室間隔缺損修補術患兒AV-DO2及cO2ER,且其作用在一定范圍內隨著劑量增加而降低,但泵注0.5 μg/kg右美托咪定血流動力學更穩定,且不良反應較少。
右美托咪定;室間隔缺損修補術;動脈-頸內靜脈球部血氧差;腦氧攝取率
0 引言
先天性室間隔缺損患兒臨床并不少見,體外循環下行室間隔缺損修補術為主要干預方法。有研究證實,體外循環后可引起患兒腦損傷,發生率高達33%~60%,其原因主要為術中腦組織缺血及炎癥反應損傷,患者術后可表現為精神錯亂、記憶能力降低等認知功能障礙[1-2]。臨床對體外循環室間隔缺損修補術患兒腦保護極為重視,右美托咪定應用于圍術期穩定血流動力學及降低炎癥反應損傷已得到臨床證實,但對于室間隔缺損修補術患兒采取何種劑量的腦保護效果最好尚無定論[3]。本研究入選患兒120例,采取不同劑量右美托咪定泵注,旨在探討不同劑量右美托咪定的腦保護效果,現報道如下。
1 臨床資料
1.1 一般資料 選擇2013年1月至2016年1月收治的120例室間隔缺損修補術患兒作為研究對象,均符合室間隔缺損診斷標準及手術指征,無明顯禁忌證,年齡6個月~12歲,ASA分級Ⅰ~Ⅱ級。120例患者隨機分為4組,各組患兒一般資料比較差異無統計學意義(P>0.05)。見表1。
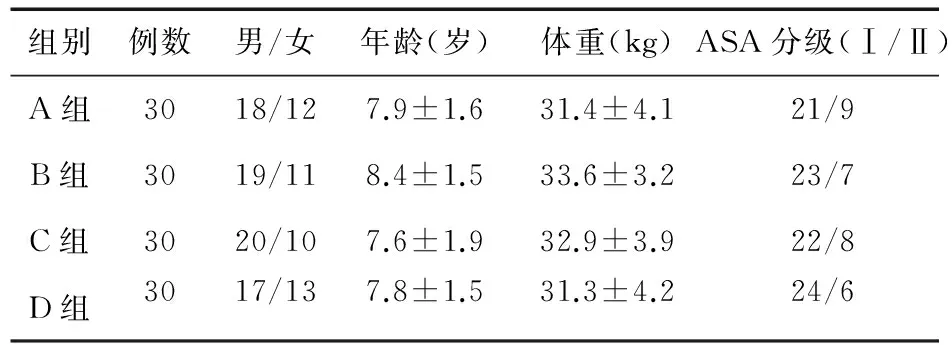
表1 四組患兒一般資料比較(例)
1.2 病例納入標準 ①患兒年齡≥6個月,且<12歲;②均符合室間隔缺損診斷標準及手術指征,無明顯禁忌證[4];③均符合倫理委員會基本要求;④均由監護人簽署知情同意。
1.3 病例排除標準 ①患兒年齡<6個月,或者≥12歲;②患兒合并嚴重心力衰竭,或者已喪失手術治療機會;③合并嚴重肝腎功能不全,估計難以耐受麻醉及手術患兒;④患兒家屬不同意手術者。
1.4 方法
1.4.1 術前準備 均完善相關檢查,入室后監測生命體征,并行有創動脈壓監測及中心靜脈壓監測,頸內靜脈穿刺時行逆行置管,遇阻力時則停止。
1.4.2 麻醉方法 A、B、C組分別于麻醉誘導前10 min靶控輸注右美托咪定0.3、0.5、0.7 μg/kg,D組作為對照組,泵注等量生理鹽水。泵注完畢后,四組均靜注長托寧0.1 mg、咪達唑侖0.05 mg/kg、芬太尼4 μg/kg、丙泊酚1.5~2.0 mg/kg、順阿曲庫銨0.15 mg/kg行麻醉誘導,待意識消失、肌松滿意后行氣管內導管插管,術中泵注瑞芬太尼10 μg/(kg·h)、丙泊酚6~10 mg/(kg·h)及間斷靜注順阿曲庫銨維持麻醉深度,術中維持腦電雙頻指數(BIS)于40~60范圍內。四組患者手術均由同一組外科醫生完成。

2 結果
2.1 四組患兒圍術期不同時刻血流動力學相關指標比較 B組、C組氣管插管后、開胸后5 min、轉流結束時刻,MAP均低于D組、A組(P<0.05),且HR低于D組(P<0.05);C組開胸后5 min、轉流結束時刻,MAP、HR低于其余三組(P<0.05)。見表2。
2.2 四組動脈-頸內靜脈球部血氧差(AV-DO2)及腦氧攝取率(cO2ER)比較 A組、B組及C組氣管插管后、開胸后5 min、轉流5 min、轉流結束時刻及手術結束即刻,AV-DO2、cO2ER均低于D組(P<0.05);且C組氣管插管后、開胸后5 min、轉流5 min、轉流及手術結束即刻的AV-DO2、cO2ER均低于A組、B組(P<0.05)。見表3。
2.3 不良反應發生率比較 D組非轉流期間發生術中高血壓(升高值>20%基礎值)3例,心率增快(升高值>20%基礎值)2例,不良反應5例(16.7%);A組術中高血壓2例(6.7%);B組未見不良反應;C組術中低血壓4例(降低值>20%基礎值),心率減慢(降低值>20%基礎值)3例,不良反應7例(23.3%)。四組不良反應發生率比較差異有統計學意義(P<0.05)。
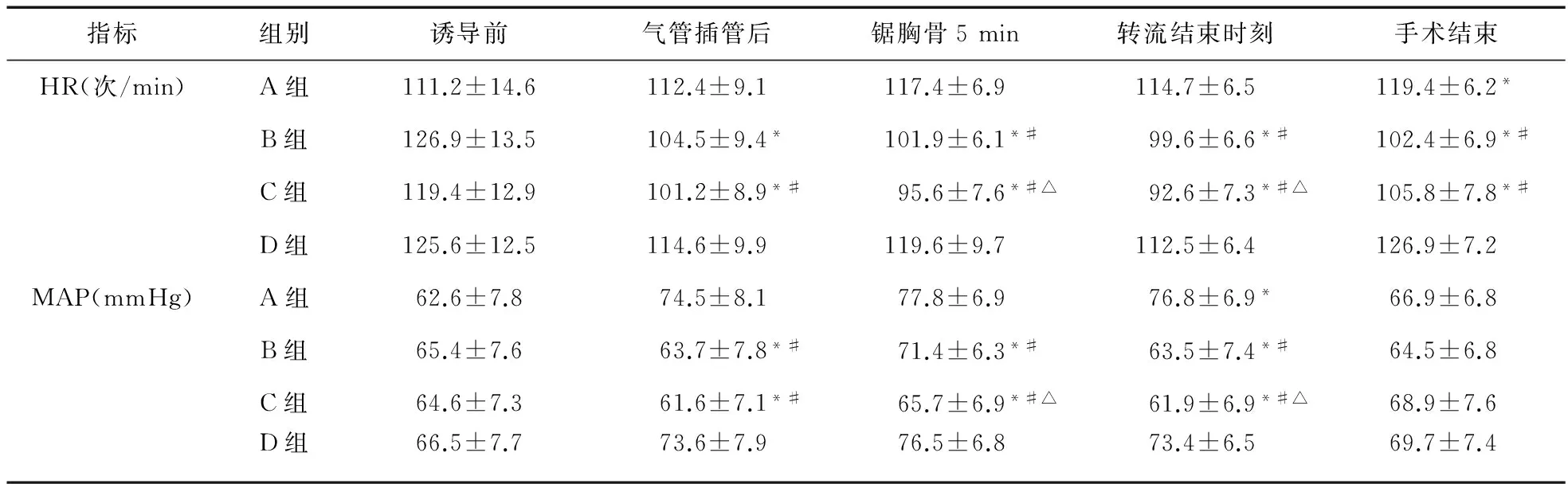
表2 四組患兒圍術期不同時刻血流動力學相關指標比較
注:*與D組比較,P<0.05;#與A組比較,P<0.05;△與B組比較,P<0.05
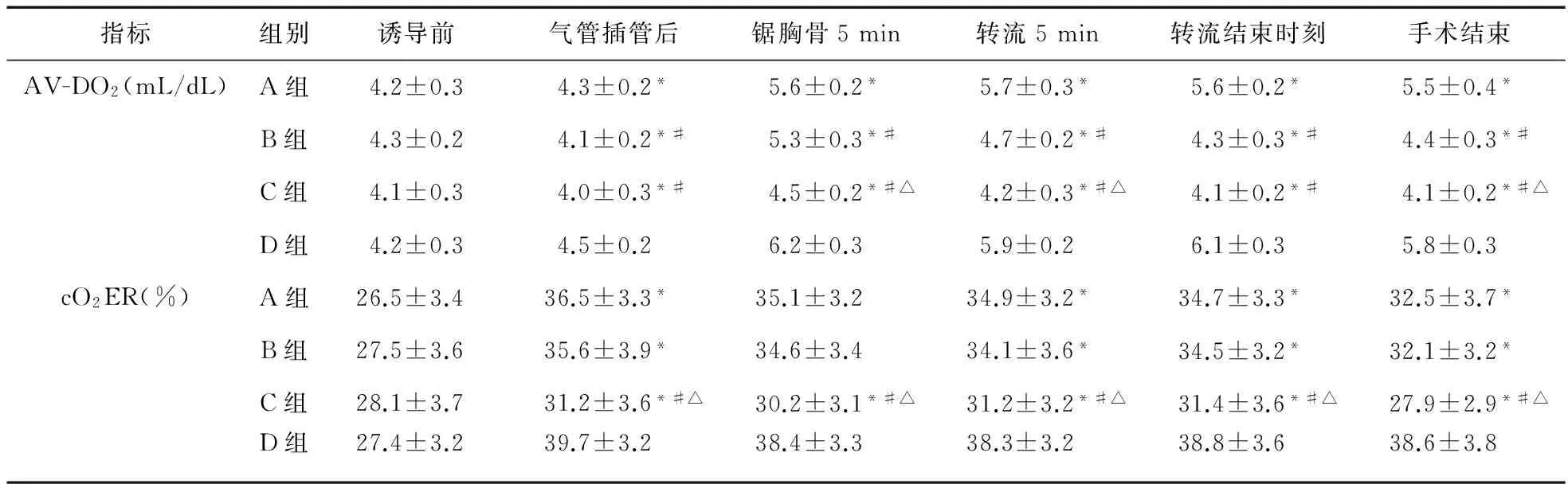
表3 四組患兒AV-DO2、cO2ER比較
注:*與D組比較,P<0.05;#與A組比較,P<0.05;△與B組比較,P<0.05
3 討論
因先天性室間隔缺損而需行修補術患兒臨床較為多見,此類患兒器官尚未發育成熟,代償功能較正常成人降低,而圍術期麻醉、手術刺激及體外循環等均可引起血流動力學劇烈波動及炎癥反應,引起一系列重要臟器功能損傷。有報道,腦組織對缺血缺氧較為敏感,腦損傷發生率較高[5-7]。
以往臨床多應用咪達唑侖聯合丙泊酚及阿片類藥物,雖能達到較好的麻醉效果,但圍術期血壓波動及腦代謝率高等問題,仍給體外循環手術患者圍術期安全提出更高的要求。右美托咪定可抑制突觸前膜P物質及傷害性肽類物質釋放,進而抑制傷害性刺激等的傳遞[8]。右美托咪定應用于顱內動脈瘤患者手術治療具有腦保護作用已得到臨床共識。相關研究表明,右美托咪定對海馬神經元具有顯著保護作用,可保護腦神經,避免局部缺血性神經損傷[9-10]。右美托咪定應用于心胸外科手術具有鎮靜、抗焦慮及穩定交感神經等作用,已得到臨床認可,但缺乏其劑量的相關報道。本研究結果表明,A組、B組的血流動力學均較為穩定,這可能與右美托咪定抑制交感神經作用相關;且隨著劑量增加,A組、B組、C組的平均動脈壓及心率降低,可能是因為隨著右美托咪定靶控濃度升高,其抑制作用增強。
腦血流代謝情況是評估顱腦損傷的重要指標之一,相關研究表明,AV-DO2、cO2ER降低表明顱腦氧供充足,而cO2ER降低表明機體腦灌注得到改善[11-14]。本研究表明,應用右美托咪定后,AV-DO2、cO2ER均顯著降低,其腦保護作用得到證實[15]。但本研究中,隨著右美托咪定靶控濃度升高,術中平均動脈壓低于70 mmHg例數增多,且心血管活性藥物使用率增加。本研究存在的不足之處:尚未將患兒蘇醒等相關指標進行統計學分析及討論,隨著靶控輸注右美托咪定濃度升高,其蘇醒時間及質量如何尚不清楚,以后在工作中將進一步總結。
[1] 李占軍,韓曙君,董蘭,等.不同劑量右美托咪定復合氯胺酮用于患兒室間隔缺損封堵術的麻醉效果[J].中華麻醉學雜志,2014,34(4):402-404.
[2] 王華偉,孫正輝,武琛,等.顱內動脈瘤栓塞術后復發的手術治療[J].中國現代神經疾病雜志,2015,15(3):219-223.
[3] Ohshima T,Miyachi S,Takahashi I,et al.Assessment of endovascular coil configuration for embolization of intracranial aneurysms using computational fluid dynamics[J].Nagoya J Med Sci,2015,77(3):383-388.
[4] 謝麗,袁麗萍.舒芬太尼/右美托咪定輔助表面麻醉減輕氣管插管應激反應的研究[J].西北藥學雜志,2016,31(4):406-408.
[5] Guo R,Cheng R.Evaluation of the sedative effect of dexmedetomidine on patients after surgical occlusion of ruptured cerebral aneurysm in intensive care unit[J].Zhongguo Wei Zhong Bing Ji Jiu Yi Xue,2012,24(5):306-308.
[6] Yokota H,Yokoyama K,Noguchi H,et al.Post-operative dexmedetomidine-based sedation after uneventful intracranial surgery for unruptured cerebral aneurysm:comparison with propofol-based sedation[J].Neurocrit Care,2011,14(2):182-187.
[7] Ramaswamy AH,Shaikh SI.Comparison of dexmedetomidine-propofol versus fentanyl-propofol for insertion of laryngeal mask airway[J].J Anaesthesiol Clin Pharmacol,2015,31(2):217-220.
[8] Yao Y,Qian B,Lin Y,et al.Intranasal dexmedetomidine premedication reduces minimum alveolar concentration of sevoflurane for laryngeal mask airway insertion and emergence delirium in children:a prospective,randomized,double-blind,placebo-controlled trial[J].Paediatr Anaesth,2015,25(5):492-498.
[9] Savla JR,Ghai B,Bansal D,et al.Effect of intranasal dexmedetomidine or oral midazolam premedication on sevoflurane EC50 for successful laryngeal mask airway placement in children:a randomized,double-blind,placebo-controlled trial[J].Paediatr Anaesth,2014,24(4):433-439.
[10]Kwak HJ,Min SK,Yoo JY,et al.The median effective dose of dexmedetomidine for laryngeal mask airway insertion with propofol 2.0 mg/kg[J].Acta Anaesthesiol Scand,2014,58(7):815-819.
[11]白潔,王曉娟,熊虹飛,等.右美托咪定聯合曲馬多預防瑞芬太尼麻醉后痛覺過敏的臨床研究[J].西北藥學雜志,2013,28(6):625-627.
[12]Bergese SD,Patrick BS,McSweeney TD,et al.A comparative study of dexmedetomidine with midazolam and midazolam alone for sedation during elective awake fiberoptic intubation[J].J Clin Anesth,2010,22(1):35-40.
[13]Tang W,Wang J,Fu GQ,et al.Effect of dexmedetomidine and midazolam on respiration and circulation functions in patients undergoing open heart surgery under acupuncture-assisted general anesthesia[J].Zhen Ci Yan Jiu,2014,39(3):216-221.
[14]張瑛,鐘文暉,王愛忠,等.右美托咪定對缺血-再灌注大鼠腸黏膜屏障功能的影晌[J].上海交通大學學報:醫學版,2014,34(4):487-490,506.
[15]李新春,戚巖,趙建輝,等.不同劑量右美托咪啶對顱腦損傷患者圍術期腦氧代謝的影響[J].河北醫藥,2013,35(3):356-357.
Effectsofdifferentdosesofdexmedetomidineoncerebraloxygenmetabolisminpediatricpatientswithventricularseptaldefectrepair
ZHONG Wei*,SU Meng-qin
(Department of Anesthesiology,Chest Hospital of Henan Province,Zhengzhou 450000,China)
ObjectiveTo observe the effects of different doses of dexmedetomidine on cerebral oxygen metabolism of children with ventricular septal defect repair.MethodsTotally 120 pediatric patients with ventricular septal defect repair were enrolled in the study.They were divided into 4 groups randomly.Patients in group A,group B and group C were given target controlled infusion of 0.3,0.5 and 0.7 μg/kg of dexmedetomidine respectively at 10 min before induction of anesthesia;group D (control group)
infusion of saline.All the patients received anesthesia induction,and the bispectral index (BIS) was maintained in the range of 40~60 during operation.The changes in hemodynamic indexes were recorded during perioperative period.The cerebral arteriovenous oxygen content difference (AV-DO2) and cerebral oxygen extraction ratio (cO2ER) were calculated by analyzing the radial arterial and jugular venous bulb blood samples.ResultsThe MAP in group B and group C after tracheal intubation,at 5 min after cutting breast bone and after flow was lower than that of group D and group A,and the HR in group B and group C was lower than that of group D (P<0.05);the AV-DO2and cO2ER after tracheal intubation,at 5 min after cutting breast bone and immediately after flow and surgery in group D were higher than those of the other groups (P<0.05).The adverse reaction rate in group B was lower than that of group C and group D (P<0.05).ConclusionDexmedetomidine can decrease the AV-DO2and cO2ER of pediatric patients with ventricular septal defect repair,which is reduced with the increase of dose within a certain range.Infusion of 0.5 μg/kg of dexmedetomidine has more stable hemodynamics and lower adverse reaction rate.
Dexmedetomidine;Ventricular septal defect repair;Cerebral arteriovenous oxygen content difference;Cerebral oxygen extraction ratio
2016-12-20
河南省胸科醫院麻醉科,鄭州 450000
*通信作者
10.14053/j.cnki.ppcr.201709020
猜你喜歡
課堂內外·初中版(科學少年)(2023年10期)2023-12-10 00:43:06
全科護理(2022年10期)2022-12-26 21:19:15
中國合理用藥探索(2022年1期)2022-11-26 00:22:32
昆明醫科大學學報(2021年2期)2021-03-29 07:42:46
鄉村科技(2021年33期)2021-03-16 02:26:54
國際放射醫學核醫學雜志(2021年10期)2021-02-28 08:41:58
河北畫報(2020年10期)2020-11-26 07:20:50
中國衛生標準管理(2015年3期)2016-01-14 03:41:47
西南軍醫(2014年5期)2014-04-25 07:42:48
中國合理用藥探索(2014年11期)2014-03-11 20:30:20