新輔助化療聯合手術治療骨肉瘤的長期效果分析
2019-10-23 14:04:42陳輝陳嵩陳培生陳順有林建華
中外醫學研究 2019年23期
關鍵詞:新輔助化療
陳輝 陳嵩 陳培生 陳順有 林建華
【摘要】 目的:通過平均10年隨訪分析新輔助化療聯合手術治療骨肉瘤(osteosarcoma,OS)的臨床預后。方法:收集2005年1月-2010年4月在福建醫科大學附屬第一醫院被診斷為OS的患者資料,包括性別、年齡、外科分期、病理分型、影像學資料等。納入病理確診骨肉瘤,采用多柔比星(ADM)、順鉑(DDP)和異環磷酰胺(IFO)聯合化療(術前1+術后6療程),隨訪資料完整的患者。結果:納入44例患者,男25例,女19例,年齡12~74歲,中位年齡18歲,平均(23.68±12.82)歲。目前隨訪時間97~162個月,平均(121.36±15.46)個月,超過10年。總的來說,生存率為43.19%(19/44),中位生存期為27個月,平均生存期為(64.07±52.36)個月(6~162個月)。總體死亡25例,發生在初診1、3、5、10年內的分別占44%(11/25)、88%(22/25)、96%(24/25)和100%(25/25)。病程中發生轉移高達65.91%(29/44),發生在初診即刻、1、3、5、10年內的分別為13.79%(4/29)、75.86%(22/29)、96.55%(28/29)、100%(29/29)和100%(29/29)。轉移型和非轉移型患者10年生存率分別為31.03%(9/29)和66.7%(10/15),差異有統計學意義(P<0.000)。結論:采用新輔助化療聯合手術治療后,OS患者平均隨訪10年生存率較短期隨訪顯著降低,而轉移率無明顯變化;轉移和死亡的發生主要集中在初診的3年內,轉移型患者的死亡率顯著高于非轉移型患者。
【關鍵詞】 骨肉瘤; 新輔助化療; 長期療效
doi:10.14033/j.cnki.cfmr.2019.23.002 文獻標識碼 A 文章編號 1674-6805(2019)23-000-04
【Abstract】 Objective:To analyze the clinical prognosis of osteosarcoma(OS) after treatment with neoadjuvant chemotherapy combined surgery through 10 years follow-up.Method:The data of patients diagnosed with OS in The First Affiliated Hospital of Fujian Medical University from January 2005 to April 2010 were collected,including gender,age,surgical staging,pathological classification and imaging material.Inclusion criteria:pathological diagnosis as osteosarcoma,had been treated with chemotherapy(ADM,CP and IFO) a period before surgery and 6 period after,and follow-up data integrity.Result:Forty-four patients included in this study,25 male and 19 female,median age 18 years,rang 12-74 years,average (23.68±12.82)years.The follow-up time average more than 10 years,average (121.36±121.36)months,rang 97-162 month.The overall survival rate was 43.19%(19/44),the median survival time was 27 months,and the average survival time was (64.07±52.36)months,rang 6-162 month.25 cases have been dead,the deaths occur in 1,3,5,10 years after diagnosed were 44%(11/25),88%(22/25),96%(24/25) and 100%(25/25) respectively.The general metastatic rate as high as 65.91%(29/44) through the course of disease,metastasis happened in the immediate,1,3,5,10 years after diagnosed were 13.79%(4/29),75.86%(22/29) and 96.55%(28/29),100%(29/29) and 100%(29/29) respectively.The 10 years survival rate of patients with or without metastasis was 31.03%(9/29) and 66.7%(10/15) respectively(P<0.000).Conclusion:The survival rate is obviously decreased but the metastatic rate slightly changes after a average 10 years follow-up compared with the results of short-term follow-up.The occurrence of metastasis and death is mainly concentrated in the first three years of disease,the mortality rate is significantly higher in patients with metastasis than who without.
【Key words】 Osteosarcoma; Neoadjuvant chemotherapy; Long-term efficacy
First-authors address:Fuzhou Second Hospital Affiliated to Xiamen University,Fuzhou 350007,China.
骨肉瘤(osteosarcoma,OS)是最常見的青少年原發性惡性骨腫瘤,男性多于女性[1]。目前OS患者的5年生存率仍然徘徊在50%~70%[2],超過1/4患者死于本病,給社會和家庭帶來了沉重的影響。過去的觀點認為,截肢是OS患者的主要治療方法。然而,10余年來,隨著新輔助化療藥物的發展,術前輔助化療不僅可縮小病灶范圍,而且可用于手術預后的評估及遠處轉移的預防,明顯降低患者的截肢率,同時也使得OS總體生存率明顯提高。新輔助化療聯合手術治療OS的臨床預后研究是近年來的熱點。但目前多數為短期隨訪研究,少有臨床長期隨訪報道,本文通過平均超過10年的隨訪,分析新輔助化療聯合手術治療OS的長期療效。
1 資料與方法
1.1 一般資料
選取2005年1月-2010年4月在福建醫科大學附屬第一醫院被診斷為OS的患者。納入標準:病理確診骨肉瘤,采用多柔比星(ADM)、順鉑(DDP)和異環磷酰胺(IFO)聯合化療(術前1+術后6療程),隨訪資料完整。總共納入44例患者,男25例,女19例;年齡12~74歲,中位年齡18歲,平均(23.68±12.82)歲。按Enneking分期:ⅡA期7例,ⅡB期37例;按生長部位:股骨20例,脛骨14例,其他部位10例;按組織學類型:小細胞型2例,毛細血管擴張型3例,普通型(包括成骨細胞型、成軟骨細胞型、成纖維細胞型等)39例。
1.2 方法
本課題組對存活的患者每年定期進行隨訪,針對原發病灶和肺部進行定期CT掃描。截至2018年6月,隨訪時間97~162個月,平均(121.36±15.46)個月。本課題組成員分別在2011年[3]和2012年[4]對這批OS患者進行了預后分析,分別報道了KISS1和GPR54蛋白的表達與OS患者預后的關系,發現短期隨訪結果生存率為54.5%,發生遠處轉移率為61.4%。但是,當年平均隨訪時間僅為29.19個月(6~55個月),由于隨訪時間較短,結果可能不夠準確。現在將平均超過10年的隨訪結果報道出來。
1.3 統計學處理
應用SPSS 20.0統計軟件,OS病例的中位生存分析和中位轉移分析采用Kaplan-Meier檢驗法;計量資料采用(x±s)表示,其他臨床資料的比較采用字2檢驗或Fisher確切概率法。以P<0.05為差異有統計學意義。
2 結果
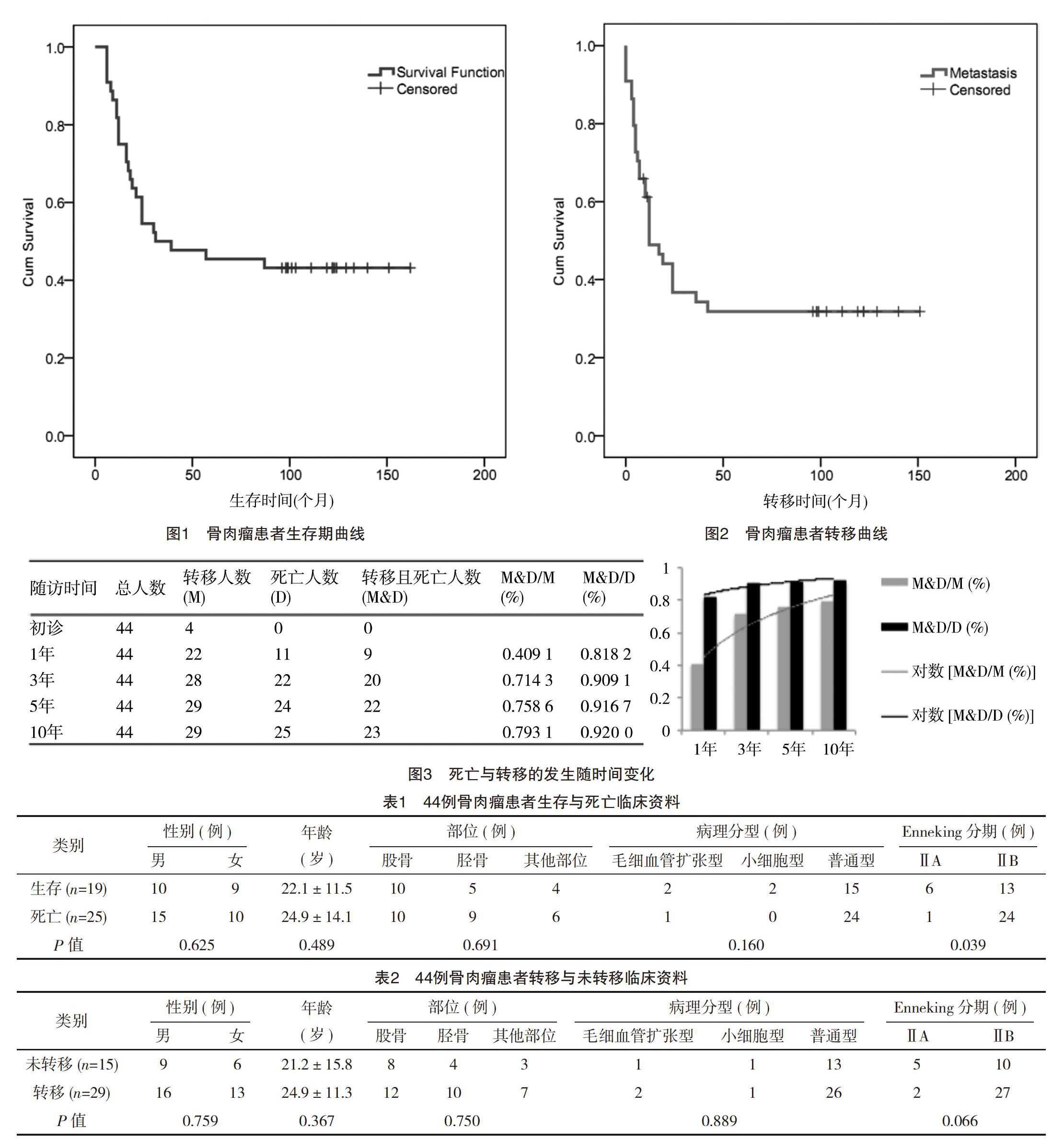
至2018年6月,隨訪時間97~162個月,平均(121.36±15.46)個月,總體生存率為43.2%(19/44),通過Recurrence free survival分析,中位生存期為27個月,平均生存期為(64.07±52.36)個月(6~162個月),見圖1;整個病程中發生轉移率高達65.9%(29/44),中位轉移時間為7個月,平均轉移時間為(11.00±10.56)個月(0~42個月),見圖2;而在早期隨訪時(8年前),總體生存率和轉移率分別為54.5%(24/44)、61.4%(27/44),長期隨訪的生存率顯著低(P=0.000),而轉移率無明顯變化。
隨訪末期總的死亡人數為25例,死亡發生在初診后1年內、3年內、5年內、10年內的分別占44%(11/25)、88%(22/25)、96%(24/25)和100%(25/25);可見,確診1年內死亡的人數將近到達總體死亡人數的一半,并且大部分的患者死亡發生在確診的3年內,見圖1。
發病過程中發生轉移總體人數為29例,肺部轉移占絕對多數(25例)。分析后發現轉移發生在初診后即刻、1、3、5、10年內的分別為13.79%(4/29)、75.86%(22/29)、96.55%(28/29)、100%(29/29)和100%(29/29)。可見初診時轉移人數較少,但是在初診后1年內轉移發生率迅速上升,3年后再發生轉移的人數同樣很少,5年后轉移人數沒有增加,因此5年和10年的轉移率相同,因此,大部分的患者轉移同樣是發生在確診的3年內,見圖2。
進一步分析發現,病程中發生轉移的患者(轉移型患者)死亡率在1、3、5、10年內的分別為40.91%(9/22)、71.43%(20/28)、75.86%(22/29)和79.31%(23/29)。而非轉移型患者的死亡率1、3、5、10年內的分別為9.09%(2/22)、12.5%(2/16)、13.33%(2/15)和13.33%(2/15)。轉移型患者死亡率顯著高于非轉移型患者,見圖3。
此外,外科分級ⅡB期的患者比ⅡA期的患者的患者死亡率顯著升高(P=0.039),但是轉移率無顯著差別(P=0.066)。而生存率和轉移率與年齡、性別、發生部位、病理分型無顯著相關性,見表1、表2。
3 討論
OS在年齡低于20歲的青少年人群中每年發病率約為8.7/1 000 000,約占兒童各種腫瘤的6%,死亡率極高[5-6]。研究表明,年齡、性別、身高、高骨代謝疾病、輻射環境和遺傳都是OS發生的危險因素[7-10]。
影響OS預后的因素也有很多,包括腫瘤的部位、范圍大小、發病年齡、是否伴發轉移、對化療的反應、手術方式等[11-19]。最近的一篇大樣本Meta分析結果顯示,性別也與預后相關[16]。筆者的研究發現,男性發病率比女性高(25∶19),但是性別對預后的影響并無統計學意義。另外,筆者的研究結果顯示,發生轉移后仍然存活的患者6例,這些患者化療后轉移病灶均消失,推斷這些患者OS組織對化療的反應良好,并且與預后相關,這與其他文獻[16]報道的結果類似。關于病理分型是否能影響OS預后,目前并沒有明確的證據,本研究中病理分型與轉移及死亡并無顯著相關性,因此病理分型可能并不是獨立影響預后的因素,而應該同時應考慮Enneking分期的影響(本研究中3例毛細血管擴張型和2例小細胞型都是ⅡA期)。
雖然OS的治療取得了一些進展,但目前仍然存在很多難題,OS患者遠期存活率的改善仍然有限。尤其是轉移型患者的預后仍然很差,而很多患者往往早期已發生轉移,死于轉移并發癥的患者超過50%[20-21]。據統計,初診時無轉移的患者5年存活率可達65%~70%,而其中僅有10%~20%患者需行截肢手術[22-23]。但初診時已有轉移表現的患者預后仍不容樂觀,伴有肺轉移的患者5年生存率僅為20%[24]。本研究中轉移型患者生存率在3、5、10年內的分別只有28.57%(8/28)、24.14%(7/29)和20.69%(6/29),5年生存率較文獻報告的稍高,但是無統計學意義。
不足之處,本文納入病例數較少,有些數據比較來自其他文獻的報道,但是本文作為一項平均超過10年的長期隨訪結果,對于OS患者遠期預后分析有一定的臨床意義。
綜上所述,筆者認為在OS患者中,轉移和死亡的發生主要集中在初診的3年內。無論是轉移型患者還是非轉移型的患者中,通過新輔助化療聯合手術治療可以提高的生存率。影響OS轉移及發展的機制非常復雜,課題組前期的研究已經發現KISS-1/GPR54基因系統等在OS的轉移和預后中起了重要作用[3-4],因此筆者將在此分子機制方面進一步探索,尋找改善OS患者預后的新靶點、新方法。
參考文獻
[1] Weber K L.Whats new in musculoskeletal oncology[J].J Bone Joint Surg Am,2005,87(6):1400-1410.
[2] ODay K,Gorlick R.Novel therapeutic agents for osteosarcoma[J].Expert Rev Anticancer Ther,2009,9(4):511-523.
[3]Wang F S,Chen H,Wu Z Y,et al.KISS1 expression in osteosarcoma:high in chinese clinical cases, but lower in cell lines[J].Asian Pac J Cancer Prev,2011,12(12):3229-3234.
[4]陳輝,吳朝陽,林建華,等.G蛋白偶聯受體 54 基因在骨肉瘤中的表達及其臨床意義[J].中國腫瘤生物治療雜志,2012(19):289-293.
[5] Goguet-Surmenian E,Richard-Fiardo P,Guillemot E,et al.CXCR7-mediated progression of osteosarcoma in the lungs[J].Br J Cancer,2013,109(6):1579-1585.
[6] Mirabello L,Troisi R J,Savage S A.Osteosarcoma incidence and survival rates from 1973 to 2004:Data from the surveillance,epidemiology,and end results program[J].Cancer,2009,115(7):1531-1543.
[7] Gorlick R,Khanna C.Osteosarcoma[J].J Bone Miner Res,2010,25(4):683-691.
[8] Arora R S,Kontopantelis E,Alston R D,et al.Relationship between height at diagnosis and bone tumours in young people:a meta-analysis[J].Cancer Causes Control,2011,22(5):681-688.
[9] Kim J,Mori T,Chen S L,et al.Chemokine receptor CXCR4 expression in patients with melanoma and colorectal cancer liver metastases and the association with disease outcome[J].Ann Surg,2006,244(1):113-120.
[10] Yang S C,Wu C H,Tu Y K,et al.Exposure to 2,3,7,8-tetrachlorodibenzo-p-dioxin increases the activation of aryl hydrocarbon receptor and is associated with the aggressiveness of osteosarcoma MG-63 osteoblast-like cells[J].Oncol Lett,2018,16(3):3849-3857.
[11] Davis A M,Bell R S,Goodwin P J.Prognostic factors in osteosarcoma: a critical review[J].J Clin Oncol,1994,12(2):423-431.
[12] Ferrari S,Bertoni F,Mercuri M,et al.Predictive factors of disease-free survival for non-metastatic osteosarcoma of the extremity: an analysis of 300 patients treated at the Rizzoli Institute[J].Ann Oncol,2001,12(8):1145-1150.
[13] Bielack S S,Kempf-Bielack B,Delling G,et al.Prognostic factors in high-grade osteosarcoma of the extremities or trunk: an analysis of 1,702 patients treated on neoadjuvant cooperative osteosarcoma study group protocols[J].J Clin Oncol,2002,20(3):776-790.
[14] Bacci G,Longhi A,Ferrari S,et al.Prognostic significance of serum lactate dehydrogenase in osteosarcoma of the extremity:experience at Rizzoli on 1421 patients treated over the last 30 years[J].Tumori,2004,90(5):478-484.
[15] Bacci G,Longhi A,Versari M,et al.Prognostic factors for osteosarcoma of the extremity treated with neoadjuvant chemotherapy:15-year experience in 789 patients treated at a single institution[J].Cancer,2006,106(5):1154-1161.
[16] Whelan J S,Jinks R C,McTiernan A,et al.Survival from high-grade localised extremity osteosarcoma:combined results and prognostic factors from three European Osteosarcoma Intergroup randomised controlled trials[J].Ann Oncol,2012,23(6):1607-1616.
[17] Ogura K,Fujiwara T,Yasunaga H,et al.Development and external validation of nomograms predicting distant metastases and overall survival after neoadjuvant chemotherapy and surgery for patients with nonmetastatic osteosarcoma:A multi-institutional study[J].Cancer,2015,121(21):3844-3852.
[18] Bertrand T E,Cruz A,Binitie O,et al.Do surgical margins affect local recurrence and survival in extremity,nonmetastatic,high-grade osteosarcoma?[J].Clin Orthop Relat Res,2016,474(3):677-683.
[19] Lee R J,Arshi A,Schwartz H C,et al.Characteristics and prognostic factors of osteosarcoma of the jaws:a retrospective cohort study[J].JAMA Otolaryngol Head Neck Surg,2015,141(5):470-477.
[20] Goguet-Surmenian E,Richard-Fiardo P,Guillemot E,et al.CXCR7-mediated progression of osteosarcoma in the lungs[J].Br J Cancer,2013,109(6):1579-1585.
[21] Ferrari S,Serra M.An update on chemotherapy for osteosarcoma[J].Expert Opin Pharmacother,2015,16(18):2727-2736.
[22] Bacci G,Balladelli A,Palmerini E,et al.Neoadjuvant chemotherapy for osteosarcoma of the extremities in preadolescent patients: the Rizzoli Institute experience[J].J Pediatr Hematol Oncol,2008,30(12):908-912.
[23] Bacci G,Ferrari S,Lari S,et al.Osteosarcoma of the limb.Amputation or limb salvage in patients treated by neoadjuvant chemotherapy[J].J Bone Joint Surg Br,2002,84(1):88-92.
[24] Mialou V,Philip T,Kalifa C,et al.Metastatic osteosarcoma at diagnosis: prognostic factors and long-term outcome-the French pediatric experience[J].Cancer,2005,104(5):1100-1109.
(收稿日期:2019-03-13) (本文編輯:何玉勤)
猜你喜歡
中國醫藥科學(2016年13期)2017-02-06 20:07:21
現代養生·下半月(2016年5期)2017-01-09 13:41:51
中國實用醫藥(2016年29期)2016-12-26 09:59:15
中國實用醫藥(2016年26期)2016-11-07 13:34:29
中國實用醫藥(2016年17期)2016-07-26 00:15:24
中國實用醫藥(2016年15期)2016-05-24 14:00:10
中國實用醫藥(2016年7期)2016-03-17 17:53:45
中國實用醫藥(2016年7期)2016-03-17 15:29:14
中國現代醫生(2015年25期)2016-02-27 12:32:48
中國實用醫藥(2016年5期)2016-02-20 21:53:59
