Augmented anastomotic urethroplasty with buccal mucosa for post penile fracture urethral injury long segment bulbar urethral stricture review
2021-09-05 09:48:58ShreyaSrivastava,AlexandraL.Tabakin,KevinJ.Chua等
Asian Journal of Urology 2021年3期
Dear editor,
The national incidence of penile fracture in the United States is estimated as 1.02 per 100 000 males [1].Nine to twenty percent of these injuries result in a concomitant urethral injury[2,3].Barros et al.[4]reported that 85 out of 888 penile fractures men with penile fractures had concomitant urethral injuries [4].Among those with both a penile fracture and urethral injury,only two cases of urethral stricture were reported.Furthermore,only three percent ofurethral strictures resulted from penile fractures [5].These data highlight the relatively low incidence of urethral stricture in patients with penile fracture and concomitant urethral injury.
According to the American Urological Association guidelines on male urethral stricture,when urethral disruption is noted after penile fracture or trauma,urinary diversion via suprapubic catheter and delayed urethral reconstruction are most commonly employed [6].However,few cases documented the management of urethral stricture in the setting of penile fracture associated urethral injuries [7].The authors herein present a case of penile fracture associated with extensive urethral injury resulting in long segment urethral stricture,the latter progressing to a 3.5 cm long near-obliterative bulbar urethral stricture that was successfully treated with augmented roof strip anastomotic urethroplasty with ventral onlay buccal mucosal graft substitution.Buccal mucosal graft substitution has been found to be highly successful in long segment urethral strictures[8,9].This approach to a long segment urethral stricture may also be utilized in strictures of any etiology,including those associated with penile fracture related urethral injuries.
A 46-year-old male with no significant past medical history,presented as a transfer from an outside hospital for evaluation of penile pain,ecchymosis,deformity,and swelling that he developed during sexual intercourse,associated with abrupt penile detumescence.At the outside facility,computed tomography scan revealed penile fracture and urethral injury.Soon after the injury,he noticed blood at the external urethral meatus.The patient had not voided since the incident and felt no pressure to void for over 12 h since the time of the incident.Physical examination at arrival in the emergency department revealed extensive penile swelling,deformity,ecchymosis,and tenderness involving the entire penile shaft.
Initial retrograde urethrogram showed contrast extravasation in the bulbar urethra along with prompt and extensive intravasation of contrast into the corpora cavernosa(Fig.1A).Contrast was also noted entering into the bladder.These findings were consistent with penile fracture and concomitant partial urethral disruption injury.Substantial inflammation and poor-quality tissue secondary to extensive urinary extravasation precluded any attempt of a successful primary urethral repair at the time of penile fracture repair.Additionally,catheterization was not attempted because of the extensive urethral injury at the time of presentation.
He therefore underwent suprapubic cystostomy catheter placement followed by exploration and repair of the penile fracture injury in the standard fashion.Extensive pericavernosal hematoma extending into the scrotum was drained.We then located and repaired a 2.5 cm tear in the anterolateral aspect of the crus of right corpus cavernosum using interrupted delayed absorbable sutures.The left corpus cavernosum was noted to be intact.Hemostasis was secure.A circumcision was then performed.There were no complications,and the patient was discharged home,on post-operative Day 4,with the suprapubic catheter connected to gravity drainage.
Retrograde urethrogram,6 weeks following the repair,revealed the presence of a near-obliterative,3.5 cm long bulbar urethral stricture (Fig.1B).Flexible cystoscopy revealed a pinpoint stricture at the penobulbar junction surrounded by spongiofibrosis through which we were unable to place a 0.889 mm guidewire.
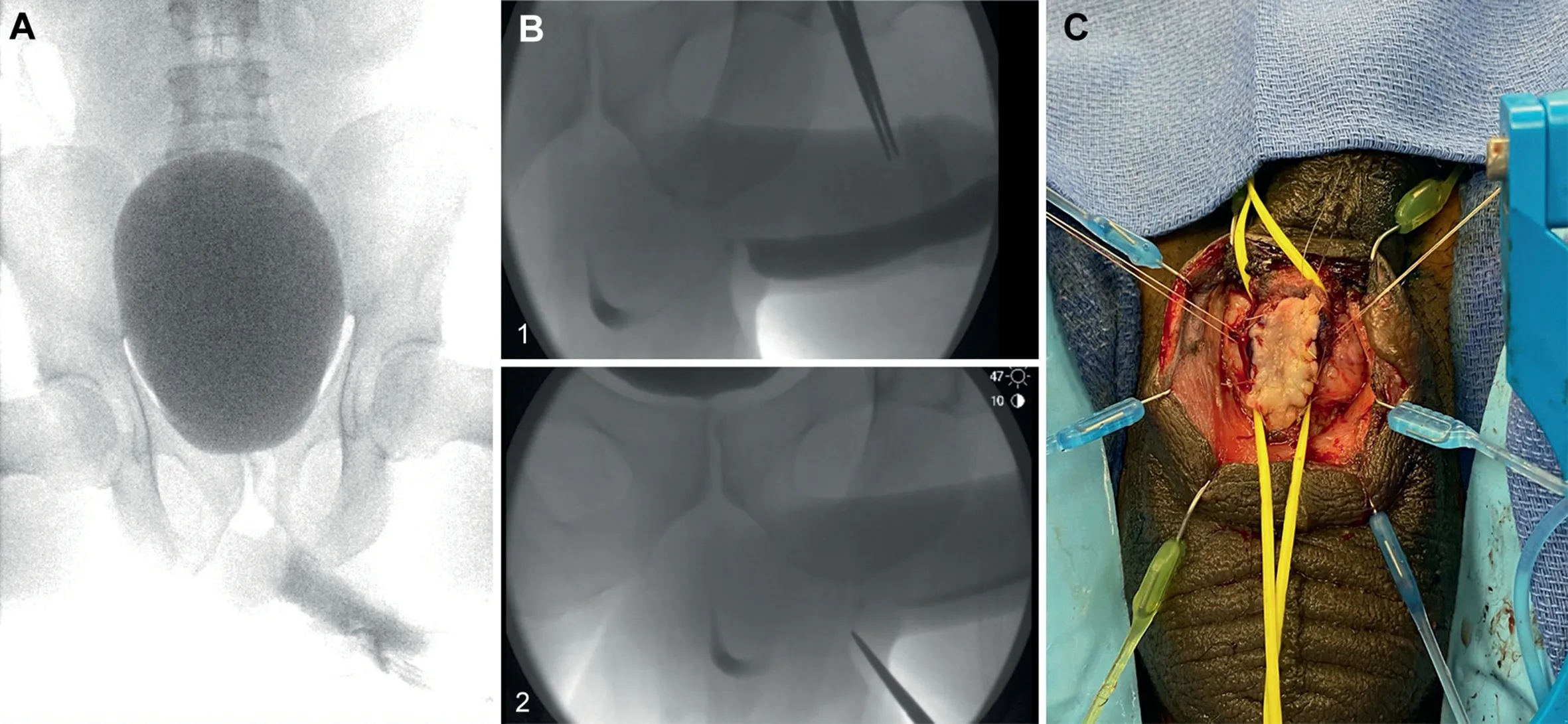
Figure 1 The results of retrograde urethrogram.(A) Retrograde urethrogram showing contrast intravasation into the corpora cavernosal;Contrast been entered the bladder in this patient with associated urethral injury.(B) Retrograde urethrogram done 3 months after initial presentation,revealing a long segment of urethral stricture(as shown as 1 and 2);(C)Open perineal roof strip anastomotic urethroplasty with buccal mucosal graft ventral onlay.
The patient subsequently underwent open perineal single-stage augmented anastomotic urethroplasty with ventral onlay buccal mucosal graft substitution of the penobulbar urethral stricture.The stricture in the distal bulbar urethra extending into the proximal penile urethra was exposed by a midline perineal incision in the standard fashion.A Lone Star? retractor with hooks facilitated excellent exposure for the urethroplasty.Extensive spongiofibrosis and scarring were noted at the site of urethral stricture.The strictured segment of the urethra and surrounding scar tissue were meticulously excised.Good vascularity and viability of the proximal and distal ends of the urethra were confirmed by brisk bleeding from the cut edges.A 3.5 cm gap was measured between the divided proximal and distal ends of the urethra.The roofs of the proximal and distal segments of the urethra were sutured together,and a 4 cm long buccal mucosal graft was used as a ventral onlay to bridge the gap on the ventral aspect(Fig.1C) to achieve the one-stage repair.Then a local tunica vaginalis flap was used to provide additional vascularity to the repair.The urethroplasty was completed over a 14 Fr silicone urethral catheter and the suprapubic cystostomy catheter was exchanged.
The first follow-up retrograde urethrogram,3 weeks after urethroplasty,showed focal contained contrast extravasation at the suture line (Fig.2A).A subsequent follow-up retrograde urethrogram,3 months after urethroplasty,revealed complete resolution of the extravasation (Fig.2B).The urethral catheter was then removed,and the suprapubic catheter was capped.Two weeks later,the patient reported satisfactory voiding with a strong urinary stream and normal erections.The suprapubic catheter was subsequently removed.At 1 year follow-up,the patient reported excellent quality of life,with normal voiding and erectile function,and no lower urinary tract symptoms.On physical exam,there was no chordee.Uroflowmetry revealed peak urinary flow rate of 15.4 mL/s with a normal voiding pattern and no postvoid residual urine.At 15-month follow-up,the patient reported continued normal voiding and erectile function,without any pain or urinary symptoms.
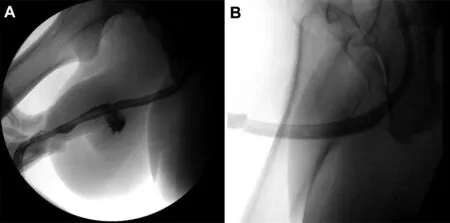
Figure 2 The follow-up retrograde urethrogram after urethroplasty.(A)First follow-up retrograde urethrogram showing contrast extravasation at the site of urethral repair;(B)Second follow-up retrograde urethrogram showing no contrast extravasation.
We present a rare case of complex penile fracture with concomitant urethral injury and unilateral cavernosal tear,resulting in a long segment bulbar urethral stricture.Urethroplasty in this patient involved the use of a buccal mucosa graft to bridge a 3.5 cm gap after excising a long,nearobliterative bulbar stricture.To our knowledge,this is the first case in which a buccal mucosal graft was successfully used for delayed augmented anastomotic urethroplasty for the repair of a complex penile fracture/urethral injury related to nearobliterative urethral stricture with extensive spongiofibrosis.
Author contributions
Case surgical management:
Alexandra L.Tabakin,Joshua Sterling,Charles F.Polotti,Jeremy C.Sinkin,Hari S.G.R.Tunuguntla.Drafting of manuscript:
Shreya Srivastava,Arnav Srivastava,Hari S.G.R.Tunuguntla.Critical revision of the manuscript:
Shreya Srivastava,Alexandra L.Tabakin,Kevin J.Chua,Hiren V.Patel,Joshua Sterling,Charles F.Polotti,Arnav Srivastava,Jeremy C.Sinkin,Hari S.G.R.Tunuguntla.Conflicts of interest
The authors declare no conflict of interest.
 Asian Journal of Urology2021年3期
Asian Journal of Urology2021年3期
- Asian Journal of Urology的其它文章
- Testing for BRCA1/2 and ataxiatelangiectasia mutated in men with high prostate indices:An approach to reducing prostate cancer mortality in Asia and Africa
- Male genital damage in COVID-19 patients:Are available data relevant?
- A comparison of artificial urinary sphincter outcomes after primary implantation and first revision surgery
- The neutrophil-tolymphocyte ratio at the prostate-specific antigen nadir predicts the time to castration-resistant prostate cancer
- Conquering new battlegrounds:Successful management of isolated giant retrovesical hydatid cyst with robotic assistance
- A systematic review of dedicated models of care for emergency urological patients