Hepatopulmonary metastases from papillary thyroid microcarcinoma: A case report
2022-06-23 06:27:56ChuanYuYangXuanWuChenDongTangWenJunYangXiaoXiaoMiJunPingShiWeiDongDu
World Journal of Clinical Cases 2022年14期
lNTRODUCTlON
Thyroid cancer is the most common endocrine tumor with a strong female preponderance (3:1)[1]. Papillary thyroid carcinoma (PTC) is a well-differentiated endocrine malignancy. Papillary thyroid microcarcinoma (PTMC) is defined by the World Health Organization as PTC with a maximum diameter ≤ 10 mm. Papillary thyroid microcarcinoma increases the incidence of thyroid cancer by 50%[2]. The main manifestations of PTCs are neck masses and thyroid nodules. However, distant metastasis of PTMC is rare, affecting bone, lung and chest lymph nodes, although local regional metastases in neck lymph nodes are commonly seen[3-5]. PTMC simultaneously metastasized to the liver and lung is very rare. Here, we report a case of PTMC concurrent with liver and pulmonary metastases.
CASE PRESENTATlON
Chief complaints
A 26-year-old woman who presented with unexplained fever was admitted to our hospital for further examination.
History of present illness
The patient showed a clear mind and no significant weight loss in the past three months.
History of past illness
She had no smoking or drinking history and no family history of tumors. She had no cough or expectoration. Ethical approval for publishing this case was obtained from the First Medical College of Zhejiang Chinese Medical University Research Ethics Committee.
Personal and family history
She denied a family history of hereditary disease.
Physical examination
Her physical examination showed nothing abnormal.
Laboratory examinations
23.Fanny: Perrault used the name Fanchon in the original French version of the tale. Most translators choose the name Fanny for English translations of the tale. Fanny is a short name or nickname for Frances in English. The name has been very popular at times in history although it is not popular today. It is unusual for a fairy tale character to have a name not related to her role in the story if she has one at all.Return to place in story.
Predictive factors for PTC metastasis included age, sex, thyroid function, Hashimoto's thyroiditis, multifocal tumor, tumor size, capsular invasion, and extrathyroidal extensions. The histopathological characteristics of tumors, such as their bilaterality, multifocality, extrathyroidal extension, capsular invasion, and lymph node metastasis, are important indicators of their invasiveness and they affect the prognosis[9,10].
Imaging examinations
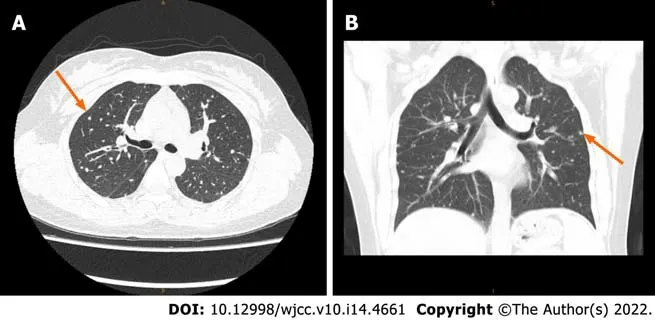
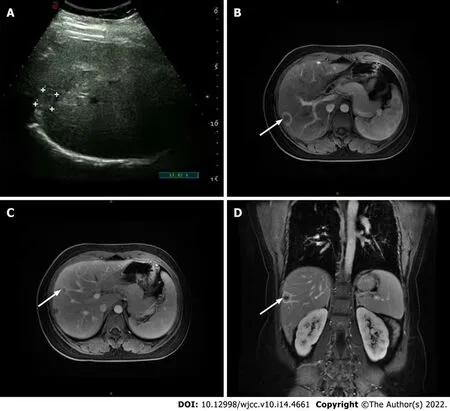
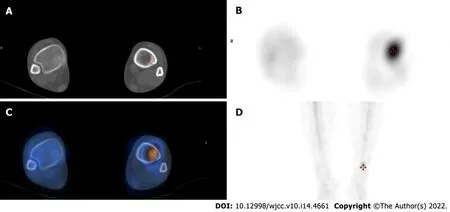
She underwent a positron emission tomography/magnetic resonance imaging (PET/MRI) examination in our hospital. The PET/MRI images showed a space-occupying lesion in the left thyroid with increased fluorodeoxyglucose (FDG) metabolism (Figure 1A), and a Computer tomography (CT) scan revealed that the lesions in the left lobe of the thyroid showed low-density nodular changes involving the thyroid capsule (Figure 1B). The PET/MRI images also showed multiple diffuse nodules (maximum 0.8 cm) in the lung with increased FDG metabolism and multiple nodules (maximum 2.0 cm) in the liver with increased FDG metabolism (Figure 1). Chest CT showed multiple metastases in both lungs, multiple low-density shadows in the liver, and small calcifications in the left breast (Figure 2). Abdominal ultrasound showed a fatty liver and multiple liver nodules (Figure 3A). MRI showed multiple space-occupying lesions in the liver (Figure 3B-D). Whole-body bone imaging and organ tomography showed a metabolically active left tibia and unevenly increased local bone density (Figure 4).

FlNAL DlAGNOSlS
Collectively, based on the medical imaging results and pathological features, a diagnosis of hepatopulmonary metastasis from papillary thyroid microcarcinoma was made.
TREATMENT
In conclusion, we present the case of a young woman with PTMC metastasis to her liver and lung. Since patients with thyroid cancer concurrent with hepatopulmonary metastases have rarely been reported, our case highlights the clinical and pathological profiles of these patients.
OUTCOME AND FOLLOW-UP
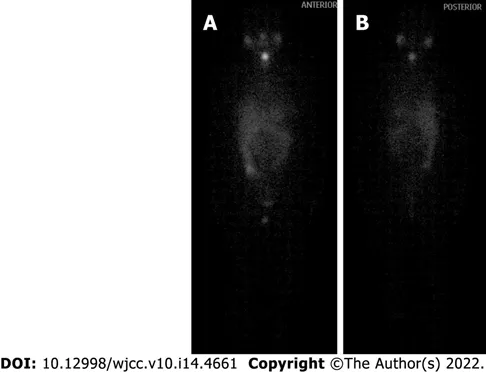
One year after thyroid cancer surgery, the patient was given iodine-131 treatment in our hospital. As shown in Figure 7, iodine imaging in the thyroid area was considered to be residual thyroid tissue. Multiple small nodules were found in both lungs, with no significant iodine uptake. A small amount of pleural effusion was observed on both sides of the lung. Multiple lymph nodes were present in the bilateral neck and supraclavicular areas without iodine intake. Physiological iodine intake was observed in the nasopharynx, oral cavity, salivary glands, gastrointestinal tract, and bladder (Figure 7). The patient had recovered well after the operation, and the incision had healed well. The patient was treated after the iodine therapy with daily oral levothyroxine sodium administration.
DlSCUSSlON
PTC accounts for approximately 85% of all follicular-derived well-differentiated thyroid cancers[6]. The 10-year survival rate is more than 80%, and these tumors are considered to be indolent[7,8]. PTMC is a subtype of PTC with a foci diameter ≤ 10 mm. PTMC accounts for the majority of PTC cases. Distant metastasis of PTMC is rare. The most common metastatic sites include the bone and lung, while brain, eye, breast, liver, kidney, muscle, and skin metastases are not commonly seen and only appear in patients with advanced tumor diseases. Here, we present a patient with PTMC who had simultaneous metastases to the lung and liver. Coexisting lung and liver metastases in PTC patients are not commonly seen.
She stretched her finger toward another object on the mantle. I allowed her to touch everything in sight, plants, glass objects, TV, VCR, lamps, speakers, candles and artificial flowers. If she started to grab, I gently reminded her to use one finger. She always obeyed. But, Hannah, an only child, possessed6 a more adventur ous personality. Her father predicted it would prevent her from accepting the one finger rule.
Then Tsar Vyslav, greatly desiring it, sent for his two eldest sons, and said: Ye, my sons, failed even to see the thief of my apples, yet thy brother Ivan has at least brought me one of its feathers. Take horse now, with my blessing13, and ride in search of it, and to the one of you who brings it to me alive I will give the half of my Tsardom. And the Tsarevitches Dimitri and Vasilii, envious14 of their younger brother Ivan, rejoiced that their father did not bid him also go, and mounting their swift horses, rode away, gladly, both of them, in search of the Fire Bird.
Liver metastasis from PTMC is a rare event with a reported frequency of only 0.5%[11]. Liver masses can be detected by various imaging modalities, such as ultrasonography, computed tomography, and magnetic resonance imaging. Liver masses are usually
I-negative in PTMC patients with liver metastasis[12], which is consistent with the observations in our patient. PTC liver metastasis has a poor prognosis. Surgical resection of liver lesions has been reported to offer the best chance for prolonged survival[13]. An increased age in cases of thyroid cancer with lung metastasis increases the mortality risk. In a study performed by Huang, the mortality rates of thyroid cancer with lung metastasis were 32.78% (118/360), 46.71% (156/334), 53.93% (199/369), 58.96% (158/268) and 82.76% (72/87) in patients aged ≤ 55 years, > 55 ≤ 65 years, > 65 ≤ 75 years, > 75 ≤ 85 years and > 85 years[14]. Since our patient was a young mother of a young child, we suggested routine follow-up liver function tests to monitor the pathophysiology of the liver.
PTMC has no early typical symptoms due to its anatomic location. Therefore, a delay in clinical diagnosis is inevitable, which leads to its diagnosis in the advanced stage. Thus, a primary tumor in the thyroid is usually not diagnosed until the symptoms of a secondary metastatic tumor appear[15]. In this case, the patient did not exhibit clinical manifestations of the disease at the initial stage, and no corres
ponding clinical symptoms were found even after metastasis occurred. Multiple metastases of thyroid cancer were incidentally found during the patient’s examination for unexplained fever, indicating that the disease is easily missed. Therefore, a better clinical index or screening method is needed.
21. You shall become my wife: This is not a romantic fairy tale in which a love match marriage takes place. The king appears interested in the daughter for his wife only for monetary reasons. First, he will be able to keep her supposed skills for his own monetary gain. Second, he can keep her from providing the same skills to a possible rival.Return to place in story.
I screamed at her, Who are you? I don t know you! How dare you come to my house and scare my daughter! To this, my mom quietly answered, Oh, I m so sorry. I may have gotten the wrong address, and she disappeared out of sight.
Male patients with distant metastases from PTMC have a high risk of death[8,15]. However, PTC patients with distant metastases have lower levels of dedifferentiation than differentiated thyroid carcinoma patients with distant metastases. Therefore, PTC exhibits more indolent behaviors than differentiated thyroid carcinoma, even with distant metastases. PTC nevertheless has a generally favorable prognosis for long-term survival, even with distant metastases. The clinical manifestations vary from the early to late stages of the disease[6]. The maximal PTMC foci is 1 cm or less[16]. In our patient, postoperative pathology revealed one PCT foci with a diameter of 0.8 cm. Total thyroidectomy with central node dissection is an effective treatment for PTC patients[17]. Long-term follow-up of PTMC patients is needed after surgical treatment[18,19]. Periodic thyroglobulin and thyroglobulin autoantibody measurements are recommended for PTMC patients[20]. An active surveillance approach is recommended by the American Thyroid Association guidelines as an alternative option for patients with low-risk PTMC[18]. Our patient was a 26-year-old woman with PTMC with multiple metastases. She was recommended to take levothyroxine sodium tablets and consume a low iodine diet after her surgery. We also suggested routine thyroid function test and liver imaging during follow-up. She is still alive and actively engaging in daily life.
Our case report is written according to CARE Checklist (2016).
CONCLUSlON
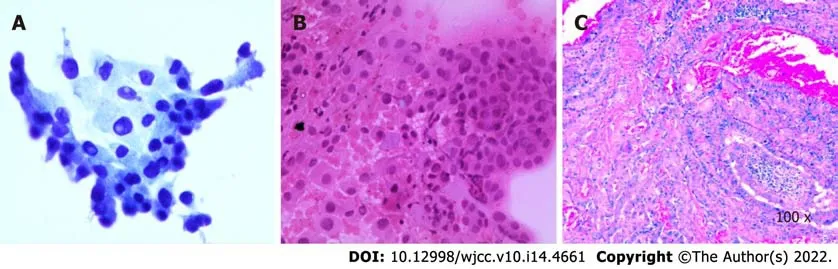
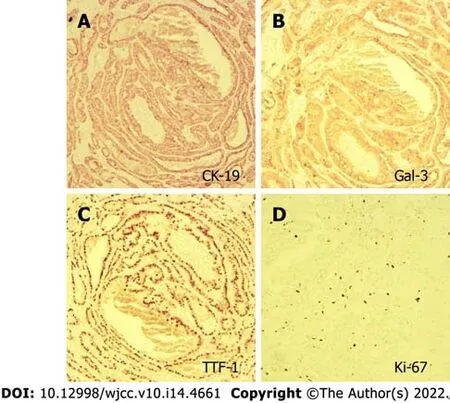
The patient underwent thyroidectomy and central node dissection. Postoperative pathology revealed multiple papillary microcarcinomas in the left thyroid and one foci with the follicular subtype (Figure 5). The carcinomas had invaded the capsule and presented no lymph node metastasis. The immunohistochemical results showed positive signals for CK-19, Gal-3, TTF, and Ki-67 (3%) (Figure 6).
ACKNOWLEDGEMENTS
The authors would like to thank colleagues from the Institute of Translational Medicine of the Affiliated Hospital of Hangzhou Normal University and colleagues from the Department of Hepatobiliary Surgery of the First Clinical Medical College of Zhejiang Chinese Medical University for their support and collaboration.
FOOTNOTES
Yang CY and Chen XW provided the case; Tang D performed radiological imaging analysis; Yang WJ performed pathological imaging analysis; Yang CY was involved in the biomedical analysis; Yang CY and Mi XX wrote the manuscript with input from Chen XW, Tang D and Yang WJ; Du WD and Shi JP revised the manuscript; all authors have contributed significantly.
The authors declare that they have no competing interests.
Her thyroid function tests showed elevated levels of thyroid-stimulating hormone and antithyroglobulin antibody, with a decreased level of thyroglobulin. Her biochemical tests showed elevated levels of triglycerides and cholesterol. Routine blood tests showed neutrophilia and lymphocytosis. Humoral tumor screening presented an elevated level of CA50. Her blood coagulation function was normal.
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
the Joint Funds of the Zhejiang Provincial Natural Science Foundation of China, No. LBY21H030001; and the Science and Technology Planning Project of Zhejiang Province, No. 2020KY708.
Our patient's diagnosis of hepatopulmonary metastasis from papillary thyroid carcinoma was based on imaging findings and pathological results. PET/MRI, ultrasonography, CT, and MRI revealed multiple nodules in the liver and lung. Our case will provide a valuable reference for the diagnosis and treatment of papillary thyroid microcarcinoma patients in the future.
Cherry-scented smoke from Grampy s pipe kept the hungry mosquitoes at bay while gray, wispy1 swirls2 danced around our heads. Now and again, he blew a smoke ring and laughed as I tried to target the hole with my finger. I, clad in a cool summer nightie, and Grampy, his sleeveless T-shirt, sat watching the traffic. We counted cars and tried to guess the color of the next one to turn the corner.
Then the Devil came to him and said, What seekest thou? If thou wilt3 take me as a godfather for thy child, I will give him gold in plenty and all the joys of the world as well
When King Quimus heard of the approach of such a great company, he sent out his wazir to give the prince honourable177 meeting, and to ask what had procured178 him the favour of the visit
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
China
Chuan-Yu Yang 0000-0001-8159-619X; Xuan-Wu Chen 0000-0001-9537-1135; Dong Tang 0000-0001-5902-8604; Wen-Jun Yang 0000-0001-5251-532X; Xiao-Xiao Mi 0000-0001-5516-3139; Jun-Ping Shi 0000-0001-9434-897X; Wei-Dong Du 0000-0002-4245-3257.
Xing YX
A
Xing YX
1 Stewart LA, Kuo JH. Advancements in the treatment of differentiated thyroid cancer.
2021; 12: 20420188211000251 [PMⅠD: 33796254 DOⅠ: 10.1177/20420188211000251]
2 Kitahara CM, Sosa JA. The changing incidence of thyroid cancer.
2016; 12: 646-653 [PMⅠD: 27418023 DOⅠ: 10.1038/nrendo.2016.110]
3 Mazzaferri EL, Jhiang SM. Long-term impact of initial surgical and medical therapy on papillary and follicular thyroid cancer.
1994; 97: 418-428 [PMⅠD: 7977430 DOⅠ: 10.1016/0002-9343(94)90321-2]
4 Sampson E, Brierley JD, Le LW, Rotstein L, Tsang RW. Clinical management and outcome of papillary and follicular (differentiated) thyroid cancer presenting with distant metastasis at diagnosis.
2007; 110: 1451-1456 [PMⅠD: 17705176 DOⅠ: 10.1002/cncr.22956]
5 Carmel Neiderman NN, Duek Ⅰ, Ravia A, Yaka R, Warshavsky A, Ringel B, Muhanna N, Horowitz G, Ziv Baran T, Fliss DM. The incidence of postoperative re-stratification for recurrence in well-differentiated thyroid cancer-a retrospective cohort study.
2021; 10: 2354-2367 [PMⅠD: 34527547 DOⅠ: 10.21037/gs-21-105]
6 Lim H, Devesa SS, Sosa JA, Check D, Kitahara CM. Trends in Thyroid Cancer Ⅰncidence and Mortality in the United States, 1974-2013.
2017; 317: 1338-1348 [PMⅠD: 28362912 DOⅠ: 10.1001/jama.2017.2719]
7 Yu XM, Wan Y, Sippel RS, Chen H. Should all papillary thyroid microcarcinomas be aggressively treated?
2011; 254: 653-660 [PMⅠD: 21876434 DOⅠ: 10.1097/SLA.0b013e318230036d]
8 Weng HY, Yan T, Qiu WW, Xi C, Hou LY, Yang ZL, Qiu ZL. Long-term outcomes and prognostic factors in papillary thyroid microcarcinoma patients with distant metastases.
2021 [PMⅠD: 34699028 DOⅠ: 10.1007/s12020-021-02906-8]
9 Zhao L, Sun X, Luo Y, Wang F, Lyu Z. Clinical and pathologic predictors of lymph node metastasis in papillary thyroid microcarcinomas.
2020; 49: 151647 [PMⅠD: 33126150 DOⅠ: 10.1016/j.anndiagpath.2020.151647]
10 Jeon MJ, Kim WG, Choi YM, Kwon H, Lee YM, Sung TY, Yoon JH, Chung KW, Hong SJ, Kim TY, Shong YK, Song DE, Kim WB. Features Predictive of Distant Metastasis in Papillary Thyroid Microcarcinomas.
2016; 26: 161-168 [PMⅠD: 26563473 DOⅠ: 10.1089/thy.2015.0375]
11 Salvatori M, Perotti G, Rufini V, Maussier ML, Summaria V, Fadda G, Troncone L. Solitary liver metastasis from Hürthle cell thyroid cancer: a case report and review of the literature.
2004; 27: 52-56 [PMⅠD: 15053244 DOⅠ: 10.1007/BF03350911]
12 Song HJ, Xue YL, Xu YH, Qiu ZL, Luo QY. Rare metastases of differentiated thyroid carcinoma: pictorial review.
2011; 18: R165-R174 [PMⅠD: 21632805 DOⅠ: 10.1530/ERC-11-0068]
13 Kuo CS, Tang KT, Lin JD, Yang AH, Lee CH, Lin HD. Diffuse sclerosing variant of papillary thyroid carcinoma with multiple metastases and elevated serum carcinoembryonic antigen level.
2012; 22: 1187-1190 [PMⅠD: 23050785 DOⅠ: 10.1089/thy.2011.0361]
14 Huang X, Xia Q, Huang Y, Peng A, Yang J. Age increased the cancer-specific mortality risk of thyroid cancer with lung metastasis.
2022 [PMⅠD: 34990026 DOⅠ: 10.1111/cen.14675]
15 Nunes KS, Matos LL, Cavalheiro BG, Magnabosco FF, Tavares MR, Kulcsar MA, Hoff AO, Kowalski LP, Leite AK. Risk factors associated with disease-specific mortality in papillary thyroid cancer patients with distant metastases.
2021 [PMⅠD: 34665427 DOⅠ: 10.1007/s12020-021-02901-z]
16 Pu W, Shi X, Yu P, Zhang M, Liu Z, Tan L, Han P, Wang Y, Ji D, Gan H, Wei W, Lu Z, Qu N, Hu J, Hu X, Luo Z, Li H, Ji Q, Wang J, Zhang X, Wang YL. Single-cell transcriptomic analysis of the tumor ecosystems underlying initiation and progression of papillary thyroid carcinoma.
2021; 12: 6058 [PMⅠD: 34663816 DOⅠ: 10.1038/s41467-021-26343-3]
17 Pastor?i? Grgi? M, Stubljar B, Per?e P, Zekan Vu?eti? M, ?iti? S. Total Thyroidectomy with Central Node Dissection is a Valuable Option in Papillary Thyroid Cancer Treatment.
2020; 59: 102-107 [PMⅠD: 34219891 DOⅠ: 10.20471/acc.2020.59.s1.13]
18 Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, Pacini F, Randolph GW, Sawka AM, Schlumberger M, Schuff KG, Sherman SⅠ, Sosa JA, Steward DL, Tuttle RM, Wartofsky L. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer.
2016; 26: 1-133 [PMⅠD: 26462967 DOⅠ: 10.1089/thy.2015.0020]
19 Gao M, Ge M, Ji Q, Cheng R, Lu H, Guan H. 2016 Chinese expert consensus and guidelines for the diagnosis and treatment of papillary thyroid microcarcinoma.
2017; 14: 203-211 [PMⅠD: 28948061 DOⅠ: 10.20892/j.issn.2095-3941.2017.0051]
20 Knappe L, Giovanella L. Life after thyroid cancer: the role of thyroglobulin and thyroglobulin antibodies for postoperative follow-up.
2021; 16: 273-279 [PMⅠD: 34693849 DOⅠ: 10.1080/17446651.2021.1993060]
 World Journal of Clinical Cases2022年14期
World Journal of Clinical Cases2022年14期
- World Journal of Clinical Cases的其它文章
- Perfectionism and mental health problems: Limitations and directions for future research
- Ovarian growing teratoma syndrome with multiple metastases in the abdominal cavity and liver: A case report
- Development of plasma cell dyscrasias in a patient with chronic myeloid leukemia: A case report
- Suprasellar cistern tuberculoma presenting as unilateral ocular motility disorder and ptosis: A case report
- Rare pattern of Maisonneuve fracture: A case report
- PD-1 inhibitor in combination with fruquintinib therapy for initial unresectable colorectal cancer: A case report