Effect of enhanced recovery after surgery on inflammatory bowel disease surgery:A meta-analysis
2022-06-23 02:06:34DongPengYuXiChengWeiTaoHuaTangGuangYanJi
World Journal of Clinical Cases 2022年11期
lNTRODUCTlON
Enhanced recovery after surgery (ERAS) or fast-track surgery programs were first proposed by Kehlet[1], and the purpose of ERAS was to reduce surgical pressure and accelerate postoperative functional recovery[2]. The ERAS protocol involves a series of interventions during the perioperative period,including preoperative short fasting, intraoperative epidural anesthesia, minimally invasive surgery,postoperative pain management and nutritional care[3-5]. Due to its significant advantages and safety,ERAS has developed rapidly over the past decade[6]. In recent years, ERAS has been applied to various surgical fields, including gastrectomy[7], cardiac surgery[8], esophageal cancer surgery and colorectal surgery[9,10].
Although the application of biologics in treating inflammatory bowel disease has changed treatment strategies, most patients with inflammatory bowel disease (IBD) still require surgery[11,12]. IBD patients are often malnourished and immunosuppressed, which increases the risk of postoperative complications and prolongs the postoperative hospital stay[13]. In addition, reoperation was required in a large population of IBD patients, which might not be suitable for minimally invasive surgery[14].Furthermore, patients with IBD might experience prolonged postoperative intestinal obstruction due to chronic inflammation of the intestinal wall[15]. Therefore, the application of ERAS in IBD surgery might be limited in these high-risk situations.
A few studies suggest the feasibility of ERAS for IBD patients[16]; however, work comparing the efficiency of ERAS in IBD and non-IBD patients is scant[17]. Therefore, the purpose of this meta-analysis was to evaluate the safety and efficacy of ERAS in IBD surgery.
MATERlALS AND METHODS
This meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement[18]. The PROSPERO registration ID is CRD42021238052, and the link is as follows:https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42021238052.
Literature search strategy
The PubMed, EMBASE and Cochrane Library databases were searched by two authors independently.The literature search was conducted on March 21, 2021. The search strategy focused on two key words:ERAS and IBD. The search strategy for ERAS was as follows:"enhanced recovery protocol" OR"enhanced recovery after surgery" OR "enhanced recovery" OR "fast track surgery" OR "fast track rehabilitation" OR "fast track" OR "FTS" OR "ERAS". The search strategy for IBD was as follows:"inflammatory bowel disease" OR "Crohn’s" OR "Crohn disease" OR "Crohn’s disease" OR "ulcerative colitis"OR "colitis" OR "IBD" OR "CD" OR "UC". Then, we used “AND” to combine these two search strategies,and the publication language was restricted to English in this search.
I confess that I was fascinated by it, and for a week thought that nothing could be more desirable; the time passed like magic, so great was the charm of her society
Inclusion and exclusion criteria
The inclusion criteria were as follows:1, patients who underwent surgery for CD or UC; 2, the ERAS and non-ERAS protocols were both reported; and 3, reported at least one of the surgical outcomes,including operation time, complications, time to first flatus, time to bowel movement, postoperative hospital stay and readmission. The exclusion criteria were as follows:1, reviews, letters, case reports,comments or conferences; and 2, publications with insufficient data that could not be extracted. For studies with overlapping patient groups, the most recent study or the study with the larger sample size were included. Disagreement regarding inclusion and exclusion were resolved by discussion between the two authors.
Study selection
Data extraction
The data were extracted and cross-checked by two authors. The extracted data included first author,study date, study design, country, publishing year, patients’ baseline information, sample size,operation time, complications, time to first flatus, time to bowel movement, postoperative hospital stay and readmission.
Outcomes
63.Took away with them all the gold and silver that they could carry: Carrying away the treasures of the defeated antagonist118 is common in fairy tales, including Jack119 and the Beanstalk and Hansel and Gretel. While supporting the ideals of love, honor, and virtue, fairy tales are very practical, supporting the idea that heros need some degree of material wealth and security to live happily ever after.Return to place in story.
Quality assessment
The Newcastle-Ottawa Scale was used to evaluate the quality of the included studies[20]. High-quality studies are indicated by a score of 9 points, medium-quality studies have scores from 7-8 points, and low-quality studies have scores less than 7 points[21].
A large ship, with three masts, lay becalmed on the water, with only one sail set; for not a breeze stiffed, and the sailors sat idle on deck or amongst the rigging
Statistical analysis
In the current meta-analysis, continuous variables are presented as the mean ± standard deviation, and categorical variables are presented as proportions. For dichotomous and continuous variables, odds ratios (ORs) and mean differences (MDs) were calculated, and 95% confidence intervals (CIs) were calculated. Thevalue and the results of the chi-squared test were used to assess the statistical heterogeneity[22,23]. High heterogeneity was considered when> 50%; in such cases, the random effects model was used, and0.1 was considered statistically significant. The fixed effects model was used when≤ 50%, and0.05 was considered statistically significant. This meta-analysis was performed with RevMan 5.3 (The Cochrane Collaboration, London, United Kingdom).
RESULTS
Study selection
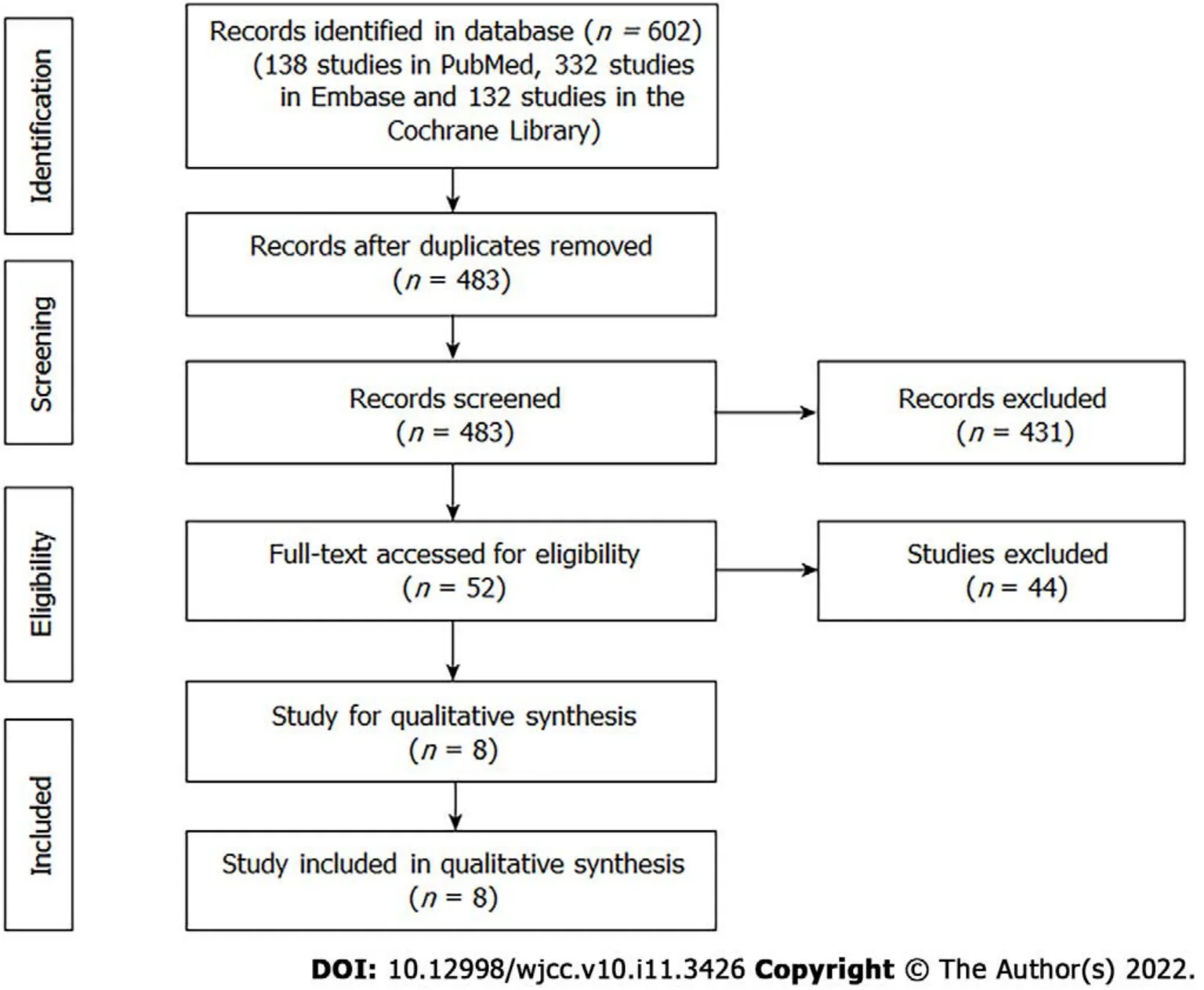
A total of 602 studies (138 studies in PubMed, 332 studies in EMBASE and 132 studies in the Cochrane Library) were retrieved in the initial search, and 483 studies were screened after excluding duplicated records. The titles and abstracts were screened, and then, 52 studies were left for full-text assessment.Finally, a total of eight studies[16,24-30] that compared the surgical outcomes of IBD patients between ERAS and non-ERAS protocols were included (Figure 1).
Patient characteristics and quality assessment of the included studies
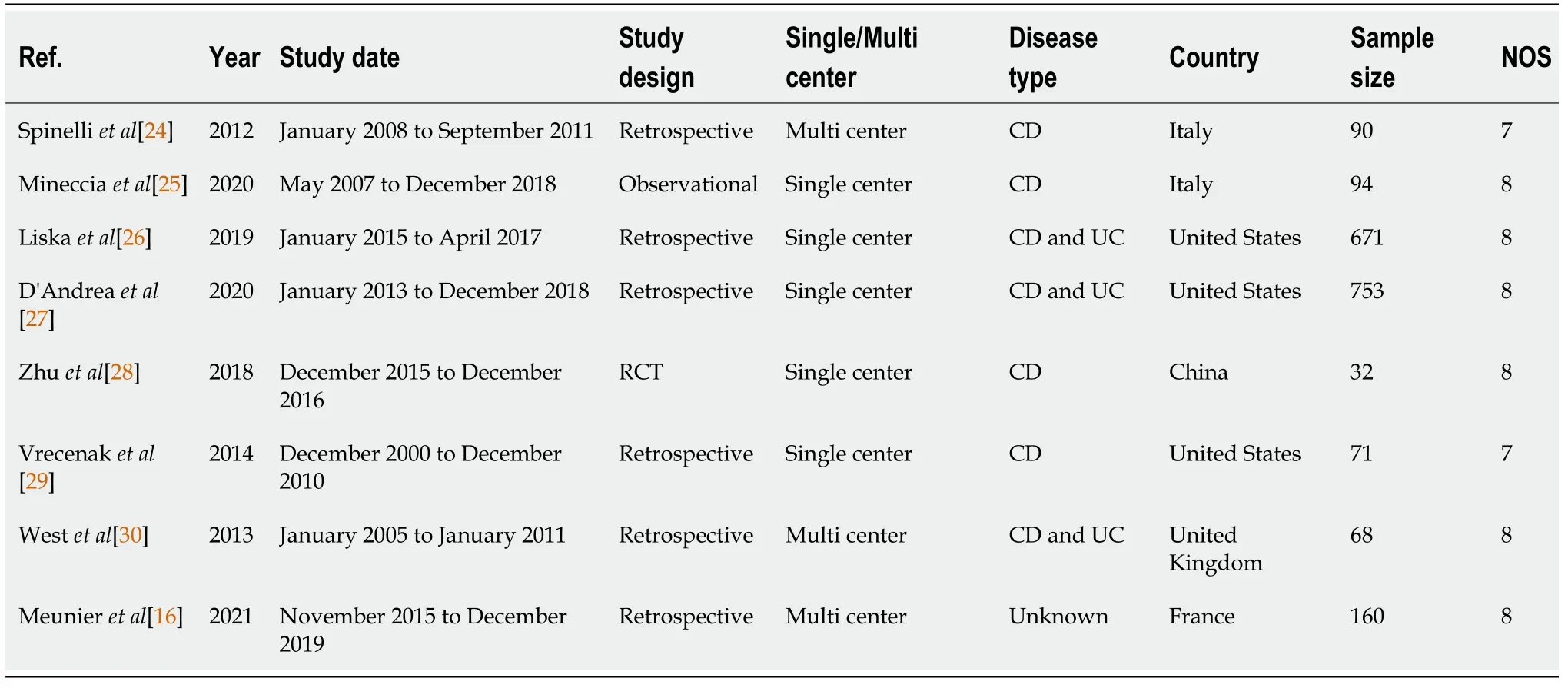
A total of eight studies including 1939 patients were included in this meta-analysis. The publication years ranged from 2012- 2021, and the study dates ranged from 2000-2019. There were six retrospective studies, one observational study and one randomized controlled trial (RCT). Three studies were conducted in United States, two studies were conducted in Italy, one study was conducted in China, one study was conducted in France and one study was conducted in the United Kingdom. The sample size and the scores of the Newcastle-Ottawa Scale of each study are shown in Table 1.
The primary outcome of the current meta-analysis was postoperative complications, which were graded based on the Clavien-Dindo classification[19]. Secondary outcomes included operation time, time to first flatus, time to bowel movement, postoperative hospital stays and readmission.
Baseline information
Then he turned to the princess: Tell us the truth, princess; who told you of this thing? I know it hair by hair, and in and out; but if I tell you what I know, who is there that can say I speak the truth? You must produce the person who can confirm my words
Complications
A total of eight studies with 1939 patients were included in this meta-analysis. There were no differences between the ERAS group and the non-ERAS group regarding baseline information. After pooling all of the data, no significance was found between the ERAS group and the non-ERAS group in terms of postoperative complications. However, the ERAS group had a lower prevalence of anastomotic fistula, less time to first flatus, less time to bowel movement and shorter postoperative hospital stays than the non-ERAS group.
Other surgical outcomes
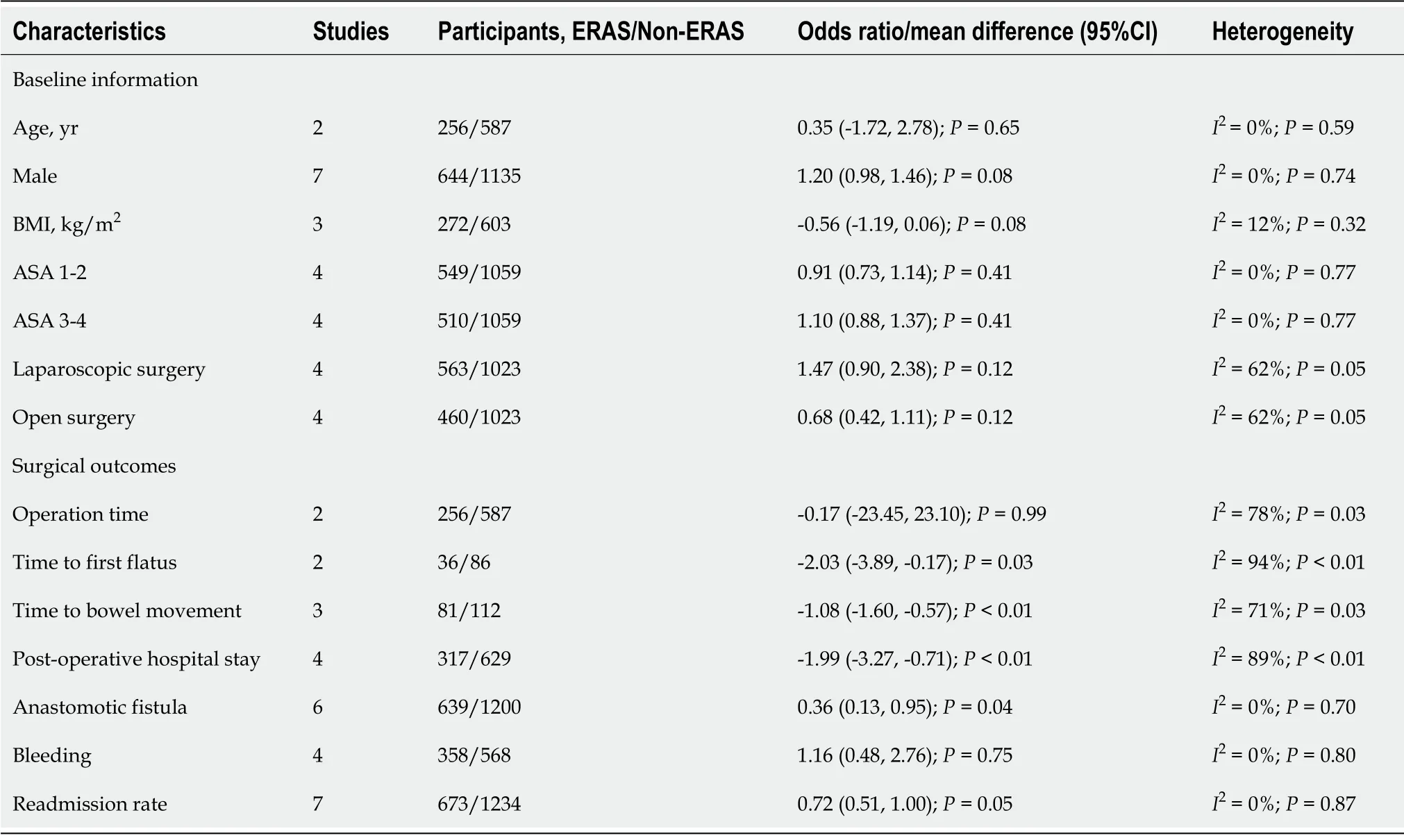
Other surgical outcomes were compared between the two groups as well. After pooling all of the data,the ERAS group had less time to first flatus (MD = -2.03, 95%CI = -3.89 to -0.17,= 0.03), less time to bowel movement (MD = -1.08, 95%CI = -1.60 to -0.57,0.01), less anastomotic fistula (OR = 0.36,95%CI = 0.13 to 0.95,= 0.04) and less postoperative hospital stay (MD = -1.99, 95%CI = -3.27 to -0.71,0.01) than the non-ERAS group. However, no significant difference was found in operation time (MD= -0.17, 95%CI = -23.45 to 23.10,= 0.99), bleeding (OR = 1.16, 95%CI = 0.48 to 2.76,= 0.75) or readmission rate (OR = 0.72, 95%CI = 0.51 to 1.00,= 0.05) (Table 2).
Oh, cried the Prince, not one of you is good for anything at all! There is a beggar-girl sitting outside the window, and I ll be bound that she can wash better than any of you! Come in, you girl there! he cried
Publication bias
The PubMed, EMBASE and Cochrane Library databases were searched from inception to March 21,2021 to find eligible studies. The primary outcome was the postoperative complications. The secondary outcomes included operation time, time to first flatus, time to bowel movement, postoperative hospital stay and readmission.
She saw the fruits in the garden ripen60 till they were gathered, the snow on the tops of the mountains melt away; but she never saw the prince, and therefore she returned home, always more sorrowful than before
DlSCUSSlON
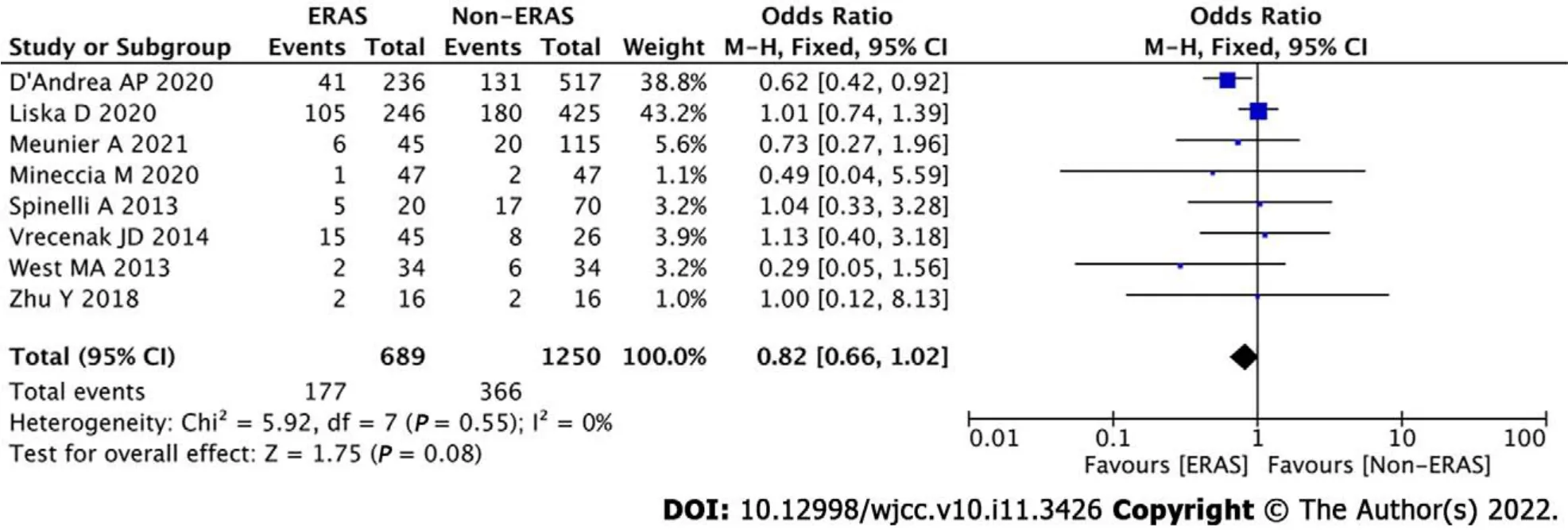
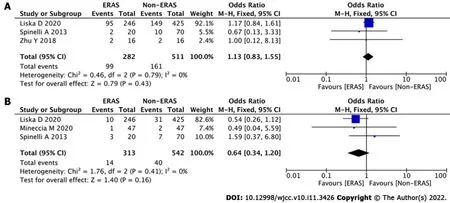
Data regarding overall complications were extracted from the eight studies. After pooling all of the data,no significance was found between the ERAS group and the non-ERAS group (OR = 0.82, 95%CI = 0.66 to 1.02,= 0.08) (Figure 2). To analyze differences in minor and major complications, we conducted subgroup analysis. However, there were no significant differences between the ERAS group and the non-ERAS group in terms of minor complications (OR = 1.13, 95%CI = 0.83 to 1.55,= 0.43) (Figure 3A)or major complications (OR = 0.64, 95%CI = 0.34 to 1.20,= 0.16) (Figure 3B).
IBD patients were at a higher risk of complications due to frequent malnutrition, immunosuppression, intra-abdominal abscess, anemia, fistula and intestinal obstruction than patients without IBD[27]. IBD patients who underwent surgery were more likely to have longer hospital stay, increased postoperative wound infections and higher readmission rates[15,31]. Furthermore, a longer pain relief time and a higher incidence of postoperative intestinal obstruction occurred in IBD patients[15].Therefore, the ERAS protocol seemed to be a challenging task in IBD patients.
In this meta-analysis, we observed that no significance was found between the ERAS group and the non-ERAS group in terms of postoperative complications, and the results were similar to those of previous studies[24-26].ERAS did not increase the complications after IBD surgery, so ERAS was considered a safe protocol. On the other hand, the ERAS group had a lower likelihood of anastomotic fistula, less time to first flatus, less time to bowel movement and shorter postoperative hospital stays than the non-ERAS group. ERAS might be an effective protocol after IBD surgery. The reduction in hospital stay brings cost savings and reduces the lost work time of family members, improves patient comfort and reduces exposure to hospital-acquired infections at the same time[17]. Moreover, the likelihood anastomotic fistula was significantly reduced in the ERAS group, which confirmed the safety of the ERAS protocol.
A reduction in hospital expenses in ERAS has been reported in other surgeries, including gastric cancer[7], colorectal cancer and esophagus cancer[9,10]. A previous study reported a reduction in hospital expenses; however, the number of studies was not sufficient to be included in this metaanalysis[28]. There was a lack of analgesic use, which required more follow-up studies confirming the beneficial details of ERAS.
A recent study reported that cancer patients undergoing laparoscopic surgery and ERAS treatment might have an immunological advantage[32]. Although no present studies evaluated the immune status of IBD patients undergoing the ERAS protocol, it is interesting to see whether similar benefits could be observed in the future. The success of ERAS depended on the patient's compliance and motivation, and this was important for IBD patients, who were mostly young and often had an active lifestyle[33,34].Such preferred patients require rapid recovery in order to return to work and social activities quickly. It was also important to involve the patient's caregivers, as they could play an important role in identifying any signs and symptoms after the patient was discharged[24].
There were some certain limitations in the current meta-analysis. First, only eight studies (one RCT and seven non-RCTs) were included. Second, the number of subgroup analyses of time to first flatus,time to bowel movement, operation time and postoperative hospital stay were relatively small,therefore, the results were not robust, and larger studies are needed. Third, differences might occur between primary or recurrent IBD patients who underwent surgery, and furthermore, the outcomes might differ from CD and UC. Fourth, the use of steroids and biologics might affect the surgical outcomes. Therefore, multicenter, multiregional, prospective and high-quality RCTs should be carried out in the future.
CONCLUSlON
In conclusion, ERAS was effective for the quicker recovery in IBD surgery and did not lead to increased complications.
ARTlCLE HlGHLlGHTS
Research background
To reduce surgical pressure and accelerate postoperative functional recovery, enhanced recovery after surgery (ERAS) has been recommended. Although the application of biologics in treating inflammatory bowel disease has changed treatment strategies, most patients with inflammatory bowel disease (IBD)still require surgery.
Research motivation
Many patients with IBD require surgery. The motivation of this meta-analysis was to examine the effect of ERAS in IBD surgery.
Relish8 the moment is a good motto, especially when coupled withe the Psalm9 118:24: This is the day which the Lord hath made, we will rejoice and be glad in it
Research objectives
The aim of this meta-analysis was to evaluate the advantage of ERAS in IBD surgery.
Research methods
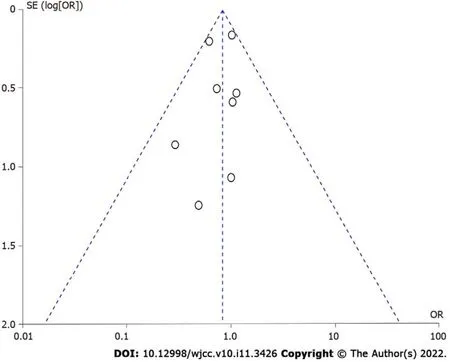
Repeated meta-analysis was performed by excluding one study at a time, and the exclusion of any one study did not significantly alter the results. Publication bias for the included studies was based on a visual inspection of the funnel plot. The funnel plot was symmetrical, and no obvious publication bias was found (Figure 4).
Research results
A total of eight studies involving 1939 patients were included in this meta-analysis. There was no difference in baseline information between the ERAS group and the non-ERAS group. No significant difference was found between the ERAS group and the non-ERAS group in terms of postoperative overall complications. The ERAS group had a lower prevalence of anastomotic fistula, less time to first flatus, less time to bowel movement and shorter postoperative hospital stays than the non-ERAS group.
Research conclusions
ERAS was effective for the quicker recovery in IBD surgery and did not lead to increased complications.
When he had finished his tale, she was filled with pity and said: Last week, when I was fishing, my net suddenly grew very heavy, and when I drew it in I found a great copper25 vase, fastened with lead
Research perspectives
This meta-analysis provided a preliminary conclusion on the effect of ERAS in IBD surgery. Therefore,multicenter, multiregional, prospective and high-quality randomized controlled trials should be carried out in the future.
The databases were searched by the two authors. First, the titles and abstracts were screened for relevant studies. Second, the full texts were evaluated based on the inclusion and exclusion criteria.Disagreements were discussed, and a final judgment was made by a third author if disagreement occurred.
Me: How s the salmon2?Server: Fantastic!Me: Does it come with rice?Server: Absolutely!Would a good and a yes have been sufficient? Undeniably!At Starbucks, the smallest coffee you can order is a Tall
The baseline information, including age, sex, body mass index, American Society of Anesthesia and surgical methods, was pooled, and no differences were found between the ERAS group and the non-ERAS group. The summary meta-analysis of baseline information in each study is shown in Table 2.
Tang H and Ji GY are co-corresponding authors; Peng D, Tang H and Ji GY contributed to the quality assessments; Cheng YX and Tao W contributed to data extraction; Peng D, Tao W and Cheng YX contributed to data analysis; Peng D contributed to writing the original draft; Peng D, Tang H and Ji GY contributed to writing and editing; All authors read and approved the final manuscript.
The authors declare that they have no competing interests.
The authors have read the PRISMA 2009 Checklist, and the manuscript was prepared and revised according to the PRISMA 2009 Checklist.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See:https://creativecommons.org/Licenses/by-nc/4.0/
China
Dong Peng 0000-0003-4050-4337; Yu-Xi Cheng 0000-0002-9220-7855; Wei Tao 0000-0002-3149-0642; Hua Tang 0000-0001-5068-1391; Guang-Yan Ji 0000-0003-4088-9636.
Ma YJ
They were all lost in admiration10 of the bird s beautiful plumage, and one forward youth, who was covered with clay from head to foot, called out, Oh, if I d only one of those feathers how happy I should be! Pull one out then, said Peter kindly, and the youth seized one from the bird s tail; instantly the swan screamed, and Peter called out, Swan, hold fast, and do what he could the poor youth couldn t get his hand away
Filipodia
It was a fine September night, with a silver moon riding high. They washed up the supper dishes and then took their chairs out onto the porch. I ll get my fiddle1(), said the old man, and play you some of the old tunes3.
Ma YJ
 World Journal of Clinical Cases2022年11期
World Journal of Clinical Cases2022年11期
- World Journal of Clinical Cases的其它文章
- Pleomorphic adenoma of the left lacrimal gland recurred and transformed into myoepithelial carcinoma after multiple operations:A case report
- Thyrotoxicosis after a massive levothyroxine ingestion:A case report
- Contrast-enhanced ultrasound manifestations of synchronous combined hepatocellular-cholangiocarcinoma and hepatocellular carcinoma:A case report
- Papillary thyroid microcarcinoma with contralateral lymphatic skip metastasis and breast cancer:A case report
- Del(5q) and inv(3) in myelodysplastic syndrome:A rare case report
- Ultrasound-guided local ethanol injection for fertility-preserving cervical pregnancy accompanied by fetal heartbeat:Two case reports