女性高血壓患者月經初潮年齡、絕經年齡及生殖期與認知功能的關系
2023-11-13 07:06:30游春嬌徐艷杰余超祝玲娟王濤周偉鮑慧慧程曉曙
中國醫學科學院學報 2023年5期
關鍵詞:認知功能
游春嬌 徐艷杰 余超 祝玲娟 王濤 周偉 鮑慧慧 程曉曙

基金項目:國家科技支撐計劃(2011BAI11B01)、江西省衛生健康委科技計劃項目(202210495)和江西省青年科學基金(2018BAB215003)
摘要:目的? 探討女性高血壓患者的月經初潮年齡、絕經年齡及生殖期與認知功能的關系。方法? 2018年7至8月在江西省婺源縣開展高血壓篩查,通過面對面問卷調查、體格測量及生化檢測收集信息,利用簡易精神狀態檢查量表(MMSE)評判認知功能。采用多重線性回歸法和Logistic回歸分析法分析月經初潮年齡、絕經年齡及生殖期對認知功能的影響,并采用懲罰樣條法進行曲線關系擬合。結果? 自然絕經女性高血壓患者4595例,平均年齡(65.1±8.4)歲,平均月經初潮年齡、絕經年齡及生殖期分別為(16.6±2.2)、(48.2±5.0)歲和(31.7±5.5)年,平均MMSE得分(19.0±6.3)分。認知功能障礙總檢出率40.4%(1859/4595)。月經初潮年齡<15歲、15~16歲及≥17歲組患者的認知功能障礙檢出率分別為28.4%、39.1%和45.8%,絕經年齡<45歲、45~49歲及≥50歲組患者的認知功能障礙檢出率分別為47.9%、39.7%和38.3%,生殖期<25年、25~29年、30~34年及≥35年組患者的認知功能障礙檢出率分別為56.0%、44.4%、40.6%和32.6%,不同年齡組間認知功能障礙檢出率差異均有統計學意義(P均<0.05)。與月經初潮年齡<15歲組比較,月經初潮年齡15~16歲、≥17歲組檢出認知功能障礙的比例較高(OR=1.45,95%CI=1.19~1.75,P<0.001;OR=1.65,95%CI=1.37~1.98,P<0.001);與絕經年齡<45歲組比較,絕經年齡45~49歲、≥50歲組檢出認知功能障礙的比例較低(OR=0.80,95%CI=0.66~0.95,P=0.013;OR=0.78,95%CI=0.65~0.93,P<0.001);與生殖期<25年組比較,生殖期25~29年、30~34年及≥35年組檢出認知功能障礙的比例較低(OR=0.66,95%CI=0.52~0.84,P<0.001;OR=0.62,95%CI=0.50~0.76,P<0.001;OR=0.51,95%CI=0.41~0.63,P<0.001)。結論? 月經初潮年齡與認知功能障礙的檢出呈正相關,而絕經年齡、生殖期與認知功能障礙的檢出呈負相關。
關鍵詞:月經初潮;絕經;生殖期;年齡;認知功能
中圖分類號: R544.1? 文獻標志碼: A? 文章編號:1000-503X(2023)05-0760-08
DOI:10.3881/j.issn.1000-503X.15544
Relationship of Cognitive Function With Menarche Age,Menopause Age,and Reproductive Period in Female Patients With Hypertension
YOU Chunjiao1,XU Yanjie1,YU Chao2,ZHU Lingjuan2,WANG Tao2,ZHOU Wei2,BAO Huihui1,CHENG Xiaoshu1
1Department of Cardiovascular Medicine,2Center for Prevention and Treatment of Cardiovascular Diseases,The Second Affiliated Hospital of Nanchang University,Nanchang 330006,China
Corresponding author:ZHOU Wei? Tel:0791-86296098,E-mail:z-w677@163.com
ABSTRACT:Objective? To explore the relationship of menarche age,menopause age,and reproductive period with cognitive function in the female patients with hypertension.Methods? Hypertension screening was carried out in Wuyuan county of Jiangxi province from July to August in 2018.Data were collected through a face-to-face questionnaire survey,physical measurement,and biochemical tests.The cognitive function was scored according to the mini-mental state examination(MMSE)scale.Multiple linear regression and Logistic regression were employed to analyze the effects of menarche age,menopause age,and reproductive period on cognitive function,and the penalized spline regression to fit the curves.Results? A total of 4595 postmenopausal women with hypertension were included in the analysis,with the mean age of(65.1±8.4)years,mean menarche age of(16.6±2.2)years,mean menopause age of(48.2±5.0)years,mean reproductive period of(31.7±5.5)years,mean MMSE score of(19.0±6.3)points,and total cognitive impairment detection rate of 40.4%(1859/4595).The detection rates of cognitive impairment were 28.4%,39.1%,and 45.8% in the females with the menarche ages of <15,15-16,and ≥17 years,47.9%,39.7%,and 38.3% in the females with the menopausal ages of <45,45-49,and ≥50 years,and 56.0%,44.4%,40.6%,and 32.6% in the females with the reproductive periods of <25,25-29,30-34,and ≥35 years,respectively.Moreover,the detection rates of cognitive impairment among different age groups were statistically significant(all P<0.05).Compared with the group with the menarche age <15 years,the groups with the menarche ages of 15-16 years and ≥17 years showed increased detection rates of cognitive impairment(OR=1.45,95%CI=1.19-1.75,P<0.001;OR=1.65,95%CI=1.37-1.98,P<0.001).Compared with the group with the menopausal age <45 years,the groups with the menopausal ages of 45-49 years and ≥50 years showed decreased detection rates of cognitive impairment(OR=0.80,95%CI=0.66-0.95,P=0.013;OR=0.78,95%CI=0.65-0.93,P<0.001).Compared with the group with the reproductive period <25 years,the groups with the reproductive periods of 25-29,30-34,and ≥35 years showed decreased detection rates of cognitive impairment(OR=0.66,95%CI=0.52-0.84,P<0.001;OR=0.62,95%CI=0.50-0.76,P<0.001;OR=0.51,95%CI=0.41-0.63,P<0.001).Conclusion? The detection rate of cognitive impairment had a positive correlation with menarche age and negative correlations with menopause age and reproductive period in the female patients with hypertension.
Key words:menarche;menopause;reproductive period;age;cognitive function
Acta Acad Med Sin,2023,45(5):760-767
據估計,全球約有5000萬人患有癡呆癥等嚴重認知功能障礙,預計到2050年,這一數字將增加兩倍[1]。認知功能障礙的日益加劇已成為全球面臨的一個重大挑戰,對個人、家庭和社會造成了嚴重的負擔,目前尚無有效的治療方法[2]。既往研究表明,女性的生殖因素(包括月經初潮年齡、絕經年齡及生殖期等)與認知功能障礙的發生風險相關,但結論不一[3-5]。且針對我國女性尤其是高血壓群體的相關研究較少。本研究擬探討我國女性高血壓患者月經初潮年齡、絕經年齡及生殖期與認知功能的關系。
對象和方法
研究對象? 來源于中國H型高血壓注冊登記研究(注冊號:ChiCTR1800017274),納入標準:18周歲及以上;確診為高血壓;意識清楚。排除標準:患精神或神經系統疾病,無法表達意愿者;不愿配合調查者。于2018年7至8月在江西省婺源縣開展高血壓篩查,共檢出高血壓患者14 234例,其中4 595例自然絕經女性高血壓患者納入分析。本研究通過南昌大學第二附屬醫院倫理委員會批準(審批號:研臨審〔2018〕第19號-1),研究對象均簽署知情同意書。
調查方法? 采用面對面問卷調查,收集患者人口學特征、生活方式、既往病史等信息;體格檢查測量身高、腰圍、體重及血壓等;采集空腹血樣,檢測血糖、總膽固醇(total cholesterol,TC)、甘油三酯(triglyceride,TG)、高密度脂蛋白膽固醇(high-density lipoprotein cholesterol,HDL-C)、低密度脂蛋白膽固醇(low-density lipoprotein cholesterol,LDL-C)、血漿同型半胱氨酸及肝腎功能等生化指標。使用簡易精神狀態檢查量表(mini-mental state examination,MMSE)評估認知功能,包括定向力、即刻記憶力、注意力和計算力、短程記憶力、語言能力5個維度。該量表共設30個條目,每個條目回答正確得1分,回答錯誤或拒絕回答得0分,總分30分。
指標定義? (1)高血壓:在未使用降壓藥物的情況下,非同日3次血壓測量平均收縮壓(systolic blood pressure,SBP)≥140 mmHg(1 mmHg=0.133 kPa)和/或舒張壓(diastolic blood pressure,DBP)≥90 mmHg;或患者既往患有高血壓,目前正在使用降壓藥[6]。(2)糖尿病:自報確診有糖尿病病史、服用糖尿病藥物或空腹血糖≥7.0 mmol/L[7]。(3)腦卒中:自報在二級及以上醫院確診為腦卒中病史。(4)血脂異常:TC≥6.2 mmol/L或TG≥2.3 mmol/L或HDL-C<1.0 mmol/L或LDL-C≥4.1 mmol/L,或自報在過去2周內服用降脂藥物[8]。(5)文化程度分為文盲、小學、中學、大學及以上(含大專)。(6)體重指數(body mass index,BMI):體重(kg)/身高(m)2。(7)目前吸煙:指每天至少1支,滿1年以上,或累計18包/年以上,包括吸香煙和/或煙葉(手卷煙等)[9]。(8)目前飲酒:指平均每周飲酒≥2次并持續1年以上,包括飲用啤酒、白酒、葡萄酒、黃酒、米酒及其他酒類[10]。(9)睡眠時長分為<5 h、5~8 h、>8 h。(10)服藥情況:詢問患者過去3個月是否使用降壓、降糖、降脂藥物(累計時間大于7 d),并記錄藥物具體名稱、用法用量、累計使用時間等。(11)女性月經和生育史:通過詢問您第一次來月經的年齡是多大(歲)?您平均多長時間來一次月經?您的月經是否規律?您來月經時有痛經嗎?您絕經(自然絕經)了嗎?絕經時年齡是多大歲數?您是否服用避孕藥(>半年)?您共懷孕過幾次(包括所有流產、引產、活產數)?您有過人工流產嗎?您有過自然流產嗎?等問題收集信息。月經初潮年齡分為<15歲、15~16歲及≥17歲組,絕經年齡分為<45歲、45~49歲及≥50歲組[11]。(12)生殖期:為絕經年齡與月經初潮年齡之差,分為<25年、25~29年、30~34年及≥35年組[11]。(13)MMSE認知功能評判:根據患者的文化背景,評判患者認知功能。文盲得分≤17分,小學得分≤20分,中學得分≤22分,大專及以上得分≤23分為認知功能障礙[12-13]。
質量控制? 使用統一的調查問卷問詢,采用標準工具測量身體指標。所有調查人員經過嚴格規范的培訓,并考核合格上崗。質控小組對調查現場流程、問卷質量等進行質控,發現問題及時復核更正。生化指標由專業機構按統一標準進行測定。數據采用雙錄入進行核驗。
統計學處理? 采用EpiData 3.2軟件錄入數據,SPSS 26.0統計軟件分析數據。定量資料符合正態分布或近似正態分布時,以均數±標準差表示,組間比較采用t檢驗或方差分析;定性資料采用頻數或構成比表示,組間比較采用χ2檢驗。采用Logistic回歸法和多重線性回歸法進行多因素分析。多因素分析模型中校正的因素依據以下原則納入:(1)參考其他文獻中校正的因素,如既往系統評價文獻報道認知功能障礙的影響因素包括年齡、吸煙、糖尿病、收縮壓、舒張壓、降壓藥、同型半胱氨酸水平[14],調查研究也發現TG、HDL-C[15]、睡眠時長[16]及月經初潮年齡、絕經年齡、生殖期、懷孕情況、流產情況、口服避孕藥等生殖因素[3]與認知功能障礙有關聯;(2)單因素分析有統計學意義的因素,包括BMI、腰圍、LDL-C、估算腎小球濾過率(estimated glomerular filtration rate,eGFR)、血脂異常、服用降脂藥、月經周期、痛經;(3)臨床上可能對認知功能有影響的因素(腦卒中)。本研究在多因素回歸模型中,校正了年齡、BMI、腰圍、收縮壓、舒張壓、同型半胱氨酸、TG、HDL-C、LDL-C、eGFR、目前吸煙、糖尿病、腦卒中、血脂異常、服用降壓藥、服用降脂藥、月經周期、痛經、懷孕次數、人工流產、服用避孕藥、睡眠時長等因素。采用懲罰樣條法[17-18]進行月經初潮年齡、絕經年齡及生殖期與認知功能障礙之間的平滑曲線擬合,探討是否存在非線性關系,求P非線性值。P<0.05為差異有統計學意義。
結果
基本情況? 4595例自然絕經女性高血壓患者平均年齡(65.1±8.4)歲,平均月經初潮年齡(16.6±2.2)歲,平均絕經年齡(48.2±5.0)歲,平均生殖期(31.7±5.5)年,平均MMSE得分(19.0±6.3)分,認知功能障礙總檢出率40.4%(1859/4595)。月經初潮年齡<15歲、15~16歲及≥17歲組認知功能障礙檢出率分別為28.4%、39.1%和45.8%,絕經年齡<45歲、45~49歲及≥50歲組認知功能障礙檢出率分別為47.9%、39.7%和38.3%,生殖期<25年、25~29年、30~34年及≥35年組認知功能障礙檢出率分別為56.0%、44.4%、40.6%和32.6%,不同年齡組間認知功能障礙檢出率差異均有統計學意義(P均<0.05)。
與不伴認知功能障礙組比較,伴認知功能障礙組患者年齡、月經初潮年齡、收縮壓、同型半胱氨酸、HDL-C較高,目前吸煙、月經周期<30 d、痛經、懷孕次數>3次、睡眠時長>8 h的比例較大,而絕經年齡、生殖期、MMSE得分、BMI、腰圍、舒張壓、TG、LDL-C、eGFR較低,糖尿病、血脂異常、服用降壓藥、服用降脂藥、人工流產、服用避孕藥的比例較小(P均<0.05)(表1)。
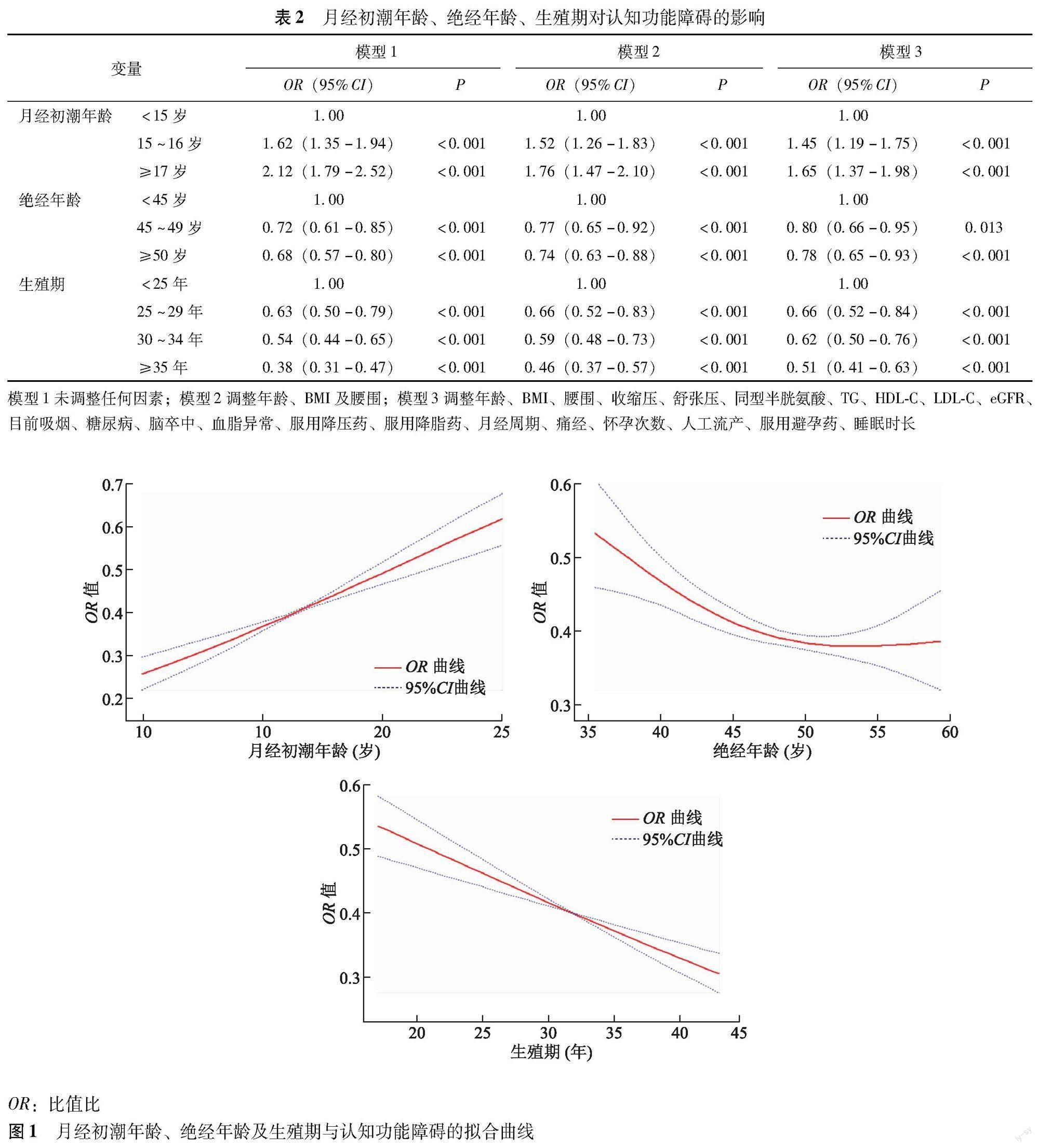
月經初潮年齡、絕經年齡、生殖期對認知功能的影響? 以MMSE得分為因變量進行多重線性回歸分析,控制其他因素后,結果顯示月經初潮年齡與MMSE得分呈負相關(β=-0.31,95%CI=-0.39~0.23),而絕經年齡、生殖期與MMSE得分呈正相關(β=0.11,95%CI=0.07~0.15;β=0.12,95%CI=0.09~0.15)。以認知功能障礙為因變量進行Logistic回歸分析,控制其他因素后完全調整模型(模型3)結果顯示,與月經初潮年齡<15歲組比較,月經初潮年齡15~16歲、≥17歲組檢出認知功能障礙的比例較高(OR=1.45,95%CI=1.19~1.75,P<0.001;OR=1.65,95%CI=1.37~1.98,P<0.001);與絕經年齡<45歲組比較,絕經年齡45~49歲、≥50歲組檢出認知功能障礙的比例較低(OR=0.80,95%CI=0.66~0.95,P=0.013;OR=0.78,95%CI=0.65~0.93,P<0.001);與生殖期<25年組比較,生殖期25~29年、30~34年及≥35年組檢出認知功能障礙的比例較低(OR=0.66,95%CI=0.52~0.84,P<0.001;OR=0.62,95%CI=0.50~0.76,P<0.001;OR=0.51,95%CI=0.41~0.63,P<0.001)(表2)。
月經初潮年齡、絕經年齡、生殖期與認知功能障礙關系的曲線擬合? 懲罰樣條法曲線關系擬合結果顯示,月經初潮年齡與認知功能障礙的檢出呈正相關(P非線性=0.375),而絕經年齡(P非線性=0.244)、生殖期(P非線性=0.286)與認知功能障礙的檢出呈負相關,且均為線性相關(圖1)。
討論
認知功能障礙是指由多種原因引起的認知功能多領域、不同程度的損傷,其持續惡化將會導致癡呆等嚴重健康問題。隨著我國老齡化的日益加劇,老年人的認知功能障礙問題越來越突出。癡呆已成為繼心血管病、腦血管病和腫瘤之后的第四大危害老年人健康的疾病[19],給個人、家庭和社會造成了沉重的經濟負擔。既往國內研究報道,我國女性認知功能障礙檢出率為32.2%[20],太原市為49.8%[21]、蘇州市為20.8%[22]、沈陽市為33.9%[23]以及銀川市為32.2%[24]。本研究中女性高血壓患者認知功能障礙檢出率為40.4%,略高于國內其他地區,可能與本組研究人群為高血壓患者,而高血壓可導致認知功能損害有關[25-26]。研究發現女性月經初潮與高血壓存在關聯[27-28];與絕經前相比,女性絕經后高血壓發生比例更高且危害較大[29],常與慢性低度炎癥、氧化應激、內皮功能障礙等諸多危險因素相關[30-31]。因此,有必要在絕經女性高血壓患者中對月經初潮、絕經與認知功能損害的關系進行探討,以便為防控工作提供指導。
現有一些研究探討了月經初潮年齡、絕經年齡及生殖期等生殖因素對認知功能的影響。一項關于美國15 754名女性的前瞻性隊列調查研究顯示,月經初潮晚、絕經年齡小、生殖期短均與癡呆癥的風險升高有關[32]。Song等[33]對8 222名新加坡華人女性的研究報道顯示,絕經早、生育期短的女性癡呆或阿爾茨海默病發生的風險升高。Gong等[3]通過對來自英國生物樣本庫273 240名女性隨訪11.8年發現,月經初潮晚、早期自然絕經、較短的生殖期都與癡呆風險升高相關。日本一項研究也顯示,較長的生殖期與認知障礙呈顯著負相關[34]。一項對我國北方農村4 275名≥65歲的絕經女性調查發現,月經初潮年齡大、絕經早、生殖期短會增加輕度認知功能障礙、癡呆和阿爾茨海默病的風險[35]。Heys等[36]對來自廣州生物庫隊列研究的11 094名自然絕經后≥50歲女性數據分析發現,生殖期長的女性認知功能更好。Li等[37]對浙江重大公共衛生監測數據的分析發現,4 796名絕經女性中較長的生育期與認知功能障礙風險的降低相關。Chou等[38]對我國臺灣地區的調查顯示,月經初潮年齡晚的女性認知功能障礙風險高。然而,部分研究也發現了相反的結論。對北歐3 601名絕經女性隨訪6.3年發現,在至少有1個APOE4等位基因的女性中,較長的生殖周期與癡呆癥風險的增加相關,但在非攜帶者中沒有相關性[39]。另一項針對瑞典女性隨訪44年的縱向研究顯示,自然絕經女性中生殖期長、絕經晚和癡呆、阿爾茨海默病的高風險相關,但癡呆與月經初潮年齡無關[40]。此外,一項在拉丁美洲和中國65歲及以上女性人群中進行的隊列研究發現,月經初潮年齡、絕經年齡及生殖期均與癡呆的發生沒有關聯[5]。我國臺灣一項研究表明,生殖期與認知功能障礙無關[38]。Bove等[41]報道自然絕經的女性中絕經年齡與認知功能無關。由此可見,目前相關研究結論不一,有必要在更多地域的人群中進一步深入研究。另外,既往研究的調查對象主要是正常女性人群。本研究針對我國女性高血壓患者這一認知功能障礙的高危人群進行分析,結果發現月經初潮年齡與認知功能障礙的風險呈正相關,而絕經年齡、生殖期與認知功能障礙呈負相關。研究結果為我國女性高血壓人群認知功能障礙的防控提供了理論依據。
生殖因素對認知功能影響的具體機制尚不清楚,可能原因是月經初潮越早、自然絕經越晚即生殖期越長,意味著高雌激素水平在體內暴露的時間越長,一方面雌激素具有神經保護作用,另一方面月經期女性周期性產生的孕酮,也具有神經保護特征[42],但其具體機制有待進一步的研究。
本研究不足之處在于樣本來源于單一區域,研究結論推廣性受到限制;此外,本研究為橫斷面調查,相關生殖因素與認知功能障礙的因果關系尚需前瞻性研究驗證。
綜上,本研究結果表明,月經初潮年齡與認知功能障礙的檢出呈正相關,絕經年齡、生殖期與認知功能障礙的檢出呈負相關。女性保持較長的生殖時間可以預防癡呆風險。
參考文獻
[1]Porsteinsson AP,Isaacson RS,Knox S,et al.Diagnosis of early Alzheimers disease:clinical practice in 2021[J].J Prev Alzheimers Dis,2021,8(3):371-386.DOI:10.14283/jpad.2021.23.
[2]Livingston G,Huntley J,Sommerlad A,et al.Dementia prevention,intervention,and care:2020 report of the Lancet Commission[J].Lancet,2020,396(10248):413-446.DOI:10.1016/S0140-6736(20)30367-6.
[3]Gong J,Harris K,Peters SAE,et al.Reproductive factors and the risk of incident dementia:a cohort study of UK biobank participants[J].PLoS Med,2022,19(4):e1003955.DOI:10.1371/journal.pmed.1003955.
[4]洪霞,張振馨,趙潔皓,等.內源性雌激素與阿爾茨海默病的病例對照研究[J].中華流行病學雜志,2001,22(5):379-382.DOI:10.3760/j.issn:0254-6450.2001.05.021.
[5]Prince MJ,Acosta D,Guerra M,et al.Reproductive period,endogenous estrogen exposure and dementia incidence among women in Latin America and China:a 10/66 population-based cohort study[J].PLoS One,28,13(2):e0192889.DOI:10.1371/journal.pone.0192889.
[6]中國高血壓防治指南修訂委員會,高血壓聯盟(中國),中華醫學會心血管病學分會,等.中國高血壓防治指南(2018年修訂版)[J].中國心血管雜志,2019,24(1):24-56.DOI:10.3969/j.issn.1007-5410.2019.01.002.
[7]中華醫學會糖尿病學分會.中國2型糖尿病防治指南(2020年版)[J].中華糖尿病雜志,2021,13(4):315-409.DOI:10.3760/cma.j.cn115791-20210221-00095.
[8]中國成人血脂異常防治指南修訂聯合委員會.中國成人血脂異常防治指南(2016年修訂版)[J].中國循環雜志,2016,31(10):937-950.DOI:10.3969/j.issn.1000-3614.2016.10.001.
[9]周子逸,李幼寶,秦獻輝,等.華東地區45~75歲農村高血壓人群吸煙與葉酸的相關性研究[J].中國預防醫學雜志,2017,18(6):406-410.DOI:10.16506/j.1009-6639.2017.06.002.
[10]於濤,王雯,王力煒,等.連云港農村地區男性高血壓人群中飲酒與血脂的相關性分析[J].中華疾病控制雜志,2016,20(4):370-373.DOI:10.16462/j.cnki.zhjbkz.2016.04.012.
[11]Yoo JE,Shin DW,Han K,et al.Female reproductive factors and the risk of dementia:a nationwide cohort study[J].Eur J Neurol,2020,27(8):1448-1458.DOI:10.1111/ene.14315.
[12]段金旗,任煒,殷秀霞,等.MMSE評估老年腦膠質瘤患者術前認知功能及影響因素[J].中國老年學雜志,2020,40(16):3406-3409.DOI:10.3969/j.issn.1005-9202.2020.16.015.
[13]Li J,Yu S,Tan Z,et al.High estimated glomerular filtration rate is associated with worse cognitive performance in the hypertensive population:results from the China H-type Hypertension Registry Study[J].Front Aging Neurosci,2022,13:706928.DOI:10.3389/fnagi.2021.706928.
[14]楊慧鋒,牛偉華,施月仙,等.慢性心力衰竭患者發生認知功能障礙影響因素的系統評價[J].中國全科醫學,2022,25(13):1642-1650.DOI:10.12114/j.issn.1007-9572.2022.0053.
[15]葉青芳,王旖旎,李玲,等.中青年高血壓住院患者輕度認知功能障礙發生現狀及影響因素研究[J].中國全科醫學,2023,26(2):154-159,167.DOI:10.12114/j.issn.1007-9572.2022.0576.
[16]韋慧燕,劉樂,楊光媚,等.我國老年人認知功能障礙現狀及其影響因素[J].醫學與社會,2022,35(2):55-59.DOI:10.13723/j.yxysh.2022.02.011.
[17]Li M,Zhan A,Huang X,et al.Positive association between triglyceride glucose index and arterial stiffness in hypertensive patients:the China H-type Hypertension Registry Study[J].Cardiovasc Diabetol,2020,19(1):139.DOI:10.1186/s12933-020-01124-2.
[18]Roshani D,Ghaderi E.Comparing smoothing techniques for fitting the nonlinear effect of covariate in Cox models[J].Acta Informatica Medica,2016,24(1):38-41.DOI:10.5455/aim.2016.24.38-41.
[19]管君花.臺州市60 歲以上人群老年癡呆發病情況及影響因素[J].醫學與社會,2018,31(6):52-54.DOI:10.13723/j.yxysh.2018.06.017.
[20]韋慧燕,劉樂,楊光媚,等.我國老年人認知功能障礙現狀及其影響因素[J].醫學與社會,2022,35(2):55-59.DOI:10.13723/j.yxysh.2022.02.011.
[21]劉路,秦瑤,李磊,等.太原市社區老年人認知功能現狀及影響因素分析[J].現代預防醫學,2020,47(12):2219-2223.
[22]盧晶夢.農村老年人認知功能現狀及影響因素研究[D].蘇州:蘇州大學,2017.
[23]劉東祺,李榮梅,張美琪,等.沈陽市社區老年人認知功能障礙現狀及影響因素分析[J].護理研究,2020,34(13):2390-2393.DOI:10.12102/j.issn.1009-6493.2020.13.027.
[24]張迪.銀川市 65 歲及以上老年人認知功能及影響因素流行病學調查研究[D].銀川:寧夏醫科大學,2020.
[25]Wang Z,Li N,Heizhati M,et al.Association between 24-h urinary sodium to potassium ratio and mild cognitive impairment in community-based general population[J].Public Health Nutr,2021,24(17):5795-5804.DOI:10.1017/S1368980021001452.
[26]Allen NB,Khan SS.Blood pressure trajectories across the life course[J].Am J Hypertens,2021,34(3):234-241.DOI:10.1093/ajh/hpab009.
[27]Zhou W,Wang T,Zhu L,et al.Association between age at menarche and hypertension among females in southern China:a cross-sectional study[J].Int J Hypertens,2019:9473182.DOI:10.1155/2019/9473182.
[28]Liu D,Qin P,Liu Y,et al.Association of age at menarche with hypertension in rural Chinese women[J].J Hypertens,2021,39(3):476-483.DOI:10.1097/HJH.0000000000002672.
[29]Lin YY,Lee SD.Cardiovascular benefits of exercise training in postmenopausal hypertension[J].Int J Mol Sci,2018,19(9):2523.DOI:10.3390/ijms19092523.
[30]Rossi R,Grimaldi T,Origliani G,et al.Menopause and cardiovascular risk[J].Pathophysiol Haemost Thromb,2002,32(5-6):325-328.DOI:10.1159/000073591.
[31]Scuteri A,Fleg JL.Hypertension in postmenopausal women as a medical and public health problem[J].High Blood Press Cardiovasc Prev,2003,10(1):51-55.DOI:10.2165/00151642-200310010-00010.
[32]Gilsanz P,Lee C,Corrada MM,et al.Reproductive period and risk of dementia in a diverse cohort of health care members[J].Neurology,2019,92(17):e2005-e2014.DOI:10.1212/WNL.0000000000007326.
[33]Song X,Wu J,Zhou Y,et al.Reproductive and hormonal factors and risk of cognitive impairment among Singapore Chinese women[J].Am J Obstet Gynecol,2020,223(3):410.e1-410.e23.DOI:10.1016/j.ajog.2020.02.032.
[34]Shimizu Y,Sawada N,Iwasaki M,et al.Japan public health center-based prospective study group.Reproductive history and risk of cognitive impairment in Japanese women[J].Maturitas,2019,128:22-28.DOI:10.1016/j.maturitas.2019.06.012.
[35]Xi H,Gan J,Liu S,et al.Reproductive factors and cognitive impairment in natural menopausal women:a cross-sectional study[J].Front Endocrinol,2022,13:893901.DOI:10.3389/fendo.2022.893901.
[36]Heys M,Jiang C,Cheng KK,et al.Life long endogenous estrogen exposure and later adulthood cognitive function in a population of naturally postmenopausal women from southern China:the guangzhou biobank cohort study[J].Psychoneuroendocrinology,2011,36(6):864-873.DOI:10.1016/j.psyneuen.2010.11.009.
[37]Li FD,He F,Chen TR,et al.Reproductive history and risk of cognitive impairment in elderly women:a cross-sectional study in eastern China[J].J Alzheimers Dis,2016,49(1):139-147.DOI:10.3233/JAD-150444.
[38]Chou HT,Wu PY,Huang JC,et al.Late menarche,not reproductive period,is associated with poor cognitive function in postmenopausal women in Taiwan[J].Int J Environ Res Public Health,2021,18(5):2345.DOI:10.3390/ijerph18052345.
[39]Geerlings MI,Ruitenberg A,Witteman JC,et al.Reproductive period and risk of dementia in postmenopausal women[J].JAMA,2001,285(11):1475-1481.DOI:10.1001/jama.285.11.1475.
[40]Najar J,stling S,Waern M,et al.Reproductive period and dementia:a 44-year longitudinal population study of Swedish women[J].Alzheimers Dement,2020,16(8):1153-1163.DOI:10.1002/alz.12118.
[41]Bove R,Secor E,Chibnik LB,et al.Age at surgical menopause influences cognitive decline and Alzheimer pathology in older women[J].Neurology,2014,82(3):222-229.DOI:10.1212/WNL.0000000000000033.
[42]Singh M,Su C.Progesterone-induced neuroprotection:factors that may predict therapeutic efficacy[J].Brain Res,2013,1514:98-106.DOI:10.1016/j.brainres.2013.01.027.
(收稿日期:2023-02-24)
猜你喜歡
山東體育學院學報(2016年5期)2017-01-18 20:58:33
中國醫藥導報(2016年29期)2016-12-27 11:10:00
中國實用醫藥(2016年29期)2016-12-26 09:42:28
中國當代醫藥(2016年28期)2016-12-20 17:42:35
中外醫學研究(2016年26期)2016-11-30 03:02:44
藝術科技(2016年9期)2016-11-18 16:23:08
中國現代醫生(2016年23期)2016-11-15 03:24:49
中國實用醫藥(2016年26期)2016-11-07 13:39:15
中國實用醫藥(2016年26期)2016-11-07 13:39:07
中國實用醫藥(2016年21期)2016-08-19 13:46:24
