Prognostic Value of Promoter Hypermethylation of Retinoic Acid Receptor Beta (RARB) and CDKN2 (p16/MTS1) in Prostate Cancer
2011-08-02 07:22:14AmeriAlidoostiHosseiniParvinEmranpourMHTaslimiSalehiFadavi
Ameri A, Alidoosti A, Hosseini Y, Parvin M, Emranpour MH, Taslimi F, Salehi E, Fadavi P
1Department of Radiation Oncology, Imam Hossein Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran; 2Department of Urology, Shahid Modarres Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran; 3Department of Pathology, Shahid Labbafinezhad Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran; 4Department of Radiation Oncology, Imam Hossein Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran; 5Department of Immunology, Faculty of Medicine, Tehran University of Medical Sciences, Tehran, Iran; 6Department of Radiation Oncology, Tehran University of Medical Sciences, Tehran, Iran
INTRODUCTION
As the most commonly diagnosed cancer (excluding skin cancer) among men, prostate cancer is a global public health problem.Previous studies showed about 27% of prostate cancer had poor prognosis and prostate cancer is the second leading cause of cancer-related deaths among men in North America and Western/Northern Europe[1-6].While many prostate cancer patients present with advanced disease, early detection with highly specific and sensitive methods might be one of the main approaches of reducing mortality[5-7].
Currently, prostate-specific antigen (PSA), histological grade [Gleason score (GS)] and stage of disease are widely used to predict the prognosis[8-10], but the tumor behavior is not always predictable using these factors.Genetic mechanisms of malignant changes are the pioneer events during disease process, long before the clinical factors appear[11].To date, more than 50 genes have been shown to be inactivated by promoter CpG island hypermethylation in prostate cancer[6].
In the recent years, a new group of cancer markers based on the characterization of epigenetic alterations are introduced to evaluate the tumors[12-15].Investigations on these epigenetic markers in tissue samples are mainly restricted to the evaluation of retrospective series of just a fraction of all prostate tumors.Amongst them, promoter CpG island methylation is mainly emerged as a putative prognostic assessment tool to seek some biological markers for aggressive prostate cancer[5,16-21].
Retinoic acid receptor beta(RARB,OMIM: 180220), andcyclin-dependent kinase inhibitor 2a(CDKN2a,p16/Cdkn2ink4/Mts1,OMIM: 600160) were widely reported to be hypermethylated in prostate cancer and some suggested their potential as diagnostic and prognostic markers[22-28].
Given the importance of finding a reliable prognostic marker, we investigated prognostic value of promoter hypermethylation ofRARBandp16genes in Iranian patients with prostate cancer with good and poor prognosis, in comparison to the patients affected with benign prostatic hyperplasia (BPH).
MATERIALS AND METHODS
Patients and Samples
In this case-control study, all participants were enrolled from men referred to the Radiotherapy-Oncology Ward in Imam Hossein Hospital, Urology Ward in Shahid Modarres Hospital, and Shahid Labbafinezhad Hospital due to clinically suspected prostate cancer from 2007 to 2008.
Prostate biopsy specimens were collected by surgery.If the pathologic studies confirmed the diagnosis of prostate cancer, the patient was included in the study.Included patients signed the informed consent form if they were candidates for prostatectomy.A 5 ml blood sample was taken to measure PSA level through routine lab procedures before surgery.Histologic slides from formalin-fixed and paraffinembedded tissue fragments were reviewed to confirm BPH or prostate cancer or to reassess GS of cancer cases by an expert in prostate diseases at the Department of Pathology,Shahid Labbafinezhad Hospital.Relevant clinical data, such as age, serum PSA level at diagnosis, and clinical stage of disease, were obtained from medical records.
Prostate cancer cases were divided into good and poor prognosis with respect to the serum PSA level, GS, and staging.PSA value more than 9, or GS summation equal or more than 7, or stage III and more, was considered as poor prognosis group, the rest with GS ≤6 and stage II, and PSA<10 were labeled as the good prognosis group.
Methods
The paraffin wax-embedded blocks, consisting of 42 cancerous and 21 BPH without cancer were prepared for methylation specific PCR (MSPCR) in our genetic laboratory to measure the degree of methylation.The genetic laboratory members were not informed of the prognostic situation of patients to which the paraffin blocks belong.
First, the DNA was extracted from tissue samples using the classical method of phenol/chloroform/isoamyl alcohol.Purified DNA samples were subjected to treatment with sodium bisulfite, which reacts with cytosine (C) bases in preference to methylated cytosine (5-mC) bases, facilitating the deamination of C to produce uracil (U) while 5-mC remains unchanged.Consequently, differences in DNA methylation become apparent as differences in DNA sequence.PCR primers specific for target sequences resulting from bisulfate modification of 5-mCpG-containing DNA are used for PCR to detect target methylated CpG island[29,30].
In brief, 40 μl of DNA (2 μg)was denatured at 97°C for 10 min, centrifuged briefly, and chilled on ice.Ten microlitres of 1 mol/L NaOH was then added and the mixture was stored at room temperature for 15 min.Then 500 μl of 3.5 mol/L sodium bisulphate and 1 mmol/L hydroquinone mixture was added to the denatured DNA, and stored at 55°C for 16 h.The treated DNA was purified using Wizard DNA purification resin (DNA clean up kit, Promega,Madison, WI, USA) according to the manufactures’instruction and desulphonated with 0.3 mol/L NaOH at room temperature for 10 min.After adding 2.5 volumes of 100% cold ethanol and a two-thirds volume of 7.5 mol/L ammonium acetate and storing at -20°C for 12 h, the precipitated DNA was centrifuged.After washing in 70%ethanol and drying, DNA was dissolved in 10 mmol/L Tris buffer.This process was performed twice for each sample in order to increase the amount of remaining DNA after bisulfit treatment.
There were 63 paraffin blocks treated with bisulfit before MSPCR.Subsequent to purification of modified DNA,methylation specific amplification was performed for evaluating methylation ofp16andRARBusing bisulphate-modified DNA (30-50 ng), primers specific for methylated and non-methylated cytosines (10 pmol each),dNTPs (each at 1 mmol/L), and 1× buffer [16.6 mmol/L(NH4)2SO4/67 mmol/L Tris/pH 8.8/6.7 mmol/L MgCl2/10 mmol/L β-mercaptoethanol] in a volume of 25 μl.
MSPCR
For each biopsy specimen, 6 PCRs were run (using methylation specific primers, non-methylation specific primers, and housekeeping primers) (although it was not required to use any housekeeping specific primers, it was used just in case that needed further studies).The products of all PCRs (7 μl)were electrophoresed on 2% agarose gels and visualized under UV illumination after staining with ethidium bromide.
The results were reported as positive or negative forp16andRARBmethylation.To confirm the positive results, the procedure was repeated one more time.
Statistical Analysis
To find out any correlation betweenp16andRARBmethylation and prognosis of prostate cancer, Chi-square (χ2)and Fisher exact tests were used to examine the results by SPSS software (version 11.5).P<0.05 was considered significant.
The whole study protocol was approved by the Ethic committee of Shahid Beheshty University of Medical Sciences.
RESULTS
We investigated the methylation profile of 63 subjects in three groups of controls (BPH), good and poor prognosis prostatic cancer, each consisted of 21 individuals.Data are provided in Tables 1 and 2.
The mean age was 61.5±5.5 in control group, 64.3±5.5 and 61.2±8.4 in good and poor prognosis groups respectively,without any significant difference.The mean PSA value was 6.14±2.48 and 17.77±9.46 in good and poor prognosis groups,respectively.
Table 3 showsRARBhypermethylation distribution and the two by two comparisons between the control, good, and poor prognosis groups.There was noRARBmethylation positive subject in control group.In good prognosis group 33.3% were positive forRARBmethylation, which was significant in comparison with control group (P<0.004).Fifteen (71.4%) of poor prognosis group were positive forRARBmethylation that was significantly higher than the good prognosis patients (P<0.013).Compared with patients with good prognostic factors, those with poor prognostic factors were 5 times more likely to haveRARBmethylation[odds ratio (OR)=5; 95% confidence interval (95% CI):1.34-18.55].

Table 1.Clinical data of individuals in good prognosis group
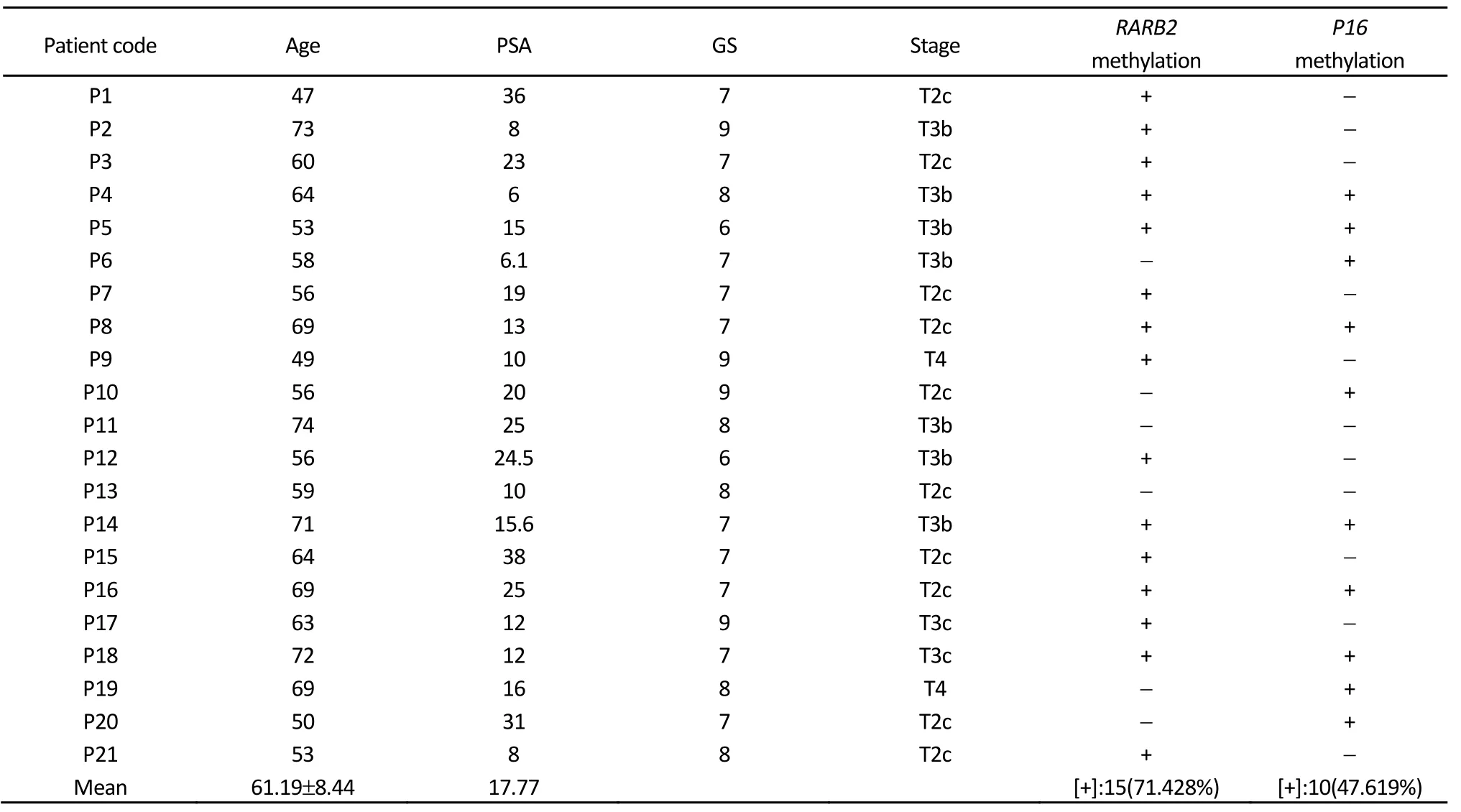
Table 2.Clinical data of individuals in poor prognosis group

Table 3.The comparison of RARB methylation status between each two of study groups
Thep16hypermethylation distribution of the three groups and the comparison are shown in Table 4.There was nop16methylated subject in controls.Four patients in good prognosis group (19.04%) hadp16methylation that was significantly higher than controls (P<0.035).From patients with poor prognosis prostate cancer, ten (47.6%) had methylatedp16 that was significant in comparison with controls (P<0.001).

Table 4.The comparison of p16 methylation status between each two of study groups
Patients with poor prognostic factors were more likely to have methylatedp16compared with patients with good prognostic factor.However the OR (equal to 3.8 with 95% CI of 0.967-15.44) has a trend to be significant.
Bothp16andRARBwere methylated in six patients with poor prognostic features and just for one patient in good prognosis group (P<0.002).Individuals in poor prognosis group in comparison to those in good prognosis group were 33 times more likely to have bothRARBandp16hypermethylation (OR=33; 95% CI: 2.45-443.59).
DISCUSSION
Although the clinical and pathologic indices such as PSA values, grade and stage of the tumor predict the prognosis of the disease, they are products of gross cellular and tissue malfunction; therefore they will become measurable lately in the process of tumor development.[8-10].Finding prognostic factors in molecular and epigenetic level to predict the tumor behavior will probably help us to identify those patients who need more invasive approaches at earlier stage to save more lives[6,12-15,31].
At the time of diagnosis, prostate cancer cells contain many somatic mutations, gene deletions, gene amplifications,chromosomal rearrangements and changes in DNA methylation.These alterations probably accumulate over a period of several decades.Prostate cancer is associated with the greatest heritable risk of any human cancer and the molecular genetics underlying this disease displays a great deal of heterogeneity both between individuals as well as within an affected organ and sometimes between races.The diversity of currently identified somatic genetic abnormalities associated with prostate cancer suggests that there is not a single dominant molecular pathway required for prostate carcinogenesis.Prostate cancer development and metastasis are multistep processes that, among others, involve the inactivation of tumor suppressor genes.Aberrant DNA methylation of CpG (cytosine preceding guanosine) sites is among the earliest and most frequent alterations in cancer.CpG dinucleotides can be found in clusters called CpG islands often in promoter regions.CpG islands of many genes, including tumor suppressor genes, are unmethylated in normal tissues but are methylated to a varying degree in multiple types of cancer, causing silencing of gene transcription and inactivation.
Several studies have indicated that hypermethylation of one or several specific genes or the overall number of hypermethylation events might be useful to classify urothelial carcinomas.Specifically, hypermethylation has been reported to increase with grade, stage and histological subtype, to differ at different locations, and to yield prognostic information additional to that provided by histopathological parameters[32-36].
The use of DNA methylated genes as diagnostic biomarkers has potential application for distinguishing between normal and prostate cancer tissues and for identifying premalignant state.An ideal biomarker would have low levels of methylation in the normal tissue and be highly elevated in the cancer and premalignant state.Previous studies revealed that promoter hypermethylation ofp16andRARb2was strongly correlated with the lack of protein expression, indicating promoter hypermethylation as the main inactivation mechanism of these genes in prostate carcinoma[22-28,37].Furthermore, it has been shown that the number of hypermethylated genes increases as prostate cancer progresses; thus, the investigation of several genes may provide additional diagnostic information[6,12-15,29].
To our knowledge this is the first study on Iranian population investigating some epigenetic factors in prostate cancer.The association ofp16andRARBgenes methylation with prostate cancer has been already examined in a number of studies[22-28,37].
In patients with good prognosis, 33.3% hadRARBgenes hypermethylation, and it was present in 71.4% of cases with poor prognosis.This was comparable with previous studies.Nakayama, et al.investigatingRARBmethylation in Japanese patients detected methylation in 79% of primary prostate cancers, 90% of hormone-refractory prostate cancers and 50%of prostate cancer cell lines, but not in any normal prostate samples[27].Furthermore, in a study by Bastian, et al.on German patients, promoter methylation ofRARBwas present in 71% of prostate cancer patients but rarely or not in BPH[28].
While 19% of our patients with good prognosis hadp16gene hypermethylation, in cases with poor prognosis, 47.6%were hypermethylated.Our patients with poor prognosis prostate cancer were several times more likely to be positive forp16promoter methylation compared with control group.Promoter methylation ofRARBandp16genes was previously reported to be associated with clinicopathologic parameters of prostate cancer progression.
We also investigated whether hypermethylation in prostate cancer is of any prognostic value.Although there is quite a few studies on prognosis evaluation, and the prior studies did not use a common prognosis definition of PSA,tumor stage, or tumor grade, our results are compatible with the preceding studies[6,14,15,25,29].Most studies concur that the frequency of hypermethylated genes increases gradually with stage and grade in prostate carcinoma.Our study showed that hypermethylation of bothRARBandp16genes could be used as a prognostic factor in prostate cancer patients.This could mean that low stage and low grade tumors with multiple hypermethylated genes need to be regarded as high-risk cases.However, more studies are needed to have a better understanding of the molecular mechanisms of the prostate cancer to develop more effective prognostic and therapeutic approaches.
Acknowledgment
We would like to express our sincere gratitude to Sanofi-Aventis for the study support.
1.Jemal A, Siegel R, Ward E, et al.Cancer statistics, 2009.CA Cancer J Clin 2009; 59:225-49.
2.Parkin DM, Bray F, Ferlay J, et al.Global cancer statistics, 2002.CA Cancer J Clin 2005; 55:74-108.
3.Perry AS, Foley R, Woodson K, et al.The emerging roles of DNA methylation in the clinical management of prostate cancer.Endocr Relat Cancer 2006; 13:357-77.
4.Hughes C, Murphy A, Martin C, et al.Molecular pathology of prostate cancer.J Clin Pathol 2005; 58:673-84.
5.Hoque MO.DNA methylation changes in prostate cancer: current developments and future clinical implementation.Expert Rev Mol Diagn 2009; 9:243-57.
6.Cho NY, Kim JH, Moon KC, et al.Genomic hypomethylation and CpG island hypermethylation in prostatic intraepithelial neoplasm.Virchows Arch 2009; 454:17-23.
7.Richiardi L, Fiano V, Vizzini L, et al.Promoter methylation in APC,RUNX3, and GSTP1 and mortality in prostate cancer patients.J Clin Oncol 2009; 27:3161-8.
8.Blute ML, Bergstralh EJ, Iocca A, et al.Use of Gleason score, prostate specific antigen, seminal vesicle and margin status to predict biochemical failure after radical prostatectomy.J Urol 2001; 165:119-25.
9.Roberts WW, Bergstralh EJ, Blute ML, et al.Contemporary identification of patients at high risk of early prostate cancer recurrence after radical retropubic prostatectomy.Urology 2001;57:1033-7.
10.Partin AW, Kattan MW, Subong EN, et al.Combination of prostate-specific antigen, clinical stage, and Gleason score to predict pathological stage of localized prostate cancer.A multi-institutional update.JAMA 1997; 277:1445-51.
11.Scher WI.Cancer of the Prostate.In DeVita VT Jr, Hellman S,Rosenberg SA (eds): Cancer: Principles and Practice of Oncology, 7th ed.Philadelphia, Pa: Lippincott Williams &Wilkins: 2005; 1192-50.
12.Murphy TM, Perry AS, Lawler M.The emergence of DNA methylation as a key modulator of aberrant cell death in prostate cancer.Endocr Relat Cancer 2008; 15:11-25.
13.Jerónimo C, Henrique R, Sidransky D.Uses of DNA methylation in cancer diagnosis and risk assessment.In: Esteller M, editor.DNA methylation.Approaches, methods and applications.CRC Press: Boca Raton 2004; 11-26.
14.Costa VL, Henrique R, Jerónimo C.Epigenetic markers for molecular detection of prostate cancer.Dis Markers 2007; 23:31-41.
15.Zhou SG, Sun YH, Gao JP.DNA methylation and prostate cancer.Zhonghua Nan Ke Xue 2007; 13:1108-12.
16.Kang GH, Lee S, Lee HJ, et al.Aberrant CpG island hypermethylation of multiple genes in prostate cancer and prostatic intraepithelial neoplasia.J Pathol 2004; 202:233-40.
17.Nakayama M, Gonzalgo ML, Yegnasubramanian S, et al.GSTP1 CpG island hypermethylation as a molecular biomarker for prostate cancer.J Cell Biochem 2004; 91:540-52.
18.Bastian PJ, Palapattu GS, Lin X, et al.Preoperative serum DNA GSTP1 CpG island hypermethylation and the risk of early prostate-specific antigen recurrence following radical prostatectomy.Clin Cancer Res 2005; 11: 4037-43.
19.Enokida H, Shiina H, Urakami S, et al.Ethnic group-related differences in CpG hypermethylation of the GSTP1 gene promoter among African-American, Caucasian and Asian patients with prostate cancer.Int J Cancer 2005; 116:174-81.
20.Maruyama R, Toyooka S, Toyooka KO, et al.Aberrant promoter methylation profile of prostate cancers and its relationship to clinicopathological features.Clin Cancer Res 2002; 8:514-9.
21.Bastian PJ, Ellinger J, Wellmann A, et al.Diagnostic and prognostic information in prostate cancer with the help of a small set of hypermethylated gene loci.Clin Cancer Res 2005; 11:4097-106.
22.Woodson K, Hayes R, Wideroff L, et al.Hypermethylation of GSTP1,CD44, and E-cadherin genes in prostate cancer among US Blacks and Whites.Prostate 2003; 55:199-205.
23.Zhang J, Liu L, Pfeifer GP.Methylation of the retinoid response gene TIG1 in prostate cancer correlates with methylation of the retinoic acid receptor beta gene.Oncogene 2004; 23: 2241-9.
24.Yao Q, He XS, Zhang JM, et al.Promotor hypermethylation of E-cadherin, p16 and estrogen receptor in prostate carcinoma.Zhonghua Nan Ke Xue 2006; 12:28-31.
25.Herman JG, Merlo A, Mao L, et al.Inactivation of the CDKN2/p16/MTS1 gene is frequently associated with aberrant DNA methylation in all common human cancers.Cancer Res 1995; 55:4525-30.
26.Jarrard DF, Bova GS, Ewing CM, et al.Deletional, mutational, and methylation analyses of CDKN2 (p16/MTS1) in primary and metastatic prostate cancer.Genes Chromosomes Cancer 1997; 19:90-6.
27.Nakayama T, Watanabe M, Yamanaka M, et al.The role of epigenetic modifications in retinoic acid receptor beta2 gene expression in human prostate cancers.Lab Invest 2001; 81:1049-57.
28.Bastian PJ, Ellinger J, Heukamp LC, et al.Prognostic value of CpG island hypermethylation at PTGS2, RAR-beta, EDNRB, and other gene loci in patients undergoing radical prostatectomy.Eur Urol 2007; 51:665-74.
29.Herman JG, Graff JR, My?h?nen S, et al.Methylation-specific PCR: a novel PCR assay for methylation status of CpG islands.Proc Natl Acad Sci USA 1996; 93:9821-6.
30.Arafa M, Kridelka F, Mathias V, et al.High frequency of RASSF1Aand RARb2gene promoter methylation in morphologically normal endometrium adjacent to endometrioid adenocarcinoma.Histopathology 2008; 53: 525-32.
31.Rosenbaum E, Hoque MO, Cohen Y, et al.Promoter hypermethylation as an independent prognostic factor for relapse in patients with prostate cancer following radical prostatectomy.Clin Cancer Res 2005;11:8321-5.
32.Salem C, Liang G, Tsai YC, et al.Progressive increases in de novo methylation of CpG islands in bladder cancer.Cancer Res 2000;60:2473-6.
33.Maruyama R, Toyooka S, Toyooka KO, et al.Aberrant promoter methylation profile of bladder cancer and its relationship to clinicopathological features.Cancer Res 2001; 61:8659-63.
34.Chan MW, Chan LW, Tang NL, et al.Hypermethylation of multiple genes in tumor tissues and voided urine in urinary bladder cancer patients.Clin Cancer Res 2002; 8:464-70.
35.Tada Y, Wada M, Taguchi K, et al.The association of death associated protein kinase hypermethylation with early recurrence in superficial bladder cancer.Cancer Res 2002; 62:4048-53.
36.Catto JW, Azzouzi AR, Rehman I, et al.Promoter hypermethylation is associated with tumor location, stage, and subsequent progression in transitional cell carcinoma.J Clin Oncol 2005; 23:2903-10.
37.Henrique R, Ribeiro FR, Fonseca D, et al.High promoter methylation levels of APC predict poor prognosis in sextant biopsies from prostate cancer patients.Clin Cancer Res 2007; 13:6122-9.
 Chinese Journal of Cancer Research2011年4期
Chinese Journal of Cancer Research2011年4期
- Chinese Journal of Cancer Research的其它文章
- Expression and Distribution Characteristics of Human Ortholog of Mammalian Enabled (hMena) in Glioma
- Changes of Serum Trace Elements, AFP, CEA, SF, T3, T4 and IGF-Ⅱ in Different Periods of Rat Liver Cancer
- Mast Cells in Adjacent Normal Colon Mucosa rather than Those in Invasive Margin are Related to Progression of Colon Cancer
- Wild-Type KRAS and BRAF Could Predict Response to Cetuximab in Chinese Colorectal Cancer Patients
- Dosimetry Comparison between Volumetric Modulated Arc Therapy with RapidArc and Fixed Field Dynamic IMRT for Local-Regionally Advanced Nasopharyngeal Carcinoma
- Hepatocellular Tumors: Immunohistochemical Analyses for Classification and Prognostication