膀胱癌根治術后復發監測中尿腫瘤標志物聯合檢測組合方式的研究
2012-11-30 07:02:20丁才學
中國當代醫藥 2012年32期
關鍵詞:檢測
丁才學
湖北省公安縣中醫醫院外3科,湖北公安 434300
膀胱癌根治術后復發監測中尿腫瘤標志物聯合檢測組合方式的研究
丁才學
湖北省公安縣中醫醫院外3科,湖北公安 434300
目的 探討膀胱癌根治術后復發監測中尿腫瘤標志物聯合檢測的最佳組合方式。方法 對40例膀胱癌根治術患者于術后復發監測中進行尿纖維連接蛋白(FN)、核基質蛋白22(NMP-22)、膀胱腫瘤抗原(BTA)、纖維蛋白降解產物(FDP)、透明質酸酶(HA)等5項腫瘤標志物檢測,然后按二聯、三聯組合方式計算其不同組合方式檢測的靈敏度、特異度和準確度,并進行比較。 結果 (1)聯合檢測時其靈敏度均較單項檢測時提高,差異均有統計學意義,均P<0.05;聯合檢測時其特異度降低,但差異均無統計學意義,均P>0.05;聯合檢測時其準確率均有所提高,但差異均無統計學意義,均P>0.05。(2)二聯組合方式中以FN+NMP-22組合靈敏度最高,其次為FN+BTA、NMP-22+BTA組合,與其他組合比較差異有統計學意義,均P<0.05。各種二聯組合之間的特異度、準確率的差異均無統計學意義,均P>0.05。(3)三聯組合方式中以FN+NMP-22+BTA組合靈敏度最高,與其他組合比較差異有統計學意義,均P<0.05;各種三聯組合之間的特異度、準確率的差異均無統計學意義,均P>0.05。 結論 尿腫瘤標志物聯合檢測可望部分替代膀胱鏡檢查用于膀胱癌根治術后復發監測,而且在決定尿腫瘤標志物聯合檢測的組合方式時應盡量選擇FN及NMP-22。
膀胱癌;復發;腫瘤標志物;尿液;聯合檢測;組合
膀胱癌根治術后復發監測目前仍以膀胱鏡及活組織檢查為金標準,但此項檢查的明顯不適使患者難以接受,因此需要研究一種無創的非侵入性,且敏感度、特異度及準確率均較高的監測方法。選擇2~3種尿腫瘤標志物 (urinary tumor markers,uTM)聯合檢測便是較為有效的監測方法[1],本研究旨在探討膀胱癌根治術后復發監測中尿uTM聯合檢測的最佳組合方式。
1 資料與方法
1.1 一般資料
選擇2007年1月~2009年6月在本院手術并進行術后隨訪的膀胱癌根治術患者為研究對象。納入標準:(1)接受膀胱癌根治術后;(2)經術后病理學活檢確診為膀胱癌;(3)能按時進行術后隨訪,且隨訪≥3年。排除標準:合并有腎盂癌、輸尿管癌等其他尿路上皮惡性腫瘤。40例患者符合納入標準,其中,男27例,女13例,年齡31~75歲,平均49歲。
1.2 實驗設計
采用同步盲法比較研究。
1.3 方法
1.3.1 復發監測 上述研究對象于膀胱癌根治術后均在術后1個月進行第一次隨訪,以后每3個月隨訪一次,除體檢、必要的特殊檢查外,同時檢測尿纖維連接蛋白(fibronectin,FN)、核基質蛋白 22(nuclear matrix protein-22,NMP-22)、膀胱腫瘤抗原(bladder tumor antigen,BTA)、纖維蛋白降解產物(fibrin degradation products,FDP) 與 透 明 質 酸 酶(hyaluronidase,HA)等5項腫瘤標志物。復發確診以膀胱鏡及病理學活組織檢查為金標準。
1.3.2 TM檢測 收集受試者清潔中段晨尿50 mL,混勻后分為5份(分別檢測上述5項uTM),置-20℃保存備用。FN應用膠體金免疫層析法進行檢測,所用BN-Q2000金標免疫層析分析儀及UFn檢測試劑盒均由上海柏納生物技術有限公司提供。其余各uTM均應用ELISA法進行檢測,酶標比色儀和檢測試劑盒均由上海藍源生物科技有限公司提供。FN、NMP-22、BTA、FDP、HA 的陽性界定值依次分別為>250 μg/L、>10 kU/L、>12 μg/L、>0.25 mg/L、>144.7 μg/L。
1.3.3 研究指標 以膀胱鏡檢查及病理學活檢為金標準判定FN、NMP-22、BTA、FDP、HA。 檢測結果的陽性、陰性,分別計算各項uTM檢測的靈敏度、特異度、準確率;按二聯、三聯方式進行組合分析,凡其中一項陽性即認為聯合檢測陽性,二聯、三聯組合中均為陰性才認為聯合檢測陰性。分別計算不同組合方式檢測的靈敏度、特異度和準確度并進行比較。
1.4 統計學處理
統計學分析應用SPSS 13.0統計學軟件進行數據處理。靈敏度、特異度、準確率的比較采用χ2檢驗。設檢驗水準α=0.05。
2 結果
2.1 受試者數量分析
40例患者均完成3年隨訪,無脫落。其中18例被確診復發。
2.2 各uTM單項檢測及不同組合方式檢測的靈敏度、特異度、準確率
(1)聯合檢測時其靈敏度均較單項檢測時提高,差異均有統計學意義,均P<0.05;聯合檢測時其特異度降低,但其與單項檢測的差異均無統計學意義,均P>0.05;聯合檢測時其準確率均有所提高,但其與單項檢測的差異均無統計學意義,均P>0.05。(2)二聯組合方式中以FN+NMP-22組合的靈敏度、特異度、準確率最高,其次為 FN+BTA、NMP-22+BTA組合,與其他組合比較差異有統計學意義,均P<0.05。(3)三聯組合方式中以FN+NMP-22+BTA組合的靈敏度、特異度、準確率最高,與其他組合比較其差異有統計學意義,均P<0.05。 詳見表 1~3。
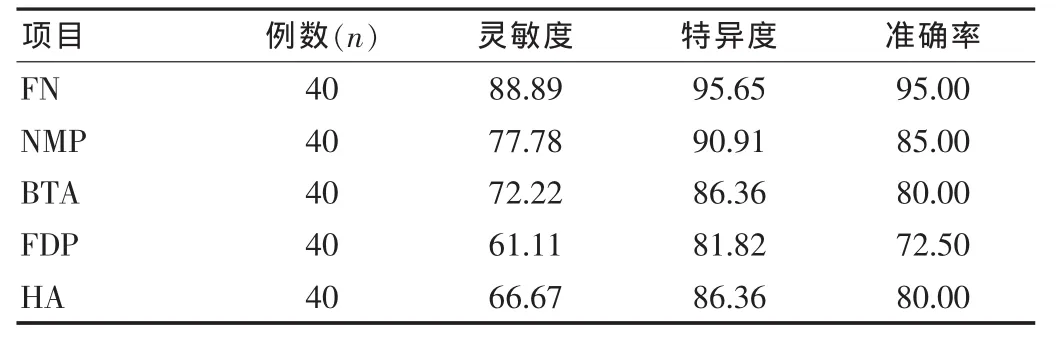
表1 單項uTM檢測的靈敏度、特異度及準確率(%)

表2 兩項uTM聯合檢測的靈敏度、特異度及準確率(%)

表3 三項uTM聯合檢測的靈敏度、特異度及準確率(%)
3 討論
為及時發現和盡早治療膀胱癌根治術后復發,必須進行術后隨訪監測,而理想的監測方法應該具有較高的靈敏度、特異度及準確率,目前只有膀胱鏡檢查符合要求。但膀胱鏡檢查作為一種侵入性手段會給患者尤其是男性患者帶來極大痛苦,還可導致諸如尿路損傷、感染等并發癥,或因前列腺增生、尿道狹窄等原因而無法行膀胱鏡檢查,且膀胱鏡檢查亦有一定的漏診率。所以,探討準確性達到或接近膀胱鏡檢查水平的非侵入性檢查手段對膀胱癌患者進行術后隨訪有著非常重要的意義。
目前多種膀胱癌uTM已廣泛應用于其復發監測,但單項檢測時敏感度、特異度和準確率均不理想,聯合檢測可起到優勢互補的作用。本研究結果顯示,聯合檢測uTM有助于提高對膀胱癌復發預測的敏感度和準確率,且特異度降低的程度不明顯。即在多種uTM中選擇2~3種uTM進行聯合檢測,與金標準比較可以達到較為理想的效果,與文獻[1-8]報告一致。 其中二聯組合中以 FN+NMP-22、FN+BTA、NMP-22+BTA組合較為理想,三聯組合中以FN+NMP-22+BTA組合為好。故筆者認為uTM聯合檢測可望成為膀胱癌根治術術后隨訪的新手段,可以此來部分替代膀胱鏡檢查,而且在決定uTM聯合檢測的組合方式時應盡量選擇FN或NMP-22,再與其他uTM進行組合。
[1]MenendezV,Fernandez Suarez A,Galan JA,et al.Diagnosis of bladder cancer by analysis of urinary fibronectin[J].Urology,2005,65(2):284-289.
[2]Mutul N,Turkerl L,Emerk K.Analytical and clinical evaluation of a new urinary tumor marker:bladder tumor fibronectin in diagnosis and follow up of bladder cancer[J].Clin Chem Lab Med,2003,41(8):1069-1074.
[3]王德林,陳在賢,何梓銘.膀胱腫瘤標記物的研究與應用[J].新醫學,2003,34(12):774-775.
[4]Ho SM,Cheng RY.A promising bladder cancer detection assay the HA HAase test[J].J Urol,2004,172(3):1123-1126.
[5]孫羿,何輝,馬強,等.膀胱腫瘤抗原和透明質酸等七項腫瘤標志物在膀胱腫瘤診斷中的應用價值[J].中華醫學雜志,2005,85(35):2507-2511.
[6]Shariat SF,Casella R,Khoddami SM,et al.Urine detection of survivin is a sensitive marker for the noninvasive diagnosis of bladder cancer[J].J Urol,2004,171:626-630.
[7]王子明,龍清志,種鐵,等.尿NMP22篩檢復發性膀胱癌臨床意義的研究[J].西安交通大學學報(醫學報),2002,23(6):567-594.
[8]李遼源,沈周俊.纖維連接蛋白和膀胱腫瘤[J].國外醫學:泌尿系統分冊,2003,23(6):639-641.
Research of combination of urinary tumor markers in the monitoring of recurrence after radical mastectomy of bladder cancer
DING Caixue
Department of Urology,the Traditional Chinese Medical Hospital of Gong′an County in Hubei Province,Gong′an 434300,China
ObjectiveTo investigate the best combination of urinary tumor markers in the monitoring of recurrence after radical mastectomy of bladder cancer.MethodsForty cases of bladder cancer patients with radical mastectomy were detected by urinary fibronectin(FN),nuclear matrix protein 22(NMP-22),bladder tumor antigen(BTA),fibrin degradation products(FDP)and hyaluronidase(HA).Then press the combination of the two markers and three markers,and to calculate the sensitivity,specificity and accuracy of the different combinations and the difference between each combination were compared.Results(1)The sensitivity of joint detection than the sensitivity of individual detection were increased.The differences had statistically significant,all P<0.05.The specificity of joint detection than the specificity of individual detection were lowered.But the differences had not statistically significant,all P>0.05.The accuracy of joint detection than the accuracy of individual detection were increased.But the differences had not statistically significant,all P>0.05.(2)In the bivalent combinations,the sensitivity of FN+NMP-22 combination was highest,followed by the FN+BTA combination and NMP-22+BTA combination.Compared with the other combinations,the differences had statistically significant,all P<0.05.Between various bivalent combinations,specificity and accuracy showed no significant difference,all P>0.05.(3)In the triple combination,the sensitivity of FN+NMP-22+BTA combination was highest.Compared with the other combinations,the differences had statistically significant,all P<0.05.Between various triple combinations,specificity and accuracy showed no significant difference,all P>0.05.ConclusionJoint detection of urinary tumor markers are expected to partially replace cystoscopy for bladder cancer after radical resection of recurrence monitoring,and try to determine the composition of the joint detection of urinary tumor markers should be FN and NMP-22.
Bladder cancer;Recurrence;Tumor markers;Urine;Joint detection;Combination
R737.14
A
1674-4721(2012)11(b)-0010-03
丁才學(1974-),男,荊州市人,本科學歷,主治醫師;主攻方向:泌尿外科疾病的診療。
2012-07-24 本文編輯:林利利)
猜你喜歡
中國設備工程(2022年12期)2022-07-11 04:33:00
中學生數理化·七年級數學人教版(2021年6期)2021-11-22 07:50:58
中學生數理化·七年級數學人教版(2021年6期)2021-11-22 07:50:58
中學生數理化·七年級數學人教版(2021年6期)2021-11-22 07:50:58
中學生數理化·七年級數學人教版(2020年12期)2021-01-18 06:57:46
中學生數理化·七年級數學人教版(2020年12期)2021-01-18 06:57:46
中學生數理化·七年級數學人教版(2019年9期)2019-11-25 07:34:36
中學生數理化·七年級數學人教版(2019年9期)2019-11-25 07:34:34
中學生數理化·七年級數學人教版(2019年12期)2019-05-21 02:53:50
中學生數理化·七年級數學人教版(2019年12期)2019-05-21 02:53:48
