Results of the parent-rated Strengths and Difficulties Questionnaire in 22,108 primary school students from 8 provinces of China
2013-12-09 02:28:51XinGAOWenhuiSHIYiZHAILiuHEXiaomingSHI
上海精神醫學 2013年6期
關鍵詞:兒童
Xin GAO, Wenhui SHI, Yi ZHAI, Liu HE, Xiaoming SHI*
?Original article?
Results of the parent-rated Strengths and Difficulties Questionnaire in 22,108 primary school students from 8 provinces of China
Xin GAO, Wenhui SHI, Yi ZHAI, Liu HE, Xiaoming SHI*
1. Introduction
Over the past three decades China’s economic boom has been associated with substantial improvements in the physical health of children but the rapid economic development has been associated with increased competitiveness in schools and with massive rural-tourban migration that may have had negative effects on the psychological wellbeing of children. This hypothesized relationship of rapid development and mental health problems in children is supported by the apparent increase in the prevalence of common behavioral and emotional problems among school-age children over recent decades.[1-4]Some of these common psychological problems can be treated relatively easily or even prevented if recognized early, so the development of screening tools that can identify highrisk children is an important part of the effort to protect the psychological wellbeing of the nation’s children and adolescents.
The Strengths and Difficulties Questionnaire (SDQ)is a brief psychopathology screening tool administered to parents or teachers that assesses the emotional symptoms, conduct problems, peer relationships and other psychological characteristics of children and adolescents.[5]It has been extensively evaluated and widely used around the world to screen children for psychopathology.[6-8]Previous studies in China have found that the SDQ has good psychometric properties,[9,10]but there have been no studies that use the SDQ in both urban and rural children or that involve multiple provinces. Moreover, no cutoff scores for identifying high-risk children who merit further clinical evaluation have been established for China.
In the current study, we administered the parentrated version of the SDQ to the parents of a large community sample (n=22,108) of urban and rural primary school students from eight provinces of China,assessed the relationship of the SDQ subscale scores to various demographic factors, and used the results to recommend cutoff scores for identifying high-risk children in China.
2. Method
2.1 Subjects
The data used in this report are from the study entitled:‘Intervention Model for Chronic Diseases among School Children in China.’ This study was funded by the Chinese Center for Disease Control and Prevention Research Foundation and was conducted in 2010 in eight provinces: Inner Mongolia, Jiangsu, Anhui, Shandong,Hunan, Guangxi, Chongqing and Gansu. As shown in Figure 1, a multi-stage cluster sampling method was used. The per capita GDP of all counties and urban districts (i.e., ‘primary sampling units’ [PSUs]) in each of the eight provinces was obtained from the China Statistical Information Network and the provincial Statistical Information Network. The PSUs in each province were evenly divided into three economic strata: high, medium and low per capita GDP. In each of the eight provinces one PSU was randomly selected from each stratum. Then in each selected PSU, one urban primary school and one rural primary school were randomly sampled. Using this method, 24 urban and 24 rural schools were sampled. In each school two or three classes were randomly selected from each of the six grades (i.e., grade 1 to grade 6) to ensure a sample size of at least 80 students from each grade. In one of the selected rural schools, there were less than 80 students in every grade, so classes of the same grades from a nearby school were recruited to achieve the required sample of 80 students. The survey was administered by trained investigators to the legal guardians of all students in selected classes during parent-teacher conferences. (In China, virtually all parents attend these conferences.) A total of 26,737 questionnaires were completed and returned; questionnaires that had multiple un-answered items or in which all the answers were the same (suggesting poor quality) were excluded;this left a final sample of 22,108 (82.7%) successfully completed surveys.
All respondents signed informed consent before the survey. The study was approved by the Institutional Review Board of the Chinese Center for Disease Control and Prevention.

Figure 1. The identification of participants
2.2 Assessments
Basic demographic information collected as part of the survey included the relationship of the respondent with the target child and the target child’s gender and age. The urban versus rural location of the PSU and the economic strata of the PSU (high, medium or low)in which each child’s school was located were also recoded.
The SDQ is a 25-item scale with fi ve subscales that each have 5 items. Each item is rated on a 3-point Likert scale: not true (0), somewhat true (1) and certainly true (2). Thus, the subscale scores range between 0 and 10. Four of the SDQ subscales measure difficulties that the child has, including emotional problems, problems of conduct, hyperactivity or inattention, and peer relationship problems. The total difficulties score is the sum of these four subscale scores ranging from 0 to 40,with higher scores indicating more difficulties. The fifth subscale measures positive (i.e., prosocial) attributes of the individual, such as the willingness to help others and to share. A previous study using the Chinese version of the parent-rated SDQ reported that the internal consistency of the full scale was satisfactory (Cronbach’s α=0.60).[9]Another study in China reported that the correlation between item scores and subscale total scores ranged from 0.32 to 0.77 and that the test-retest correlation of items ranges from 0.43 to 0.79.[10]And the SDQ scores in China correlate with the scores on the Chinese version of the Achenbach’s Child Behavior Checklist (CBCL).[11]
We used the percentile banding method suggested by Goodman[12]to identify cutoff scores for the total difficulty score associated with ‘abnormal’, ‘borderline’and ‘normal’ results. Total parental SDQ scores above the 90thpercentile were classified as abnormal, those in the 80thto 90thpercentile range as ‘borderline’, and those below the 80thpercentile as ‘normal’.
2.3 Statistical analysis
Data were independently double entered using EPI Data 3.0. All statistical analyses were carried out using SPSS software version 17.0. Descriptive statistics were used to describe the demographic variables, SDQ scores and threshold values. The internal consistency of SDQ was assessed using Cronbach’s alpha. Independent sample t-tests were used to compare the SDQ scores by gender(male v. female) and residence (urban v. rural). Pearson correlation coefficients were calculated to measure the correlation between age and SDQ scores. Multivariate linear regression was used to identify factors that were independently associated with the SDQ subscale scores.Results were considered statistically significant when p<0.05.
3. Results
3.1 General information
The demographic characteristics of the sample are shown in Table 1. Among the 22,108 children, 11,863(53.7%) were male and 10,245 (46.3%) were female. A total of 11,431 (51.7%) lived in urban areas and 10,677(48.3%) in rural areas. Their age ranged from 5 to 13 years with a mean (sd) age of 9.3 (1.8) years. Among the informants who completed the survey, 19,749 (89.3%)were parents and 2359 (10.7%) were other relatives.
3.2 Internal consistency
The internal consistency of the SDQ subscales were as follows: emotional symptoms (Cronbach’s α=0.57),conduct problems (Cronbach’s α=0.50), hyperactivity/inattention (Cronbach’s α=0.62), peer relationship problems (Cronbach’s α=0.22), and prosocial behaviors(Cronbach’s α=0.65). Cronbach’s α for the total difficulties scale (i.e. the sum of the fi rst four subscale scores) was 0.69 and Cronbach’s α for all 25 items (using reverse coding for the prosocial behavior items) was 0.73.
3.3 Distribution of the SDQ scores in Chinese students
The male-female differences of SDQ scores stratifying by age are shown in Table 2. There were no statisticallysignificant differences between any of the subscale scores at age 5 and only one significant difference existed at age 13 (higher hyperactivity/inattention in boys). In the intervening years of 6 through 12, girls had more prosocial behaviors while boys had higher scores on the hyperactivity/inattention subscale, the conduct problems subscale and on the total difficulties score.

Table 1. Characteristics of the 22,108 surveyed primary school students and their informants from 8 provinces in China
The correlation between age and SDQ scores is shown in Table 3, and the mean scores of each SDQ subscale by age for boys and girls are shown in Figures 2 and 3. In both boys and girls hyperactivity/inattention decreased with age, while peer relationship problems became more common with increasing age. There was also an increase in reports of emotional problems with age in girls and, to a lesser extent, in boys.
The rural-urban comparison of SDQ scores stratified by gender are shown in Table 4. As reported by their guardians, compared to urban children rural children(both boys and girls) had more emotional symptoms,more conduct problems, more peer relationship troubles and less prosocial behaviors. The total difficulty scores were significantly higher among children from rural areas (t=13.66 p<0.001). On the other hand,boys who lived in urban areas tended to have more hyperactivity/inattention symptoms compared to boys from rural areas, but this was not the case for urban girls versus rural girls.
As shown in Table 5, these urban-rural differences remained statistically significant for all SDQ subscales even after adjusting for gender, age, type of informant(parent v. other relative) and economic strata of the community within the province (high, medium or low per capita GDP). Interestingly, the economic strata of the community also had a significant association with all SDQ subscale scores even after adjusting for the rural versus urban variable: compared to children from high-income counties or urban districts, students from medium- or low-income communities had higher levels of emotional symptoms, more conduct problems, more peer relationship problems, less prosocial behavior and
lower levels of hyperactivity/inactivity. One unexpected finding was that children for whom a non-parent guardian (usually a grandparent or other relative)completed the survey had significantly more difficulties and significantly less prosocial behavior that children for whom a parent completed the survey.

Table 2. Scores on the parent-rated Strengths and Difficulties Questionnaire (SDQ) of 22,108 primary school children from 8 provinces in China
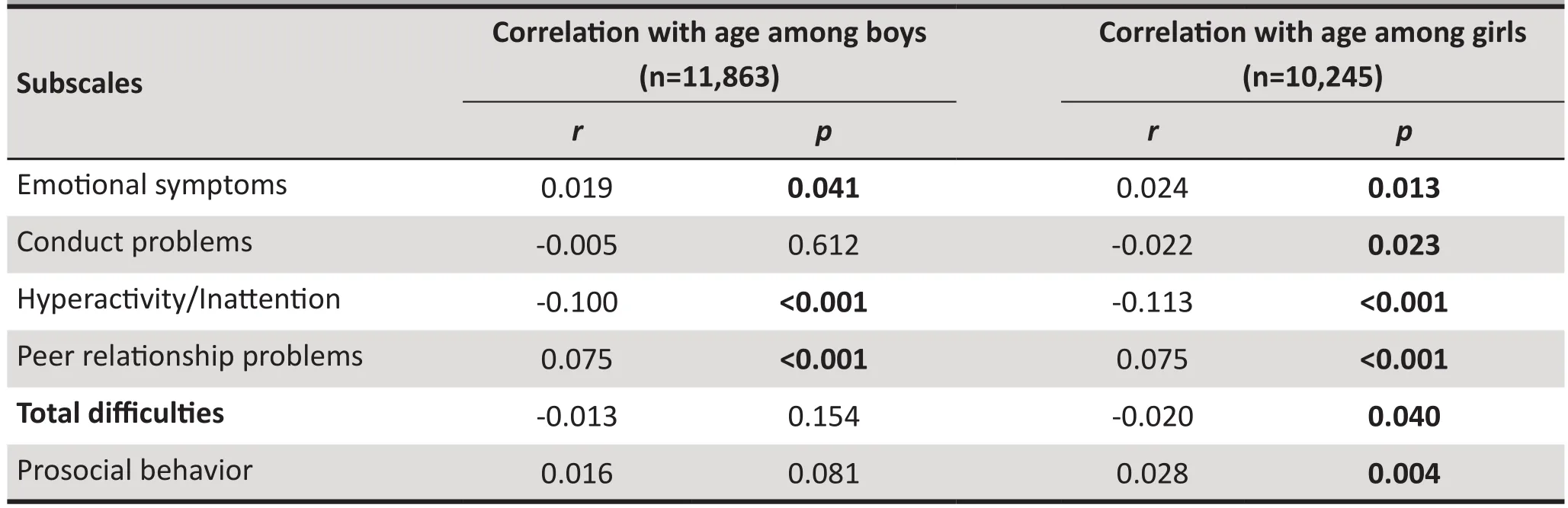
Table 3. Correlation of age with scores on the parent-rated Strengths and Difficulties Questionnaire (SDQ)for male and female schoolchildren from 8 provinces in China

Figure 3. Parent-rated Strengths and Difficulties Questionnaire (SDQ) scores by age among girls

Table 4. Urban-rural comparison of the subscale scores of the parent-rated Strengths and Difficulties Questionnaire (SDQ) in a random sample of 22,108 children from 8 provinces in China

Table 5. Multiple linear regression of demographic characteristics associated with subscale scores on the parent-rated Strengths and Difficulties Questionnaire (SDQ) among 21,108 children from 8 provinces in China
3.4 Recommended SDQ cutoff scores in China and comparison with cutoff scores used in other countries
The cutoff scores for classifying results as ‘abnormal’,‘borderline’ and ‘normal’ (see methods section for method of doing this), are presented in Table 6 along with the corresponding cutoff scores used in Japan[13]and the United Kingdom.[14]For total difficulties,hyperactivity/inattention and peer relationship problems, the cutoff scores for borderline and abnormal ranges in China were higher than those in Japan and the United Kingdom. For prosocial behavior, the cutoffscores were lower in China compared to those in Japan and the United Kingdom. For conduct problems, the cutoff scores in China and the United Kingdom were similar, but both of these scores were higher than those employed in Japan. For the emotional symptoms subscale, all three countries used similar cutoff scores.
4. Discussions
4.1 Main Findings
Parents and guardians of 6 to 12 year-old boys reported more hyperactivity/inattention issues, more conduct problems, higher total difficulties scores and less prosocial behaviors than parents of girls. Parental reports of the prevalence of emotional symptoms were similar in boys and girls at most ages, but girls 8 years old had more emotional symptoms than boys at the same age. We also found that among children 5 to 13 years old scores of hyperactivity/inattention decreased with age, but scores of emotional symptoms increased with age. These findings are similar those reported previously in China and elsewhere,[15,16]and fit with current understanding of the psychological development and socialization of primary school aged children.
We found that psychological and behavioral problems reported by guardians were significantly more severe among children from rural areas than among children from urban areas. Children living in rural communities had more emotional symptoms, more conduct problems, more peer interaction problems, higher total difficulties scores and less prosocial behaviors. These differences might be due to socio-economic factors such as lower family income, lower parental level of education and parental unemployment.[15]Another factor that may be related to this result is that in rural China a large number of children are ‘left behind’when their parents migrate to cities for work. In a survey conducted in rural Hunan province using SDQ to compare ‘left behind’ children and children living with their parents, ‘left behind’ children had significantly higher total difficulty scores and significantly lower prosocial behavior scores.[17]In our study, even though we cannot be certain that all the children withoutparents as informants were not living with their parents,the fact that there were more psychological problems in children who did not have parents come to the parent-teacher meetings echoes previous findings and highlights the need to pay increased attention to the psychological health of these ‘left-behind’ children.

Table 6. Comparison of cutoff scores of the parent-rated Strengths and Difficulties Questionnaire(SDQ) among primary school age children from Chinaa, Japanb and the United Kingdomc
However, another possible explanation for these urban-rural differences is that rural respondents are less sensitive to the stigmatizing effect of reporting emotional and behavioral problems in their children than urban residents. If that is the case, their report of more prevalent problems may not reflect true differences in the behavior of rural versus urban children. Similarly,the more common reports of hyperactivity/inattention problems in urban versus rural boys may reflect different levels of awareness about the importance of this as a‘problem’ between urban versus rural communities;it does not necessarily mean that there are significant differences in the prevalence of these problems. Future studies are needed to explore the reasons for these observed urban-rural differences.
Using the percentile method of categorizing results as ‘abnormal’, ‘borderline’ and ‘normal’ as described by Goodman,[12]we found that the cutoff scores in Chinese children were different from those reported for Japan and the United Kingdom.[13,14]The cutoff scores we recommend in China for total difficulties, hyperactivity/inattention, peer relationship problems and conduct problems among Chinese children were higher than those used in Japan and the United Kingdom, but the cutoff scores for emotional symptoms and prosocial behaviors were lower. These results suggest that difficulties in attention, discipline and peer interaction were more common among children in China while prosocial behaviors such as helping, sharing and caring were less common in Chinese children. There are several possible explanations for these differences.(a) Our sample included a higher proportion of boys(53.7% versus 50.5% in the Japan study and 50.0% in the United Kingdom study). Boys tend to have higher difficulty scores and lower prosocial behavior scores so this could have resulted in greater difficulties and less prosocial behaviors in the Chinese sample. (b) Our fi nding of a higher prevalence of psychological problems in children from rural areas and from economically deprived communities suggests that the lower level of urbanization and economic development in China compared to that in Japan and the United Kingdom may be a factor in the higher levels of reported psychological problems in children in China. (c) Cross-cultural differences in parental expectation may also be a factor. In collectivistic cultures like China and Japan, children are usually encouraged to be modest and disciplined, while in individualistic cultures children are encouraged to be independent and self-confident. Parents in China and Japan may have more demanding standards when assessing the psychological and behavioral performance of their children and, thus, tend to report more difficulties instead of strengths. Similarly, the Japanese culture highly emphasizes politeness, obedience and collectivism; this may contribute to the lower cutoff scores in Japan compared to China on hyperactivity/inattention and peer relationship problem subscales.Future studies are needed to understand these crosscultural differences.
4.2 Limitations
The current study has the following limitations. (a) Data from 17.3% of the surveyed participants were excluded because of missing data or indications of compromised quality (e.g. same answers to all questions). It is possible that these children have different profiles than those in which the guardians appropriately completed the survey. Some evidence suggests that children from families in which parents are less capable of completing the questionnaires might be at a higher risk of psychological and behavioral problems.[15](b) Only a parent-rated SDQ was used in this study; other studies have combined parental ratings with those of teachers and, occasionally, older siblings.[18]We were, therefore,unable to compare the categorization based on parental SDQ scores to those of other informants. (c) No ‘gold standard’ diagnostic assessment was conducted so it is not possible to determine the sensitivity and specificity of the proposed cut off score – which is based on the arbitrary decision that 10% of children are ‘abnormal’ –for identifying mental disorders. (d) The questionnaires were filled out by the guardians of the children who attended the parent-teacher conferences. It is possible that the person who filled out the questionnaire did not know the child very well; if this was the case it would undermine the validity of the assessment.(e) The internal consistency of the peer relationship subscale was very low (alpha=0.22). This suggests that this subscale score is a sub-optimal measure for peer relationship in China and that more work will be needed to revise this subscale for use in China. (f) We did not conduct test-retest assessments of SDQ in this study so the stability of the measures over time is unknown.(g) Despite being the largest such study using SDQ yet conducted in China, the sample was not nationally representative so there may be unknown biases in the study. (h) Finally, the very large sample was one of the strengths of the study, but with such a large study very small differences in mean scores between groups can easily achieve statistical significance. Thus some of the differences identified between groups,though statistically significant, may not be of practical importance.
4.3 Significance
This study identified a stratified random sample of over 20,000 schoolchildren 5 to 13 years of age in 8 provinces of China – a sampling frame that covered more than 30 percent of all children in this age group in the country.Though not nationally representative, it is the largest such study conducted in China to date so it provides a detailed overview of the types of psychological problems experienced by children attending primary school. This information is essential for developing teacher-training programs about children’s psychological problems, for planning screening campaigns for mental disorders, and for developing treatment services for children with mental disorders. For example, this study indicates that screening for hyperactivity/inattention problems in boys should start before the age of 10 and coaching in developing and maintaining good peer relationships should start in the early teen years. If the rural-urban differences identified in the study are confirmed in more detailed studies, there will be a clear need to develop intervention strategies to enhance rural children’s mental health. Further work is also needed to determine whether or not the cutoff scores identified for the Chinese version of the SDQ actually identify a high-risk group of children that are in need of clinical services. If the SDQ proves to have good sensitivity and specificity for identifying children who meet formal diagnostic criteria of mental disorders, mechanisms for providing these services in ways that will be acceptable both to the parents and to the children will need to be developed and tested.
Conflict of interest
The authors declare no conflict of interest related to this article.
Acknowledgements
The authors would like to thank the Centers of Disease Control and Prevention of Inner Mongolia, Jiangsu,Anhui, Shandong, Hunan, Guangxi, Chongqing and Gansu for their on-site work and support.
Funding
The study was funded by Chinese Center for Disease Control and Prevention Youth Funding (2010A205).
1. Li HT, Ye RW, Ren AG, Gao JJ, Zhang T, Liu JM. Behavioral problems of children aged 4-6 years in 26 cities and counties in China. Chinese Mental Health Journal 2009;23(6): 415-420. (in Chinese)
2. Yang BX, Cheng ZH, Yuan GZ. The research progress of mental health epidemiology in primary and secondary school students. Journal of International Psychiatry 2004;31(3): 184-186. (in Chinese)
3. Wang YF, Gu BM, Zhang AL. An epidemiological study on behavioral problems in 2432 school-children in an urban area in Beijing. Chinese Mental Health Journal 1988;2(3):114-117. (in Chinese)
4. Wang YF, Gu BM. Children behavioral problems in urban area of Beijing: a comparison between 1985 and 1993. Chinese Mental Health Journal 2000;14(1): 51-53. (in Chinese)
5. Youthinmind [internet]. [cited 2013 Dec 5]. Information for researchers and professionals about the strengths and difficulties questionnaire. Available from: http://sdqinfo.com/
6. Stone LL, Otten R, Engels RC, Vermulst AA, Janssens JM.Psychometric properties of the parent and teacher versions of the strengths and difficulties questionnaire for 4- to 12-year-olds: a review. Clin Child Fam Psychol Rev 2010;13(3): 254-274.
7. Goodman R. Psychometric properties of the strengths and difficulties questionnaire. J Am Acad Child Adolesc Psychiatry 2001;40(11): 1337-45.
8. Mieloo C, Raat H, van Oort F, Bevaart F, Vogel I, Donker M,et al. Validity and reliability of the strengths and difficulties questionnaire in 5-6 year olds: differences by gender or by parental education. PLoS One 2012;7(5): e36805.
9. Kou JH, Du YS, Xia LM. Reliability and validity of “children strengths and difficulties questionnaire” in Shanghai norm.Shanghai Archives of Psychiatry 2005;17(1): 25-28. (in Chinese)
10. Liu SJ, Huang Y, Deng XH, Tang X, Xie L, Jin M, et al. The initial factors analysis of the Chinese version of the Strengths and Difficulties Questionnaire. West China Medical Journal 2006;21(2): 295-296. (in Chinese)
11. Kou JH, Du YS. The relationship study between children strengths and difficulties questionnaire and child behavior checklist. Journal of Clinical Psychiatry 2009;19(5): 317-319.(in Chinese)
12. Goodman R. The strengths and difficulties questionnaire: a research note. J Child Psychol Psychiat 1997;38(5): 581-586.
13. Matsuishi T, Nagano M, Araki Y, Tanaka Y, Iwasaki M,Yamashita Y, et al. Scale properties of the Japanese version of the Strengths and Difficulties Questionnaire (SDQ): a study of infant and school children in community samples.Brain Dev 2008;30(6): 410-415.
14. Meltzer H, Gatward R, Goodman R, Ford T. Mental health of children and adolescents in Great Britain. Int Rev Psychiatry 2003;15(1-2): 185-187.
15. Shojaei T, Wazana A, Pitrou I, Kovess V. The strengths and difficulties questionnaire: validation study in French schoolaged children and cross-cultural comparisons. Soc Psychiatry Psychiatr Epidemiol 2009;44(9): 740-747.
16. Huang YR, Yan Q, Li YY, Liu J, Y HQ, Yan Y. Strengths and Difficulties Questionnaire in 737 primary and middle school students aged 6–17 in Changsha. Journal of Central South University (Medical Science) 2012;37(8): 860-864. (in Chinese)
17. Yang XH, Zhu CY, Yang QS, Li ZH, Xie GR. Left-home children’s hope and its relationship with mental health. Chinese Journal of Clinical Psychology 2013;21(3): 505-507. (in Chinese)
18. Goodman R, Ford T, Simmons H, Gatward R, Meltzer H.Using the Strengths and Difficulties Questionnaire (SDQ) to screen for child psychiatric disorders in a community sample.Br J Psych 2000;177: 534-539.
長處與困難問卷(父母版)在中國8個省份22,108名小學生中的調查結果
高欣 石文惠 翟屹 何柳 施小明*
中國疾病預防控制中心 北京
背景: 我國兒童心理問題不斷增多,因此能夠有效評估兒童行為和情緒問題的篩選工具對于促進我國兒童身心健康和預防兒童精神疾病有重要的意義。目的在來源于中國不同地區城市和農村的大樣本兒童中對國際公認的長處和困難問卷(SDQ)中文版的使用進行評估,包括情緒癥狀、品行問題、多動/注意缺陷、同伴交往問題和親社會行為。方法采用分層隨機抽樣選取8省份22,108名小學生(年齡在5歲至13歲)的法定監護人(父母為主)進行SDQ(父母版)中文版問卷調查。本研究評估了SDQ評分與社會人口學特征之間的關聯性,并比較了中國與日本和英國在“異常”, “臨界”和“正常”標準的百分位劃界分。結果SDQ(父母版)5個分量表中有4個內部一致性尚可,但是“同伴關系問題”分量表則較差(alpha =0.22)。監護人反映男孩比女孩的多動/注意力缺陷問題更多,而女孩比男孩的情感癥狀問題突出。男孩和女孩的多動/注意力缺陷問題都會隨著年齡的增長而減少,而同伴交往問題隨著年齡增長而增多。農村地區和監護人不是父母(即祖父母或其他親屬)的孩子中,情緒癥狀、品行問題和同伴交往問題較為普遍。中國兒童中判定為“異常”的90%百分位劃界分(19-40)要高于日本和英國報道的兒童劃界分。討論此項研究提示,對男孩的多動/注意缺陷問題應在10歲之前開始預防,并且在青春期早期就要開始訓練如何減輕與同伴交往帶來的壓力。進一步的研究需要注重于提高SDQ在中國文化背景下的信效度,并確定SDQ對于識別孩子是否需要心理健康服務的敏感性和特異性。
Background:A valid screening tool for behavioral and emotional problems in children and adolescents is needed to promote psychological wellbeing and to prevent mental disorders in China’s children.Aim:Assess the use of the Chinese version of the internationally recognized Strengths and Difficulties Questionnaire (SDQ) – which assesses emotional symptoms, conduct problems, hyperactivity/inattention, peer relationship problems and prosocial behaviors – in a large sample of urban and rural children from different parts of China.Methods:The Chinese version of the parent-reported SDQ was administered to legal guardians (primarily parents) of a stratified random sample of 22,108 primary school children 5 to 13 years of age from eight provinces in China. The association between SDQ scores and socio-demographic characteristics was assessed and the percentile cutoff scores for ‘abnormal’, ‘borderline’ and ‘normal’ results in China were compared with those for Japan and the United Kingdom.Results:The internal consistency of the 4 of the 5 SDQ subscales were satisfactory but that for the ‘peer relationships problems’ subscale was quite poor (alpha=0.22). Guardians reported that boys were more likely than girls to have hyperactivity/inattention problems and that girls were more likely than boys to have problems with emotional symptoms. For both boys and girls hyperactivity/inattention problems decreased with age while peer relationship problems increased with age. Emotional symptoms, conduct problems and peer relationship problems were more common in children from rural areas and in children whose identified guardian was not a parent (i.e., a grandparent or other relative). The 90thpercentile cutoff score for abnormal results was higher in Chinese children than the cutoff scores reported for children in Japan and the United Kingdom.Conclusions:This study suggests that prevention programs for hyperactivity/inattention problems in boys need to start before the age of 10 and that training in methods of reducing the stress associated with peer relationships should start in early adolescence. Further work is needed to improve the cultural validity of the SDQ in China and to determine its sensitivity and specificity for identifying children who are in need of mental health services.
10.3969/j.issn.1002-0829.2013.06.005
Chinese Center for Disease Control and Prevention, Beijing, China
*correspondence: sxmcdc@163.com
(received: 2013-08-19; accepted: 2013-09-29)

Xin Gao attained a bachelor’s degree in 2005 and a master’s degree in mental health in 2008, both from West China School of Medicine, Sichuan University. From 2008 to the present, she has been working as an assistant researcher engaged in mental health facilitation and injury prevention in the department of community chronic diseases at the Chinese Center for Disease Control.
*通訊作者:sxmcdc@163.com
猜你喜歡
少兒美術·書法版(2021年12期)2021-10-24 02:50:16
少兒美術·書法版(2021年9期)2021-10-20 06:35:28
少兒美術·書法版(2021年7期)2021-10-20 06:29:16
少兒美術·書法版(2021年11期)2021-10-20 06:23:28
少兒美術·書法版(2021年10期)2021-10-20 06:14:04
少兒美術·書法版(2021年8期)2021-10-20 06:08:10
少兒美術(2019年8期)2019-12-14 08:07:00
少兒美術(2019年3期)2019-12-14 08:02:56
雜文選刊(2016年7期)2016-08-02 08:39:56
小天使·一年級語數英綜合(2016年6期)2016-05-14 12:21:05
- 上海精神醫學的其它文章
- Introduction to mediation analysis with structural equation modeling
- A case of neuroleptic malignant syndrome induced by perospirone
- Operationalizing the involuntary treatment regulations of China’s new mental health law
- Case-control study of allele frequencies of 15 short tandem repeat loci in males with impulsive violent behavior
- Characteristics of the gastrointestinal microbiome in children with autism spectrum disorder: a systematic review
- Can cognitive dissonance methods developed in the West for combatting the ‘thin ideal’ help slow the rapidly increasing prevalence of eating disorders in non-Western cultures?