小兒肺熱咳喘口服液對小兒毛細支氣管炎Th1/Th2細胞的影響研究
2015-03-23 07:18:12李靜董艷張晶潔潘鴻
實用心腦肺血管病雜志 2015年4期
關鍵詞:小兒
李靜,董艷,張晶潔,潘鴻
·中醫·中西醫結合·
小兒肺熱咳喘口服液對小兒毛細支氣管炎Th1/Th2細胞的影響研究
李靜,董艷,張晶潔,潘鴻
目的探討小兒肺熱咳喘口服液對小兒毛細支氣管炎Th1/Th2細胞的影響。方法選擇2013年9月—2014年12月北京市昌平區中西醫結合醫院兒科收治的毛細支氣管炎住院患兒80例,按隨機數字表法分為試驗組和對照組,各40例。根據臨床用藥指南,兩組患兒均給予抗感染和對癥治療,對照組患兒靜脈滴注頭孢曲松鈉治療,治療組患兒在對照組基礎上給予小兒肺熱咳喘口服液治療,療程均為7 d。比較兩組患兒臨床療效,治療前后干擾素γ (IFN-γ)、白介素4(IL-4)水平及Th1細胞分數、Th2細胞分數、Th1/Th2細胞百分比變化,并觀察治療期間兩組患兒不良反應發生情況。結果試驗組患兒臨床療效優于對照組(P<0.05)。治療前兩組患兒血清IFN-γ、IL-4水平及Th1細胞分數、Th2細胞分數、Th1/Th2細胞百分比比較,差異無統計學意義(P>0.05);治療后試驗組患兒血清IFN-γ、IL-4水平及Th1細胞分數、Th2細胞分數、Th1/Th2細胞百分比低于對照組(P<0.05)。結論小兒肺熱咳喘口服液治療毛細支氣管炎患兒臨床療效良好,可通過調節Th1/Th2細胞而增加患兒免疫功能。
毛細支氣管炎;小兒肺熱咳喘口服液;Th1-Th2平衡
李靜,董艷,張晶潔,等.小兒肺熱咳喘口服液對小兒毛細支氣管炎Th1/Th2細胞的影響研究[J].實用心腦肺血管病雜志,2015,23(4):114-117.[www.syxnf.net]
Li J,Dong Y,Zhang JJ,et al.Impact of xiaoer-feire-kechuan oral solution on Th1/Th2 cells of infants with bronchiolitis[J].Practical Journal of Cardiac Cerebral Pneumal and Vascular Disease,2015,23(4):114-117.
毛細支氣管炎是兒科常見疾病,多發于1歲尤其是6個月以下嬰幼兒,春季為其高發季節[1]。毛細支氣管炎是由呼吸道合胞病毒引起下呼吸道急性炎癥所致的氣道阻塞性疾病[2],近年來,該病在嬰幼兒肺部病毒感染疾病中居首位[3]。其主要臨床表現為呼吸困難、喘息且易反復發作,與一般炎癥不同,患兒常為家族遺傳性過敏體質[4]。臨床研究顯示,毛細
支氣管炎的發病機制與哮喘極相似,且該病病后哮喘發生率高達25%~50%[5]。臨床上治療毛細支氣管炎以抗感染及對癥治療為主,但患兒極易出現胃部不適等不良反應[6]。毛細支氣管炎隸屬中醫“咳嗽”范疇,且臨床多見痰熱壅肺型[7]。小兒肺熱咳喘口服液為中藥合劑,由多種中草藥提煉而成,其中包含了麻杏石甘湯及白虎湯兩劑古方,加之現代經典方劑,具有解毒清熱化痰、宣肺止咳平喘的功效[8-9]。有研究證實,小兒肺熱咳喘口服液具有廣譜抗菌、抗病毒的作用[10]。本研究探討了小兒肺熱咳喘口服液對小兒毛細支氣管炎Th1/Th2細胞的影響,旨在為臨床應用小兒肺熱咳喘口服液治療小兒毛細支氣管炎提供參考。
1 資料與方法
1.1 納入和排除標準納入標準:(1)符合全國小兒呼吸疾病會議制定的相關診斷標準,以憋悶、喘息為主要臨床表現,或伴有發熱,雙肺可聞及喘鳴音或濕啰音;(2)年齡<2歲; (3)首次發病,且無其他急、慢性疾病;(4)病程2~7 d; (5)經患兒家長同意并簽署知情同意書。排除標準:(1)近2周有其他呼吸道炎癥或感染者;(2)合并其他急、慢性疾病者;(3)過敏體質及有免疫系統疾病者;(4)有先天性疾病和其他遺傳疾病者;(5)患兒家長拒絕接受治療者。
1.2 一般資料選擇2013年9月—2014年12月北京市昌平區中西醫結合醫院兒科收治的毛細支氣管炎住院患兒80例,按隨機數字表法分為試驗組和對照組,各40例。兩組患兒性別、月齡、白細胞計數(WBC)及病程比較,差異無統計學意義(P>0.05,見表1),具有可比性。
表1 兩組患兒一般資料比較(±s)Table 1 Comparison of general information between the two groups
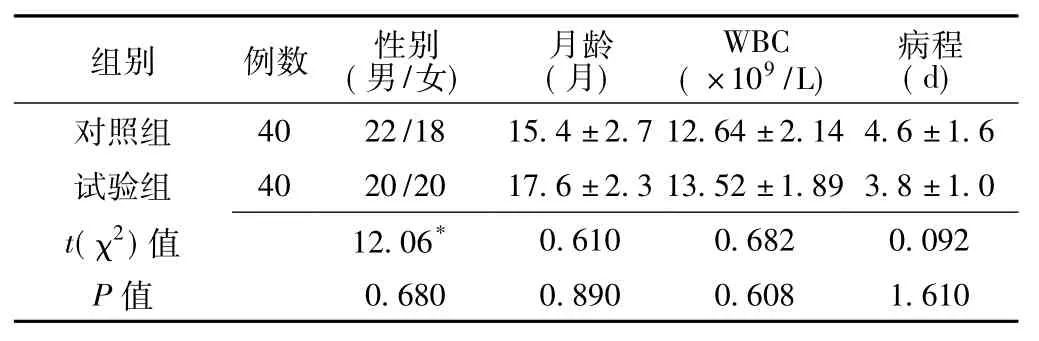
表1 兩組患兒一般資料比較(±s)Table 1 Comparison of general information between the two groups
注:WBC=白細胞計數,*為χ2值
組別例數性別(男/女)月齡(月) WBC (×109/L)病程(d) 40 22/18 15.4±2.7 12.64±2.14 4.6±1.6試驗組40 20/20 17.6±2.3 13.52±1.89 3.8±1.0 t(χ2)值對照組0.680 0.890 0.608 1.610 0.610 0.682 0.092 P值12.06*
1.3 治療方法根據臨床用藥指南,兩組患兒均給予抗感染和對癥治療,對照組患兒靜脈滴注頭孢曲松鈉50~80 mg/kg,1次/d。治療組患兒在對照組基礎上給予小兒肺熱咳喘口服液,具體用法:1歲以下患兒5 ml/次,2次/d;1~3歲患兒10 ml/次,3次/d。療程均為7 d,且治療期間注意患兒飲食及觀察患兒臨床癥狀、體征變化。
1.4 觀察指標治療后判定兩組患兒臨床療效,比較兩組患兒治療前后干擾素γ(IFN-γ)、白介素4(IL-4)水平及Th1細胞分數、Th2細胞分數、Th1/Th2細胞百分比變化,并觀察治療期間兩組患兒不良反應發生情況。
1.4.1 血清IFN-γ、IL-4水平檢測清晨空腹采集靜脈血3 ml,1 200 r/min離心,離心半徑為3 cm,分離血清,待檢。采用雙抗體夾心酶聯免疫吸附試驗(ELISA)法測定血清IFN -γ和IL-4水平,操作步驟嚴格按照試劑盒說明書進行操作。
1.4.2 Th1/和Th2細胞檢測取患者外周靜脈血3 m l,采用FACSCalibur流式細胞儀檢測Th1細胞分數、Th2細胞分數,計算Th1/Th2細胞百分比。
1.5 臨床療效判定標準顯效:咳嗽、喘息及肺部啰音等臨床癥狀顯著改善;有效:咳嗽、喘息及肺部啰音等臨床癥狀好轉,體溫恢復正常;無效:咳嗽、喘息及肺部啰音等臨床癥狀未見好轉或出現加重,其他臨床癥狀未見改善。
1.6 統計學方法采用SPSS 19.0統計學軟件進行數據處理,計量資料以(±s)表示,采用兩獨立樣本t檢驗;計數資料采用χ2檢驗;等級資料采用秩和檢驗。以P<0.05為差異有統計學意義。
2 結果
2.1 兩組患兒臨床療效比較試驗組患兒臨床療效優于對照組,差異有統計學意義(u=1.816,P<0.05,見表2)。

表2 兩組患兒臨床療效比較〔n(%)〕Table 2 Comparison of clinical effect between the two groups
2.2 兩組患兒血清IFN-γ和IL-4水平比較治療前兩組患兒血清IFN-γ、IL-4水平比較,差異無統計學意義(P>0.05);治療后試驗組患兒血清IFN-γ、IL-4水平低于對照組,差異有統計學意義(P<0.05,見表3)。
表3 兩組患兒治療前后血清IFN-γ、IL-4水平比較(±s,μg/L)Table 3 Comparison of serum levels of IFN-γ,IL-4 between the two groups before and after treatment
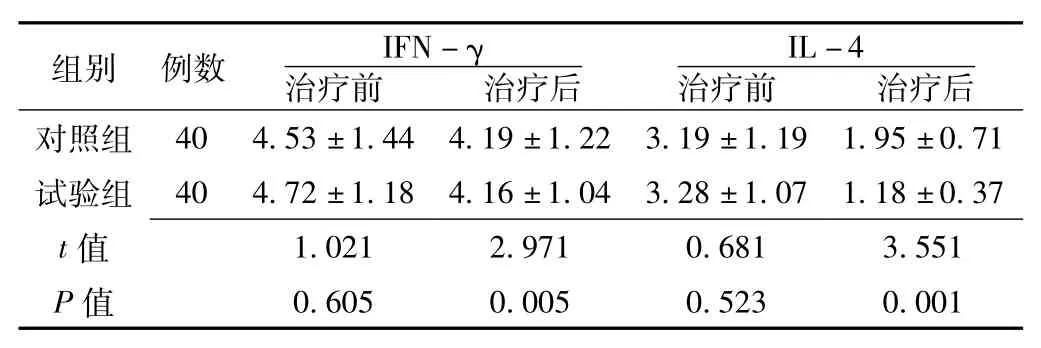
表3 兩組患兒治療前后血清IFN-γ、IL-4水平比較(±s,μg/L)Table 3 Comparison of serum levels of IFN-γ,IL-4 between the two groups before and after treatment
注:IFN-γ=干擾素γ,IL-4=白介素4
組別例數IFN-γ治療前治療后對照組治療后IL-4治療前40 4.53±1.44 4.19±1.22 3.19±1.19 1.95±0.71試驗組40 4.72±1.18 4.16±1.04 3.28±1.07 1.18±0.37 t 1.021 2.971 0.681 3.551 P值值0.605 0.005 0.523 0.001
2.3 兩組患兒Th1、Th2細胞分數及Th1/Th2細胞百分比比較
治療前兩組患兒Th1、Th2細胞分數及Th1/Th2細胞百分比比較,差異無統計學意義(P>0.05);治療后試驗組患兒Th1、Th2細胞分數及Th1/Th2細胞百分比低于對照組,差異有統計學意義(P<0.05,見表4、圖1~2)。
表4 兩組患兒治療前后Th1細胞分數、Th2細胞分數及Th1/Th2細胞百分比比較(±s,%)Table 4 Comparison of Th1,Th2 cell counts and Th1/Th2 cell percentage between the two groups before and after treatment
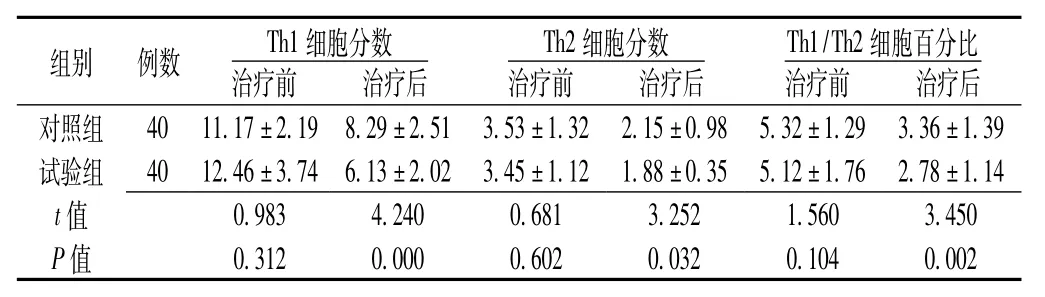
表4 兩組患兒治療前后Th1細胞分數、Th2細胞分數及Th1/Th2細胞百分比比較(±s,%)Table 4 Comparison of Th1,Th2 cell counts and Th1/Th2 cell percentage between the two groups before and after treatment
組別例數Th1細胞分數治療前治療后對照組40 11.17±2.19 8.29±2.51 3.53±1.32 2.15±0.98治療后Th2細胞分數治療前治療后Th1/Th2細胞百分比治療前5.32±1.29 3.36±1.39試驗組40 12.46±3.74 6.13±2.02 3.45±1.12 1.88±0.35 5.12±1.76 2.78±1.14 t 0.983 4.240 0.681 3.252 1.560 3.450 P值值0.312 0.000 0.602 0.032 0.104 0.002
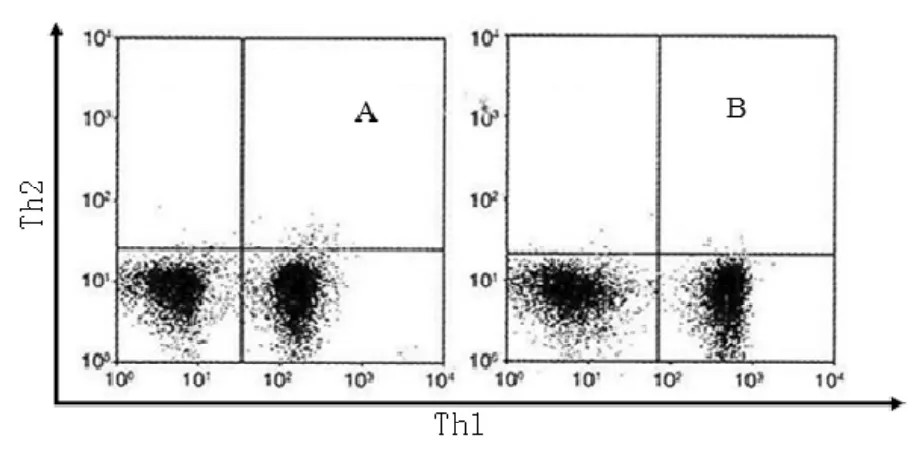
圖1 兩組患兒Th1流式細胞圖Figure 1 Flow cytometry of Th1 between the two groups
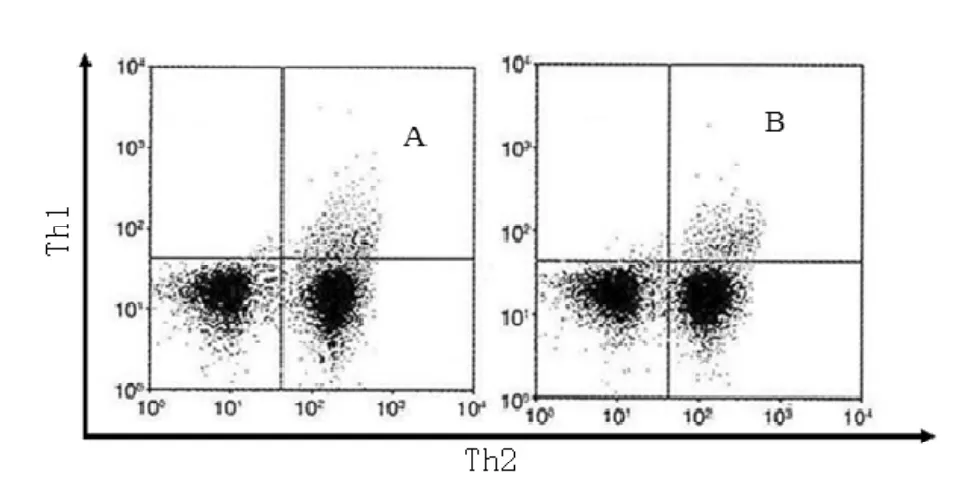
圖2 兩組患兒Th2流式細胞圖Figure 2 Flow cytometry of Th2 between the two groups
3 討論
毛細支氣管炎又稱“喘息性肺炎”,是嬰幼兒特有的呼吸道感染性疾病,其主要臨床表現為呼吸急促、發熱咳嗽、喘息憋悶及吸氣性胸部凹陷等[11]。目前,毛細支氣管炎的發病機制尚未明確,多數學者認為其是由病毒直接作用所致,如流感病毒、鼻病毒、副流感病毒、人類偏肺病毒等,且50%以上是由吸道合胞病毒引起;還有學者認同神經致病機制及免疫病理機制等[12-13]。由于小兒為純陽之體而易感邪化熱,因此,治療應以清肅肺熱、解毒平喘為主[14]。小兒肺熱咳喘口服液方中所含麻杏石甘湯主宣肺止咳,白虎湯清熱生津,配以金銀花、魚腥草清理肺熱,知母、麥冬滋陰解郁除煩,組方合理精辟[15]。本研究結果顯示,小兒肺熱咳喘口服液可以降低毛細支氣管炎患兒Th1和Th2細胞水平,從而提高患兒免疫功能。
Smith等[16]研究顯示,毛細支氣管炎患兒因Th2源性細胞因子作用而易轉變為哮喘,臨床已證實支氣管哮喘發病機制是Th1/Th2細胞和功能失衡所致,且免疫學研究也顯示,毛細支氣管炎與哮喘的發病機制相似,均存在Th1/Th2細胞失調[17-18]。Th1細胞主要分泌IFN-γ,其能促使機體產生白介素12(IL-12),并形成正反饋調節。毛細支氣管炎急性期因抑制Th1細胞功能而不能誘導產生IFN-γ,而經藥物治療后IFN-γ水平升高,提示IFN-γ早期就參與毛細支氣管炎的炎癥免疫過程[19]。毛細支氣管炎是由多種炎性細胞、炎性遞質和細胞因子參與形成的慢性氣道炎癥,具有氣道高反應性、可逆性氣道阻塞和氣道變應性炎癥等臨床特征,其發病過程與Th活化并分泌多種細胞因子密切相關[17-18]。近年有研究顯示,Th1與Th2的失衡與哮喘發生關系密切[19]。正常情況下Th1產生IL-2、IFN-γ及腫瘤壞死因子α、β等多種細胞炎性因子,激活巨噬細胞而發生遲發超敏反應;Th2細胞產生IL -4、IL-5、IL-6、IL-10、IL-13等多種細胞炎性因子,誘導嗜酸粒細胞產生和募集及免疫球蛋白亞型轉化,從而產生IgE。這兩類細胞炎性因子表達的正常調節由Th1/Th2細胞功能的平衡決定。在上述諸多細胞炎性因子中,IL-4與IFN-γ互為拮抗作用,常用來反映Th1/Th2細胞的平衡[20]。Th2細胞主要分泌IL-4,其作用是誘導Th2細胞的生長和分化,并能抑制Th1細胞產生IFN-γ,其在變應性炎癥的發生發展中具有重要作用[20]。本研究結果顯示,治療后試驗組患兒血清IFN-γ和IL-4水平低于對照組,且Th1細胞分數、Th2細胞分數及Th1/Th2細胞百分比低于對照組,提示小兒肺熱咳喘口服液可以降低毛細支氣管炎患兒Th1/Th2細胞水平。
綜上所述,小兒肺熱咳喘口服液治療小兒毛細支氣管炎臨床療效良好,可通過調節Th1/Th2細胞而增加患兒免疫功能,值得臨床推廣應用。
[1]Openshaw PJ,Tregoning JS.Immune responses and disease enhancement during respiratory syncytial virus infection[J].Clin Microbiol Rev,2005,18(3):541-555.
[2]Legg JP,Hussain IR,Warner JA,et al.Type 1 and type 2 cytokine im-balance in acute respiratory syncytialvirusbronchiolitis[J].Am J Respir Crit Care Med,2003,168(6):633-639.
[3]Takemura M,Niimi A,Matsumoto H,et al.Clinical,physiological and anti-inflammatory effect of montelukast in patients with?cough variant asthma[J].Respiration,2012,83(4):308-315.
[4]Tripp RA,Oshansky C,Alvarez R.Cytokines and Respiratory Syncytial Virus Infection[J].Proc Am Thorac Soc,2005,2 (2):147-149.
[5]Pinto RA,Arredondo SM,Bono MR,et al.Thelper1/Thelper2 cyto -kine imbalance in respiratory syncytial virus infection is associated with increased endogenous plasma cortisol[J].Pediatrics,2006,117(5):e878-e886.
[6]Tamaoki J,Yokohori N,Tagaya E,et al.Comparable effect of a leukotriene receptor antagonist and long-acting beta-adrenergic agonist incough variant asthma[J].Allergy Asthma Proc,2010,31 (5):78-84.
[7]Legg JP,Hussain IR,Warner JA,et al.Type 1 and type 2 cytokine imbalance in acute respiratory syncytial virus bronchiolitis[J].Am J Respir Crit Care Med,2003,168(6):633-639.
[8]CostaML,Stein RT,Bauer ME.Levels of Th1 and Th2 cytokines in children with post-infectious bronchiolitis obliterans[J].Ann Trop Paediatr,2005,25(4):261-266.
[9]Matsuoka H,Niimi A,Matsumoto H,et al.Inflammatory subtypes
in coughvariant asthma:association with maintenance doses of inhaled corticosteroids[J].Chest,2010,138(6):1418-1425.
[10]Brandenburg AH,Kleinjan A,van Het Land B,et al.Type1-like immune response is found in children with respiratory syncy-tial virus infection regardless of clinical severity[J].J Med Virol,2000,62(2):267-277.
[11]Flamant C,Hallalel F,Nolent P,et al.Severe respiratory syncytialvirus bronchiolitis in children:From short mechanical ventilation to extracor-porealmembrane oxygenation[J].EurJPediatr,2005,164(2):93-98.
[12]Bartz H,Turkel O,Hoffjan S,et al.Respiratory syncytial virus decreases the capacity of myeloid dendritic cells to induce inter-feron -gamma in naive T cells[J].Immunology,2003,109(1):49 -57.
[13]Piedimonte G,Renzetti G,Auais A,et al.Leukotriene synthesis during respiratory syncytial virus bronchiolitis:influence of age and atopy[J].Pediatr Pulmonol,2005,40(4):285-291.
[14]Bendelja K,Gagro A,Bace A,et al.Predominant type 2 response in infants with respiratory syncytial virus(RSV)infection demonstrated by cytokine flow cytometry[J].Clin Exp Immunol,2000,121(2):332-338.
[15]Bacharier LB,Boner A,Carlsen KH,et al.Diagnosis and treatment of asthma in childhood:a PRACTALL consensus report[J].Allergy,2008,63(1):5-34.
[16]Smith PK,Wang SZ,Dowling KD,et al.Leucocyte populationsin respiratory syncytial virus-induced bronchiolitis[J].J Paediatr Child Health,2001,37(2):146-151.
[17]Papadopoulos NG,Arakawa H,Carlsen KH,et al.International consensus on(ICON)pediatric asthma[J].Allergy,2012,67 (8):976-997.
[18]Yu I,Yoo Y,Kim DK,et al.Distribution of antibody time to Mycoplasma pneumoniae in Korean children in 2000—2003[J].J Korean Med Sci,2005,20(4):542-547.
[19]Oommen A,Grigg J.Urinary leukotriene E4 in preschool children with acute clinical viral wheeze[J].Eur Respir J,2003,21(1): 149-154.
[20]Bukstein DA,Luskin AT,Bernstein A."Real world"effective daily controller medicine in children with mild persistent asthma[J].Ann Allergy Asthma Immunol,2003,90(5):543-549.
Im pact of Xiaoer-feire-kechuan O ral Solution on Th1/Th2 Cells of Infants w ith Bronchiolitis
LI Jing,DONG Yan,ZHANG Jing-jie,et al.
Integrated Chinese and Western Medicine Hospital of Changping District,Beijing 102208,China
Objective To explore the impact of xiaoer-feire-kechuan oral solution on Th1/Th2 cells of infants with bronchiolitis.M ethods A total of 80 infants with bronchiolitis that hospitalized in Department of Pediatrics,Integrated Chinese and Western Medicine Hospital of Changping District were selected from September 2013 to December 2014,and they were divided into experiment group and control group according to random number table,each of 40 cases.Infants of both groups were given anti-infectious therapy and symptomatic treatment according to clinical medication guides,and infants of control group were given extra intravenous drip of ceftriaxone sodium,while infants of experiment group were given extra xiaoer-feirekechuan oral solution based on the treatment of control group,both groups treated for 7 days.Clinical effect,serum levels of IFN -γ and IL-4,Th1 cell counts,Th2 cell counts and Th1/Th2 cell percentage before and after treatment were compared between the two groups,and incidence of adverse reactions were observed.Results The clinical effect of experiment group was statistically significantly better than that of control group(P<0.05).No statistically significant differences of serum levels of IFN-γ and IL-4,Th1 cell counts,Th2 cell counts or Th1/Th2 cell percentage were found between the two groups before treatment(P>0.05);while serum levels of IFN-γ and IL-4,Th1 cell counts,Th2 cell counts and Th1/Th2 cell percentage of experiment group were lower than those of control group after treatment(P<0.05).Conclusion Xiaoer-feire-kechuan oral solution can has a certainly good clinical effect on bronchiolitis in infants,it may adjust Th1/Th2 cells to improve the immune function.
Bronchiolitis;Feirekechuan oral liquid;Th1-Th2 balance
R 562.21
B
10.3969/j.issn.1008-5971.2015.04.038
2015-02-13;
2015-04-15)
(本文編輯:謝武英)
102208北京市昌平區中西醫結合醫院
猜你喜歡
基層中醫藥(2021年2期)2021-07-23 01:41:54
基層中醫藥(2021年10期)2021-06-05 07:15:14
幽默大師(2020年11期)2020-11-26 06:12:18
幽默大師(2020年10期)2020-11-10 09:07:20
家庭醫學(下半月)(2020年1期)2020-05-11 02:05:36
海峽姐妹(2019年12期)2020-01-14 03:24:46
家庭醫學(下半月)(2019年10期)2019-11-16 08:59:46
家庭醫學(下半月)(2019年10期)2019-11-16 08:59:46
家庭醫學(下半月)(2019年10期)2019-11-16 08:59:44
云南中醫學院學報(2014年3期)2014-07-31 18:57:41
