兒童急性下呼吸道感染相關危險因素的Meta分析
2015-11-18 12:21:52付卓萬莉雅徐勇勝鄭躍杰
天津醫藥 2015年9期
付卓,萬莉雅△,徐勇勝,鄭躍杰
兒童急性下呼吸道感染相關危險因素的Meta分析
付卓1,萬莉雅1△,徐勇勝1,鄭躍杰2
目的探討兒童急性下呼吸道感染(ALRI)的相關危險因素,為其防治提供科學依據。方法計算機檢索PubMed、Databases-Medline(Ovid)、Embase、CINAHL和Global Health Library、中國知網(CNKI)、維普(VIP)和萬方數據庫,查找有關兒童急性下呼吸道感染的危險因素的期刊與論文,檢索時限均為1990年1月—2014年12月。根據文獻納入與排除標準,由2位評價員獨立進行文獻資料的篩選與提取并質量評價后,采用Stata 11.0軟件進行Meta分析。結果對納入的27篇文獻進行Meta分析,結果顯示,低出生體質量、缺乏充足的母乳喂養、房間擁擠、室內空氣污染、營養不良、處于吸煙環境(或孕婦吸煙)和HIV接觸史(未感染情況)與ALRI密切相關。結論上述7種危險因素在ALRI進程中起重要作用,還需進一步研究發現其他潛在的危險因素,以降低兒童ALRI的可能性。
呼吸道感染;急性病;危險因素;Meta分析;兒童
急性下呼吸道感染(acute lower respiratory infec?tion,ALRI)是5歲以下兒童發病率和死亡率最高的疾病之一[1]。據世界衛生組織統計,全世界每年大約有430萬5歲以下兒童死于ALRI,占該年齡組死亡人數的30%,其中肺炎占80%~90%[2]。在我國,兒童ALRI的發病率及死亡率均居首位,其發病率占兒科住院患兒的24.5%~65.2%,占兒科門診的39%~65.5%。5歲以下兒童中每年有105萬人死亡,其中30萬死于肺炎,為該年齡組的第1位死因[3]。目前,僅有少數研究調查了兒童ALRI與危險因素之間的關系,尚缺乏對已發表的評估兒童ALRI與危險因素關系文獻的系統性回顧。本研究通過查閱和篩選近5年國內外發表的關于兒童急性下呼吸道感染發病危險因素的相關病例對照研究文獻,采用Stata 11.0軟件進行了系統性Meta分析,旨在探討當前兒童ALRI的主要危險因素,為其預防和治療提供科學依據。
1 資料與方法
1.1 檢索策略采用計算機檢索:Pubmed、Databases-Med?line(Ovid)、Embase、CINAHL Health Library和Global Health Library、中國知網(CNKI)、中國維普科技期刊數據庫(VIP)及萬方數據庫。檢索的時間范圍為1990年1月—2014年12月。檢索詞包括:中文“兒童急性下呼吸道感染”、“危險因素”;英文“acute lower respiratory infection in children”、“risk factors”。共檢索到53條文獻。
1.2 文獻納入及排除標準納入標準:(1)急性下呼吸道感染病例是參照WHO的病例進行定義的[4-5]。(2)1990—2014年國內外發表的關于兒童急性下呼吸道感染的危險因素研究。(3)開展的研究有明確的年限。(4)研究樣本量>100例。(5)研究數據包含OR值及95%CI或可以通過統計學方法轉化為OR值及95%CI。(6)各文獻研究方法相似。排除標準:參考Song等[6]提供的標準對每篇文獻進行質量評價,排除研究信息少、研究內容重復和陳舊、統計學信息不全及無法利用的文獻。根據以上標準,由2名評價員分別閱讀檢索到的文獻題目及摘要進行初步篩選,對明顯不符合納入標準的文獻予以排除,符合的則閱讀全文,決定是否納入,最終有27篇文獻符合納入標準。
1.3 文獻提取由2名評價員獨立獲取文獻,互相核對獲取文獻結果。獲取文獻的主要內容包括:文獻的基本信息,包括作者、發表時間、研究設計類型和樣本量;研究對象,包括年齡、診斷;相關危險因素。
1.4 數據的統計學方法提取文獻信息后,按統計學Meta分析的要求整理并核對文獻數據,建立納入文獻數據基本情況表。采用Stata 11.0軟件進行Meta分析。分類變量使用OR和95%CI表示。首先對各納入研究結果間的異質性進行檢驗,若P>0.05且I2≤50%,采用固定效應模型進行Meta分析;反之則采用隨機效應模型。最后進行效應量的合并統計分析,若OR>1,I2<50%,該因素為兒童ALRI的危險因素;反之為保護因素。納入的文獻是否存在發表偏倚則通過Begg's檢驗,當P>0.05時認為不存在發表偏倚,P≤0.05時則存在發表偏倚。
2 結果
2.1 檢索結果及納入文獻的基本情況本研究初步檢索文獻53篇,根據本文擬定的文獻納入與排除標準和質量評價標準,閱讀摘要及全文后,最終27篇文獻納入本次Meta分析研究。納入文獻的基本情況見表1。
2.2 兒童ALRI危險因素的Meta分析
2.2.1 低出生體質量8個研究[7-14]記錄了低出生體質量與兒童ALRI之間的相關性,8篇研究文獻間不存在異質性(P=0.800,I2=0.0),采用固定效應模型。結果顯示,低出生體質量為兒童ALRI危險因素(OR=1.55,95%CI:1.32~1.78),見圖1。
2.2.2 缺乏母乳喂養7個研究[7-8,10,15-18]記錄了缺乏母乳喂養與兒童ALRI之間的相關性,2篇文獻[12,19]報道了母乳喂養與兒童ALRI之間的關聯,研究文獻不存在異質性(P=0.095,I2=44.4%),采用固定效應模型。結果顯示,缺乏充足的母乳喂養為兒童ALRI危險因素(OR=2.03,95%CI:1.82~2.24),見圖2、3。
2.2.3 居住條件擁擠7個研究[7-8,10,13,18,20-21]記錄了居住條件擁擠與兒童ALRI之間的相關性,7篇研究文獻不存在異質性(P=0.621,I2=0.0%),采用固定效應模型。結果顯示,居住條件擁擠為兒童ALRI危險因素(OR=2.22,95%CI:1.84~2.60),見圖3。
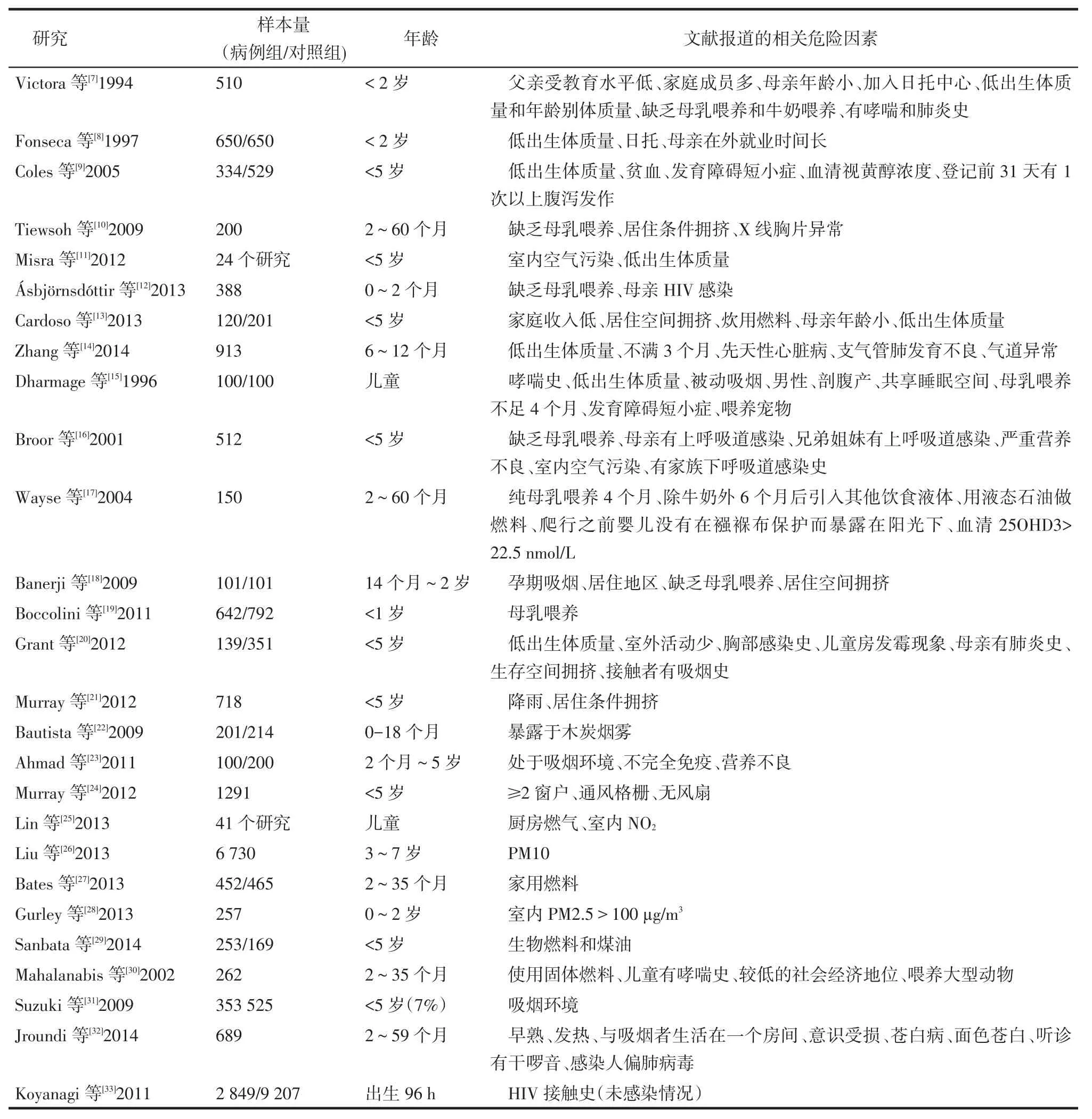
Tab.1 Basic information of inclusive literature表1 納入文獻基本信息
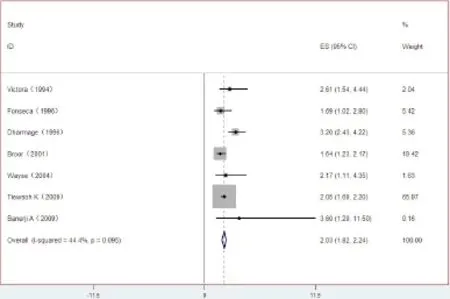
Fig.2 The forest plot of non-breast feeding and childhood ALRI圖2 缺乏母乳喂養與兒童ALRI關系的森林圖
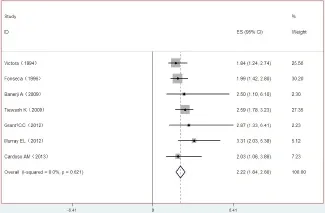
Fig.3 The forest plot of crowded household and childhood ALRI圖3 居住條件擁擠與兒童ALRI關系的森林圖
2.2.4 室內空氣污染10個研究[8,16,22-29]記錄了室內空氣污染與兒童ALRI的相關性,10篇研究文獻不存在異質性(P=0.069,I2=39.7%),采用固定效應模型。結果顯示,室內空氣污染為兒童ALRI危險因素(OR=1.12,95%CI:1.07~1.17),見圖4。
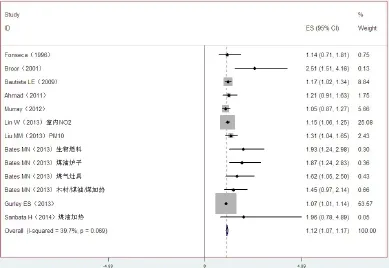
Fig.4 The forest plot of indoor air pollution and childhood ALRI圖4 室內空氣污染與兒童ALRI關系的森林圖
2.2.5 營養不良3個研究[12,20,30]記錄了營養不良與兒童ALRI之間的相關性,3篇研究文獻不存在異質性(P=0.481,I2=0.0%),采用固定效應模型。結果顯示,營養不良為兒童ALRI危險因素(OR=1.31,95%CI:1.12~1.51),見圖5。
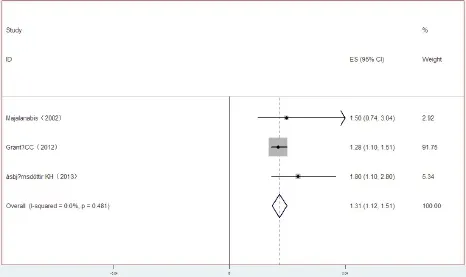
Fig.5 The forest plot of undernutrition and childhood ALRI圖5 營養不良與兒童ALRI關系的森林圖
2.2.6 處于吸煙環境/孕婦吸煙4個研究[18,20,31-32]記錄了處于吸煙環境/孕期吸煙與兒童ALRI之間的相關性,4篇研究文獻不存在異質性(P=0.776,I2=0.0),采用固定效應模型。結果顯示,處于吸煙環境[18,31-32]或是孕婦吸煙[20]為兒童ALRI危險因素(OR=1.61,95%CI:1.31~1.91),見圖6。
2.2.7 HIV接觸史(未感染情況)2個研究[12,33]記錄了HIV接觸史與兒童ALRI之間的相關性,2篇研究文獻不存在異質性(P=0.187,I2=42.5%),采用固定效應模型。結果顯示,HIV接觸史為兒童ALRI危險因素(OR=1.26,95%CI:1.02~1.49),見圖7。
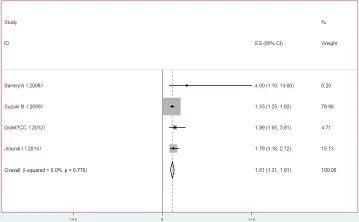
Fig.6 The forest plot of living in a house with smokers or smoking in pregnant and childhood ALRI圖6 處于吸煙環境或孕期吸煙與兒童ACRI關系的森林圖
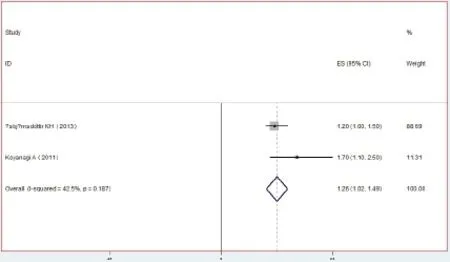
Fig.7 The forest plot of HIV-exposed uninfected children圖7 接觸過HIV(未感染情況)與兒童ALRI關系的森林圖
2.3 各研究發表偏倚分析低出生體質量和室內空氣污染對應的文獻存在發表偏倚(Z分別為2.35和2.38,P<0.05),缺乏母乳喂養、居住條件擁擠、營養不良、吸煙環境和HIV感染對應的文獻都不存在發表偏倚(Z分別為0.90、0.00、0.00、0.70和0.00,均P>0.05)。
3 討論
ALRI是兒科的常見疾病,是導致兒童死亡的主要原因。大多數早產兒和小于胎齡兒均是低出生體質量兒,體質量不足2 500 g[25]。低出生體質量兒的主要缺陷是呼吸中樞及器官發育不成熟,缺乏肺泡表面活性物質,從母體中獲得的抗體相對少。因此,低出生體質量兒較易引起ALRI。本研究以“低出生體質量”和“兒童急性下呼吸道感染(ALRI)”為關鍵詞篩選并納入的8篇文獻,均報道了低出生體質量兒是ALRI的主要危險因素,說明低出生體質量與兒童ALRI緊密相關。
母乳中的表皮生長因子可幫助誘導腸上皮細胞成熟,免疫球蛋白A和低聚糖可防止病原體黏附,而乳鐵蛋白具有廣譜抗微生物特性,包括破壞細菌外膜[26-27]。純母乳喂養可以減少嬰兒發生感染性疾病的危險[28]。缺乏母乳喂養可增加疾病的嚴重程度,包括接受住院治療和住院的頻率。關于缺乏母乳喂養可引起兒童ALRI的文獻報道很多,本研究經篩選后有7篇文獻納入到危險因素Meta分析中,結果顯示缺乏母乳喂養是兒童ALRI的主要危險因素。
居住條件擁擠、室內空氣污染(做飯使用燃料)、處于吸煙環境(或孕婦吸煙)均是室內空氣污染的最主要污染源。為了節能,現代建筑在設計時傾向于使用非透氣材料,居住者人數、做飯使用燃料及所釋放的油煙和家庭成員吸煙行為都是室內空氣質量好壞的決定性因素。煙草或植物燃燒產生的煙霧含有很多包裹著復雜有機化合物的碳基顆粒,這些微塵顆粒足夠小,使其能夠避開人體呼吸道系統的防御機能,并深入肺組織,對于兒童甚至嬰幼兒的健康構成了最大的潛在威脅。本研究發現,房間擁擠、室內空氣污染(做飯使用燃料)、處于吸煙環境(或孕婦吸煙)都是兒童ALRI的主要危險因素。
喂養不當、飲食習慣不良和疾病因素是營養不良的主要病因。長期攝食不足、人工喂養者和不恰當的斷奶期是嬰兒營養不良的主要因素。可見,本研究報道的各危險因素之間也是互為因果關系,相輔相成的。有關營養不良的報道在本研究共篩選到4篇文獻,其中有1篇報道的95%CI是無效的,因此,僅對3篇文獻進行了分析,證實了營養不良是造成兒童ALRI的主要危險因素。
有HIV接觸史(未感染情況)的嬰幼兒比無HIV接觸史的嬰幼兒具有更高的發病率和病死率,可能是這個弱勢群體面臨的健康問題[9]。本研究只篩選到2篇文獻報道了HIV接觸史(未感染情況)與兒童ALRI的關系,結果表明HIV接觸史(未感染情況)是兒童ALRI的主要危險因素。
另外,納入本研究的文獻還報道了其他兒童ALRI的危險因素,由于這些危險因素報道頻次較少,不符合Meta分析的要求,因此,本次Meta分析不予以統計分析。本文還對每個研究對應的文獻逐個進行發表偏倚分析。Begg's檢驗結果顯示,低出生體質量和室內空氣污染對應的文獻存在發表偏倚,可能的原因是納入的文獻中存在樣本量小,設計簡單的研究。由于文獻質量的限制,尚需更多設計良好的多中心、大樣本的隨機對照試驗加以驗證,并再次進行Meta分析以便為臨床提供更好的證據。
[1]Lozano R,Naghavi M,Foreman K,et al.Global and regional mortal?ity from 235 causes of death for 20 age groups in 1990 and 2010:a systematic analysis for the Global Burden of Disease Study 2010[J]. Lancet,2012,380(9859):2095-2128.doi:10.1016/S0140-6736(12)61728-0.
[2]Kwon HJ,Rhie YJ,Seo WH,et al.Clinical manifestations of respira? tory adenoviral infection among hospitalized children in Korea[J]. Pediatr Int,2013,55(4):450-454.doi:10.1111/ped.12108.
[3]Liu L,Johnson HL,Cousens S,et al.Global,regional,and national causes of child mortality:an updated systematic analysis for 2010 with time trends since 2000[J].Lancet,2012,379:2151-2161.doi:10.1016/S0140-6736(12)60560-1.
[4]Persell SD,Friedberg MW,Meeker D,et al.Use of behavioral eco?nomics and social psychology to improve treatment of acute respira?tory infections(BEARI):rationale and design of a cluster random?ized controlled trial[1RC4AG039115-01]-study protocol and baseline practice and provider characteristics[J].BMC Infectious Diseases,2013,13:290.doi:10.1186/1471-2334-13-290.
[5]Woodhead M,Blasi F,Ewig S,et al.Guidelines for the management of adult lower respiratory tract infections--summary[J].Clin Micro?biol Infect,2011,17 Suppl 6:1-24.doi:10.1111/j.1469-0691. 2011.03602.x.
[6]Song JW,Chung KC.Observational studies:cohort and case-con?trol studies[J].Plast Reconstr Surg,2010,126(6):2234-2242.doi:10.1097/PRS.0b013e3181f44abc.
[7]Victora CG,Fuchs SC,Flores JA,et al.Risk factors for pneumonia among children in a Brazilian metropolitan area[J].Pediatrics,1994,93(6 Pt 1):977-985.
[8]Fonseca W,Kirkwood BR,Misago C.Factors related to child care increase the risk of pneumonia among children living in a poor com?munity in northeast Brazil[J].J Trop Pediatr,1997,43(2):123-124. doi:10.1093/tropej/43.2.123.
[9]Coles CL,Fraser D,Givon-Lavi N,et al.Nutritional status and diar?rheal illness as independent risk factors for alveolar pneumonia[J].Am J Epidemiol,2005,162(10):999-1007.doi:10.1093/aje/kwi312.
[10]Tiewsoh K,Lodha R,Pandey RM,et al.Factors determining the out?come of children hospitalized with severe pneumonia[J].BMC Pedi?atr,2009,9:15.doi:10.1186/1471-2431-9-15.
[11]Misra P,Srivastava R,Krishnan A,et al.Indoor air pollution-relat?ed acute lower respiratory infections and low birth weight:a system?atic review[J].J Trop Pediatr,2012,58(6):457-466.doi:10.1093/ tropej/fms017.
[12]ásbj?rnsdóttir KH,Slyker JA,Weiss NS,et al.Breastfeeding is as?sociated with decreased pneumonia incidence among HIV-exposed,uninfected Kenyan infants[J].AIDS,2013,27(17):2809-2815.doi:10.1097/01.aids.0000432540.59786.6d.
[13]Cardoso AM,Coimbra CE Jr,Werneck GL.Risk factors for hospital admission due to acute lower respiratory tract infection in Guarani indigenous children in southern Brazil:a population-based casecontrol study[J].Trop Med Int Health,2013,18(5):596-607.doi:10.1111/tmi.12081.
[14]Zhang XB,Liu LJ,Qian LL,et al.Clinical characteristics and risk factors of severe respiratory syncytial virus-associated acute low?er respiratory tract infections in hospitalized infants[J].World J Pe?diatr,2014,10(4):360-364.doi:10.1007/s12519-014-0513-x.
[15]Dharmage SC,Rajapaksa LC,Fernando DN.Risk factors of acute lower respiratory tract infections in children under five years of age[J].Southeast Asian J Trop Med Public Health,1996,27(1):107-110.PMID:9031411.
[16]Broor S,Pandey RM,Ghosh M,et al.Risk factors for severe acutelower respiratory tract infection in under-five children[J].Indian Pe?diatr,2001,38(12):1361-1369.
[17]Wayse V,Yousafzai A,Mogale K,et al.Association of subclinical vitamin D deficiency with severe acute lower respiratory infection in Indian children under 5 y[J].Eur J Clin Nutr,2004,58(4):563-567. doi:10.1038/sj.ejcn.1601845.
[18]Banerji A,Greenberg D,White LF,et al.Risk factors and viruses associated with hospitalization due to lower respiratory tract infections in Canadian Inuit children:a case-control study[J].Pediatr Infect Dis J,2009,28(8):697-701.doi:10.1097/INF.0b013e31819f1f89.
[19]Boccolini CS,Carvalho ML,Oliveira MI,et al.Breastfeeding can prevent hospitalization for pneumonia among children under 1 year old[J].J Pediatr(Rio J),2011,87(5):399-404.doi:10.2223/JPED.2136.
[20]Grant CC,Emery D,Milne T,et al.Risk factors for community-ac?quired pneumonia in pre-school-aged children[J].J Paediatr Child Health,2012,48(5):402-412.doi:10.1111/j.1440-1754.2011. 02244.x.
[21]Murray EL,Klein M,Brondi L,et al.Rainfall,household crowding,and acute respiratory infections in the tropics[J].Epidemiol In?fect,2012,140(1):78-86.doi:10.1017/S0950268811000252.
[22]Bautista LE,Correa A,Baumgartner J,et al.Indoor charcoal smoke and acute respiratory infections in young children in the Dominican Republic[J].Am J Epidemiol,2009,169(5):572-580.doi:10.1093/ aje/kwn372.
[23]Ahmad I,Shaheen N,Khan S.Risk factors for pneumonia among hospitalized children between 2 months to 5 years[J].Pak J Med Sci,2011,19(2):89-94.
[24]Murray EL,Brondi L,Kleinbaum D,et al.Cooking fuel type,house?hold ventilation,and the risk of acute lower respiratory illness in ur?ban Bangladeshi children:a longitudinal study[J].Indoor Air,2012,22(2):132-139.doi:10.1111/j.1600-0668.2011.00754.x.
[25]Lin W,Brunekreef B,Gehring U.Meta-analysis of the effects of in?door nitrogen dioxide and gas cooking on asthma and wheeze in chil?dren[J].Int J Epidemiol,2013,42(6):1724-1737.doi:10.1093/ije/ dyt150.
[26]Liu MM,Wang D,Zhao Y,et al.Effects of outdoor and indoor air pollution on respiratory health of Chinese children from 50 kinder?gartens[J].J Epidemiol,2013,23(4):280-287.doi:10.2188/jea. JE20120175.
[27]Bates MN,Chandyo RK,Valentiner-Branth P,et al.Acute lower re?spiratory infection in childhood and household fuel use in Bhak?tapur,Nepal[J].Environ Health Perspect,2013,121(5):637-642. doi:10.1289/ehp.1205491.
[28]Gurley ES,Homaira N,Salje H,et al.Indoor exposure to particulate matterandtheincidenceof acute lower respiratory infec?tions among children:abirthcohortstudyinurbanBangladesh[J].In?door Air,2013,23(5):379-386.doi:10.1111/ina.12038.
[29]Sanbata H,Asfaw A,Kumie A.Association of biomass fuel use with acute respiratory infections among under-five children in a slum urban of Addis Ababa,Ethiopia[J].BMC Public Health,2014,14:1122.doi:10.1186/1471-2458-14-1122.
[30]Mahalanabis D,Gupta S,Paul D,et al.Risk factors for pneumonia in infants and young children and the role of solid fuel for cooking:a case-control study[J].Epidemiol Infect,2002,129(1):65-71.
[31]Suzuki M,Thiem VD,Yanai H,et al.Association of environmental tobacco smoking exposure with an increased risk of hospital admis?sions for pneumonia in children under 5 years of age in Vietnam[J]. Thorax,2009,64(6):484-489.doi:10.1136/thx.2008.106385.
[32]Jroundi I,Mahraoui C,Benmessaoud R,et al.Risk factors for a poor outcome among children admitted with clinically severe pneumonia to a university hospital in Rabat,Morocco[J].Int J Infect Dis,2014,28:164-170.doi:10.1016/j.ijid.2014.07.027.
[33]Koyanagi A,Humphrey JH,Moulton LH,et al.Predictive value of weight loss on mortality of HIV-positive mothers in a prolonged breastfeeding setting[J].AIDS Res Hum Retroviruses,2011,27(11):
(2015-01-23收稿2015-05-12修回)
(本文編輯魏杰)
Meta-analysis of risk factors of severe acute lower respiratory infections in children
FU Zhuo1,WAN Liya1△,XU Yongsheng1,ZHENG Yuejie2
1 Tianjin Children's Hospital,Tianjin 300134,China;2 Zunyi Medical University,Shenzhen Children's Hospital△
ObjectiveTo identify the risk factors for severe acute lower respiratory infections(ALRI)in children and to provide scientific basis for prevention and treatment of ALRI.MethodsSeveral databases including Pubmed,Databases-Medline(Ovid),Embase,CINAHL and Global Health Library,CNKI,VIP and Wanfang Date were searched(1990.1-2014.12)for
.All selected studies were about risk factors of ALRI in children.The screening and quality evalua?tion of the literature data was conducted independently by two reviewers according to the inclusion and exclusion criteria. Stata 11.0 software was used for Meta-analysis.ResultsMeta-analysis of 27 included literature showed that seven risk fac?tors were significantly associated with severe ALRI:low birth weight,lack of exclusive breastfeeding,crowded household,ex?posure to indoor air pollution,malnutrition,living in a house with smokers or smoking in pregnant and HIV-exposed unin?fected condition.ConclusionThe above seven risk factors play the important role in the development of ALRI in children. Furthermore,it emphasizes the need for further studies investigating other potential risk factors to decrease the possibility of childhood ALRI.
respiratory tract infections;acute disease;risk factors;meta-analysis;child
R725.6
A
10.11958/j.issn.0253-9896.2015.09.033
1天津市兒童醫院呼吸科(郵編300134);2遵義醫學院深圳兒童醫院
付卓(1977),女,碩士研究生,主要從事小兒呼吸內科方面研究
△通訊作者E-mail:wanliya_1209@163.com
猜你喜歡
中學生數理化·八年級物理人教版(2021年12期)2021-12-31 03:23:08
民用飛機設計與研究(2020年4期)2021-01-21 09:15:02
中學生數理化·中考版(2020年10期)2020-11-27 01:59:48
中國生殖健康(2019年2期)2019-08-23 08:12:08
電子制作(2018年18期)2018-11-14 01:48:24
山東工業技術(2016年15期)2016-12-01 05:31:22
雜文選刊(2016年7期)2016-08-02 08:39:56
小天使·一年級語數英綜合(2016年6期)2016-05-14 12:21:05
汽車觀察(2016年3期)2016-02-28 13:16:26
小學生·新讀寫(2006年6期)2006-06-14 05:16:24