山羊上頜竇及額竇黏膜厚度與可承受壓強相關研究
2016-07-22 10:40:46呂源韓奕詩李巖峰任桓樊佳東劉茜胡品包文雅
華西口腔醫學雜志 2016年1期
呂源韓奕詩李巖峰任桓樊佳東劉茜胡品包文雅
1.遼寧醫學院解放軍總醫院第一附屬醫院研究生培養基地,錦州 121000;2.解放軍總醫院第一附屬醫院口腔科,北京 100048;3.78086部隊50分隊衛生所,成都 610017;4.解放軍總醫院第一附屬醫院病理科,北京 100048
?
山羊上頜竇及額竇黏膜厚度與可承受壓強相關研究
呂源1韓奕詩2李巖峰2任桓3樊佳東2劉茜4胡品2包文雅2
1.遼寧醫學院解放軍總醫院第一附屬醫院研究生培養基地,錦州 121000;2.解放軍總醫院第一附屬醫院口腔科,北京 100048;3.78086部隊50分隊衛生所,成都 610017;4.解放軍總醫院第一附屬醫院病理科,北京 100048
[摘要]目的 探討山羊上頜竇及額竇黏膜的厚度及可承受壓強的差異,并分析造成這種差異的可能原因,為上頜竇提升術中涉及黏膜問題時提供理論依據和指導。方法 從獲取的每塊黏膜上切取2塊所需大小的黏膜,中性甲醛溶液固定24 h后,將黏膜制成組織切片,用于測量黏膜厚度,另一塊黏膜用于可承受壓強數值的測定,再進行二者相關性的分析,選擇合適的統計方法和軟件。結果 山羊上頜竇頂、上頜竇底、額竇黏膜厚度分別為(410.03±65.97)、(461.33±91.37)、(216.90±46.47) μm。山羊上頜竇頂、上頜竇底、額竇黏膜可承受壓強分別為(260.08±80.12)、(306.90±94.37)、(121.72±31.72) kPa。上頜竇頂與額竇、上頜竇底與額竇、上頜竇頂與竇底黏膜的厚度均值之間差異有統計學意義(P<0.05),可承受壓強均值之間差異也有統計學意義(P<0.05)。結論 上頜竇頂、底黏膜較額竇黏膜厚度及可承受壓強均大,上頜竇底黏膜較上頜竇頂黏膜厚度和可承受壓強稍偏大,并且竇黏膜可承受壓強與黏膜厚度之間成正相關關系。
[關鍵詞]山羊; 上頜竇底提升; 竇黏膜; 黏膜厚度; 可承受壓強
上頜竇黏膜的生物學特性與上頜竇提升時黏膜剝離的難易和成骨效果等因素密切相關,因此研究上頜竇黏膜生物學特性對上頜竇提升術中黏膜的剝離與提升有重要指導意義。本研究將通過建立體外動物模型,對山羊鼻竇(上頜竇、額竇)黏膜的厚度和可承受壓強相關問題進行研究和探討,以期加深對上頜竇黏膜特性的理解,為上頜竇提升術中涉及到的黏膜特性問題和種植體植入提供理論依據和指導。
1 材料和方法
1.1 動物及材料、設備
選取解放軍總醫院第一附屬醫院動物實驗中心提供的5只山羊,年齡為1~2歲,雌雄不限,體態身形大小接近,身體健康,口腔、上頜竇無異常。
骨鋸(天津宇通醫療器械廠),剪刀、彎止血鉗、無齒鑷、刀片(上海偉榮醫療器材有限公司),刻度尺(寧波得力文具有限公司),推拉力計(溫州一鼎儀器制造有限公司),CT設備(PHILIPS公司,荷蘭),顯微鏡(Olympus公司,日本)。
1.2 方法
1.2.1 實驗模型的獲得[1]將山羊頭顱行CT掃描和三維重建分析后進行剝皮、劃線和截骨(圖1),最終每只山羊均可獲得左右各2個上頜竇頂、上頜竇底、額竇共6個竇腔。

圖 1 劃分截骨線Fig 1 Divide osteotomy line
1.2.2 實驗過程 各竇腔黏膜剝離下來以后均切取20 mm×20 mm方形黏膜和大于5 mm×10 mm的任意形狀黏膜。先將后者置于10%中性甲醛溶液中固定24 h后制成黏膜組織切片,在帶有刻度目鏡的光學顯微鏡下隨機選取每張切片的3處位點進行讀數并記錄(圖2),數值經單位換算最終得到黏膜厚度值。將方形黏膜展平置于自制同心環形夾具間后擰緊螺絲,將推拉力計推力端與自制壓具連接后對夾具內環所暴露的中央部位黏膜均勻施加垂直向下的壓力,直至黏膜破裂,讀數并記錄。
1.3 統計學分析
采用SPSS 17.0軟件包對實驗數據進行分析,其中對黏膜厚度及可承受壓強分別選擇配對t檢驗,黏膜厚度和可承受壓強二者之間的相關性研究選擇線性回歸。所有P值均為雙邊,P<0.05為差異有統計學意義。

圖 2 測量黏膜 HE × 100Fig 2 Measure the membrane HE × 100
2 結果
山羊上頜竇頂、上頜竇底、額竇黏膜厚度分別為(410.03±65.97)、(461.33±91.37)、(216.90± 46.47) μm。山羊上頜竇頂、上頜竇底、額竇黏膜可承受壓強分別為(260.08±80.12)、(306.90± 94.37)、(121.72±31.72) kPa。上頜竇頂與額竇(t=7.479,P=0.000)、上頜竇底與額竇(t=7.128,P=0.000)、上頜竇頂與竇底(t=-2.953,P=0.016)黏膜厚度間差異均有統計學意義(P<0.05)。上頜竇頂與額竇(t=5.131,P=0.001)、上頜竇底與額竇(t=5.874,P=0.000)、上頜竇頂與竇底(t=-2.892,P=0.018)黏膜可承受壓強間差異均有統計學意義(P<0.05)。
統計學分析結果可見,上頜竇黏膜可承受壓強-厚度之間相關性(r=0.976,P=0.000)以及額竇可承受壓強-厚度之間相關性(r=0.920,P=0.000)均較強;上頜竇、額竇可承受壓強-厚度的決定系數R2分別為0.953和0.847,說明上頜竇黏膜和額竇黏膜可承受壓強的差異中分別有95.3%和84.7%來源各自黏膜厚度的改變。
上頜竇、額竇黏膜可承受壓強-厚度直線回歸方程經方差分析后得到兩者F值分別為368.367和44.237,P值均為0.000,回歸方程均有統計學意義,可認為上頜竇和額竇黏膜可承受壓強與黏膜厚度之間有直線回歸關系,上頜竇黏膜可承受壓強-厚度回歸方程為y=-176.273+1.055x,額竇黏膜可承受壓強-厚度回歸方程為y=-14.520+0.628x。回歸方程散點圖見圖3、4。
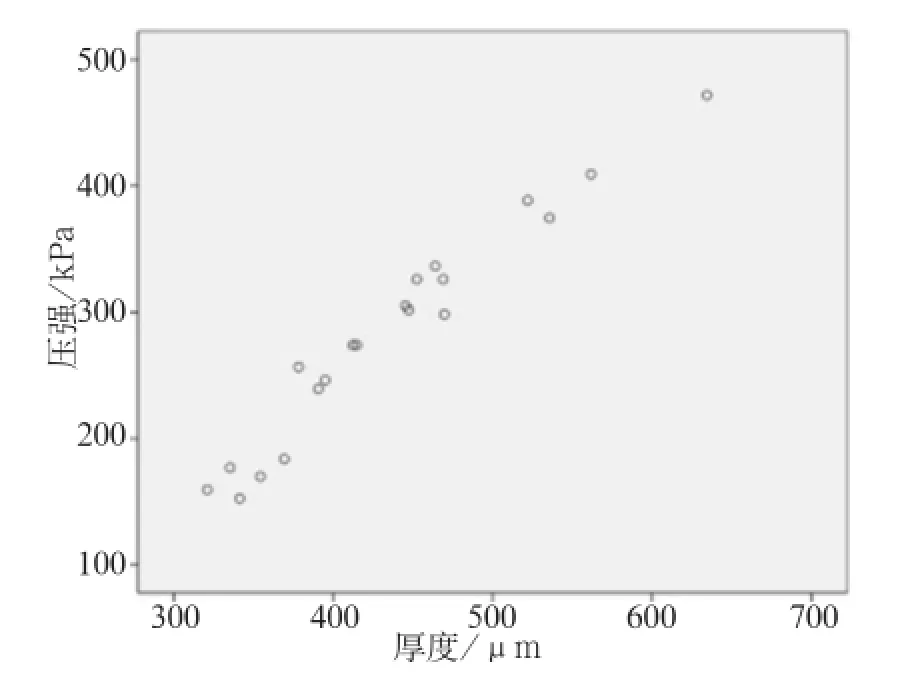
圖 3 上頜竇黏膜可承受壓強-厚度直線回歸關系散點圖Fig 3 The scatter chart of linear regression relation between the pressure and the membrane thickness in maxillary sinus membrane
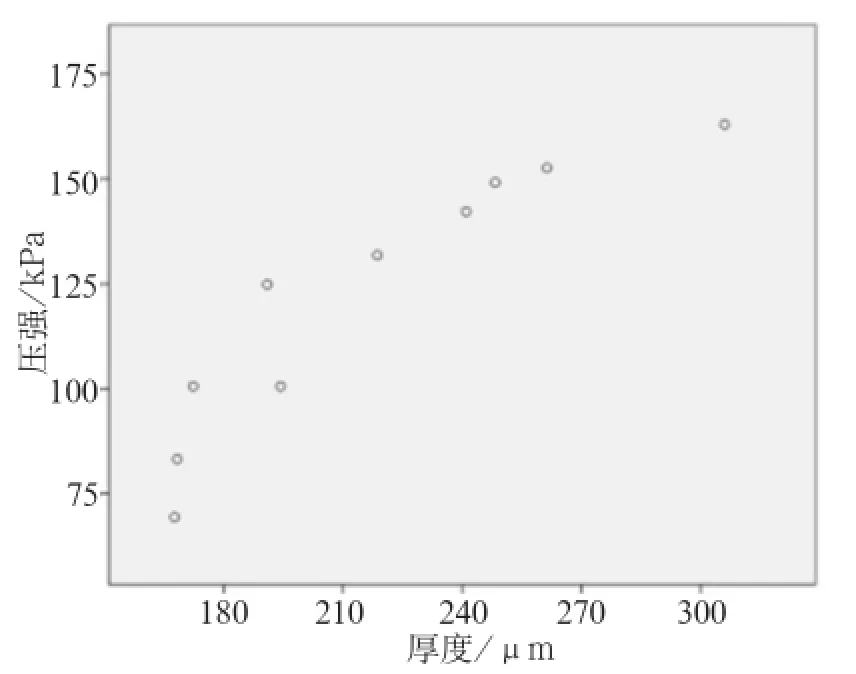
圖 4 額竇黏膜可承受壓強-厚度直線回歸關系散點圖Fig 4 The scatter chart of linear regression relation between the pressure and the membrane thickness in frontal sinus membrane
3 討論
3.1 實驗動物和取材部位的確定
關于實驗動物的選擇原則上應選擇與人類最為接近的靈長類動物如猴子,但考慮到價格和倫理問題并未選用。有學者[2]利用兔子和犬進行上頜竇實驗,但兔子和犬上頜竇小,相對不易操作。Haas等[3]認為犬沒有Schneiderian膜也不經歷氣化,但是有學者[4]卻不同意該觀點。豬上頜竇大小合適,但豬上頜竇外側壁較厚且皮質骨非常堅韌[5],并且上頜竇黏膜較人類厚[6]。山羊上頜竇位置、大小形態和骨結構與人類相似,外側壁骨板較薄,外科鉆鉆孔開窗以及黏膜的剝離和提升都較容易[7-8];尤其山羊竇腔黏膜厚度、組織結構也近似于人類[9-10],因此,本實驗研究選擇羊作為動物模型。
側壁開窗式上頜竇底提升術與沖頂式上頜竇底提升術均需剝離和抬高上頜竇底黏膜,本研究將每側上頜竇分割為頂、底兩部分,頂部選取兩側上頜竇外側壁靠近分割線部位黏膜,作為側壁開窗式上頜竇底提升術所需剝離的黏膜,底部選取接近后牙區根尖位置的黏膜,作為沖頂式上頜竇底提升術所需剝離的黏膜。選擇額竇黏膜,首先考慮作為上頜竇黏膜特性的對比研究,即使數值不作為上頜竇提升直接參考,但可更好了解上頜竇黏膜生物學特性并分析形成該特性的可能原因。
3.2 實驗技術關鍵點
實驗前行CT掃描和重建分析,旨在了解上頜竇和額竇的大小、上頜竇外側壁骨板厚度等,確定雙側上頜竇與參照物(牙膠條)間的位置關系以指導截骨;并且當出現上頜竇分嵴、黏膜轉折和變移時,在黏膜剝離等操作前給予提示和指導。
為保證實驗不受其他因素的干擾,每只羊處死后立即行CT掃描和后續實驗,頜骨鋸開后竇腔暴露于空氣中,為防止黏膜干燥引起性狀改變,應立即開始剝離黏膜,并將暫未行黏膜剝離的竇腔浸泡于室溫生理鹽水中,正進行剝離的黏膜和竇腔亦用生理鹽水不斷潤濕,并在保證操作質量前提下盡量縮短操作時間。為降低實驗結果的偶然誤差,保證實驗結果和最終數據的準確性,竇黏膜的剝離由一人完成。黏膜較薄,因此在任何操作步驟中均應輕柔仔細。
為使固定組織收縮率盡量降低,筆者參考大量文獻[11-12],最終選用10%中性甲醛溶液(即含磷酸鹽的緩沖液)作為黏膜固定液,最終測量得到羊上頜竇黏膜平均厚度,與以往文獻數據差異不大[9]。值得說明的是黏膜本身厚度極薄,相比較而言黏膜厚度值受標本制作過程中切片機切片方向的影響更值得考慮。因此切片機在切片時務必垂直于黏膜,待切片制作完成后檢查未達標準者(本實驗出現5例)返回重新制作切片。
盡管CT測量黏膜厚度的方法不存在黏膜浸于固定液中導致細胞微變形和切片機切片時的誤差,但是CT測量值單位通常為mm,光鏡讀數折算后單位為μm,二者相比數量級有差異,若以CT測量得到精確黏膜厚度較為困難。Janner等[13]曾運用錐形束CT在上頜竇不同位置測量黏膜厚度,但黏膜厚度有很大個體差異。故本實驗將CT測量黏膜厚度結果僅作為組織學輔助參考。
3.3 黏膜形態學表現
在剝離、切取黏膜和對黏膜垂直施壓時,即可直觀發現不同位置黏膜之間的差別:黏膜透明、纖薄時剝離容易發生卷曲和壓破,黏膜發白;厚重時剝離相對容易,不易壓破。隨推拉力計力值增大可見黏膜逐漸變薄和通透。但總體來說上頜竇黏膜韌性較大,上頜竇提升操作時若不以銳利器械施加過大的力作用于上頜竇黏膜,黏膜并不會輕易穿破,本實驗壓具底面直徑為6 mm,其推拉力計測定數值約為0.6~0.9 kg,最小值為上頜竇頂的0.44 kg,接近于500 mL瓶裝水重量,若臨床接觸黏膜的操作器械面直徑與本實驗不同,操作力值亦作相應調整。但本實驗為山羊竇黏膜,盡管山羊上頜竇情況與人類十分類似,但數值建議作為參考,完全以本數值為依據還需謹慎操作。
3.4 對結果的分析
針對山羊上頜竇頂、上頜竇底、額竇黏膜厚度均值大小不同,從上頜竇、額竇解剖方面分析,上頜竇與額竇黏膜厚度差別考慮可能原因:1)竇開口位置高低不同[14];2)神經支配不同。上頜竇底與上頜竇頂、額竇黏膜厚度差別可能原因是咀嚼力刺激大小不同。黏膜可承受壓強均值差異同樣提出前述猜想。但以上問題有待進一步驗證。
[參考文獻]
[1]樊佳東. 新型剝離器的優化和對羊上頜竇底黏膜剝離的對比研究[D]. 錦州: 遼寧醫學院研究生學院, 2014. Fan JD. A comparative study on the optimization of the new type of stripper and the dissection of the maxillary sinus floor in goat[D]. Jinzhou: Liaoning Medical University Postgraduate School, 2014.
[2]Allegrini S Jr, Yoshimoto M, Salles MB, et al. Bone regeneration in rabbit sinus lifting associated with bovine BMP[J]. J Biomed Mater Res Part B Appl Biomater, 2004, 68(2): 127-131.
[3]Haas R, Mailath G, D?rtbudak O, et al. Bovine hydroxyapatite for maxillary sinus augmentation: analysis of interfacial bond strength of dental implants using pull-out tests [J]. Clin Oral Implants Res, 1998, 9(2):117-122.
[4]李祥, 朱雙喜, 黃代營, 等. 上頜竇外提升及同期牙種植動物模型的建立[J]. 中國口腔種植學雜志, 2010, 15(4):165-167. Li X, Zhu SX, Huang DY, et al. An experimental model for maxillary sinus floor lift with simultaneous implant placement[J]. Chin J Oral Implantology, 2010, 15(4):165-167.
[5]Estaca E, Cabezas J, Usón J, et al. Maxillary sinus-floor elevation: an animal model[J]. Clin Oral Implants Res, 2008,19(10):1044-1048.
[6]Stelzle F, Benner KU. An animal model for sinus floor elevation with great elevation heights. Macroscopic, microscopic,radiological and micro-CT analysis: ex vivo[J]. Clin Oral Implants Res, 2010, 21(12):1370-1378.
[7]Derong Z, Lian G, Jiayu L, et al. Anatomic and histological analysis in a goat model used for maxillary sinus floor augmentation with simultaneous implant placement[J]. Clin Oral Implants Res, 2010, 21(1):65-70.
[8]Grageda E, Lozada JL, Boyne PJ, et al. Bone formation in the maxillary sinus by using platelet-rich plasma: an experimental study in sheep[J]. J Oral Implantol, 2005, 31(1):2-17.
[9]López-Ni?o J, García-Caballero L, González-Mosquera A,et al. Lamb ex vivo model for training in maxillary sinus floor elevation surgery: a comparative study with human standards[J]. J Periodontol, 2012, 83(3):354-361.
[10]肖菲, 趙保東, 王維英, 等. 用盤鉆經牙槽嵴提升上頜竇底手術的臨床效果觀察[J]. 中華口腔醫學雜志, 2011, 46 (6):321-325. Xiao F, Zhao BD, Wang WY, et al. Clinical study of transcrestal maxillary sinus floor elevation with the disk-up sinus reamer[J]. Chin J Stomatol, 2011, 46(6):321-325.
[11]Jonmarker S, Valdman A, Lindberg A, et al. Tissue shrinkage after fixation with formalin injection of prostatectomy specimens[J]. Virchows Arch, 2006, 449(3):297-301.
[12]顧挺, 張春葉, 王麗珍. 固定時間對口腔黏膜鱗狀細胞癌組織染色的影響[J]. 中國當代醫藥, 2013, 20(10):7-8, 11. Gu T, Zhang CY, Wang LZ. The effects of fixation time on the staining for oral squamous cell carcinoma(OSCC) tissues [J]. Chin Modern Med, 2013, 20(10):7-8, 11.
[13]Janner SF, Caversaccio MD, Dubach P, et al. Characteristics and dimensions of the Schneiderian membrane: a radiographic analysis using cone beam computed tomography in patients referred for dental implant surgery in the posterior maxilla[J]. Clin Oral Implants Res, 2011, 22(12):1446-1453.
[14]汪運坤, 林清霞, 張開文. 上頜竇竇口的應用解剖學觀測[J]. 耳鼻咽喉頭頸外科, 1999, 6(3):169-172. Wang YK, Lin QX, Zhang KW. Applied anatomy of the ostium of maxillary sinus[J]. Chin Arch Otolaryngology-Head Neck Surg, 1999, 6(3):169-172.
(本文編輯 杜冰)
[中圖分類號]R 782
[文獻標志碼]A [doi] 10.7518/hxkq.2016.01.012
[收稿日期]2015-07-08; [修回日期] 2015-11-07
[基金項目]解放軍總醫院臨床扶植基金(2014FC-SXYY-1003);首都衛生發展科研專項(首發2014-4-5022)
[作者簡介]呂源,住院醫師,碩士,E-mail:lvyuan586@163.com
[通信作者]李巖峰,副教授,博士,E-mail:m.god@yeah.net
Correlation studies in goats about the membrane thickness and pressure of the maxillary and frontal sinuses
Lü Yuan1,Han Yishi2, Li Yanfeng2, Ren Huan3, Fan Jiadong2, Liu Qian4, Hu Pin2, Bao Wenya2.
(1. Master’s Training Site, First Affliated Hospital of Peoples Liberation Army General Hospital, Liaoning Medical Universiy, Jinzhou 121000, China; 2. Dept. of Stomatology, The First Hospital Affiliated to The PLA General Hospital, Beijing 100048, China; 3. Clinic of Squadron 50 of Unit 78086, Chengdu 610017, China; 4. Dept. of Pathology, The First Hospital Affiliated to The PLA General Hospital, Beijing 100048, China)
Supported by: Clinial Support Fundation of The PLA General Hospital(2014FC-SXYY-1003); Special Project of Capital Health Development(2014-4-5022). Correspondence: Li Yanfeng, E-mail: m.god@yeah.net.
[Abstract]Objective This study aimed to explore the differences of membrane thickness and pressure on the paranasal sinus membrane in goats and analyze their causes. The results can provide theoretical basis and guidance for the issues of the maxillary sinus floor augmentation related to the membrane. Methods The membrane was cut into two sizes from every sinus membrane. The membrane was fixed in formalin to obtain tissue specimens for the membrane thickness study and pressure study. The correlation between the two parameters was then analyzed, and appropriate statistical methods and software were selected. Results The top of maxillary sinus, the bottom of maxillary sinus and the frontal sinus membrane thickness were (410.03±65.97), (461.33±91.37), (216.90±46.47) μm. The pressure were (260.08±80.12), (306.90±94.37),(121.72±31.72) kPa. The mean differences of the membrane thickness between the top of the maxillary sinus and the frontal sinus, bottom and frontal, and top and bottom were statistically significant (P<0.05). The mean differences in membrane pressure were also statistically significant (P<0.05). Conclusion The membrane thickness and pressure of the top and bottom of the maxillary sinus are higher than those of the frontal sinus membrane. However, the thickness and pressure of the bottom membrane are slightly higher than those of the top membrane. Pressure and membrane thickness are positively correlated in the sinus membrane.
[Key words]goat; maxillary sinus floor elevation; sinus membrane; membrane thickness; pressure