經皮冠狀動脈介入治療后雙聯抗血小板治療療程研究進展
2017-07-18 11:22:02趙靜
中國全科醫學 2017年21期
關鍵詞:支架
趙 靜
·新進展·
經皮冠狀動脈介入治療后雙聯抗血小板治療療程研究進展
趙 靜
經皮冠狀動脈介入治療后雙聯抗血小板治療可以有效預防心血管事件的發生風險,但是也會帶來出血風險。目前,其最優療程仍存在著較大爭議。近年來國際指南對該療程的推薦持續更新,從早期的“一概而論”到近期的多因素考慮。本文通過回顧近年來國內外相關指南,結合臨床試驗研究,分析討論雙聯抗血小板治療療程,指出應根據患者具體情況,如支架類型、基礎疾病、出血風險等,在權衡風險與獲益后,最終做到個體化、精準化治療。
急性冠狀動脈綜合征;藥物洗脫支架;經皮冠狀動脈介入;雙聯抗血小板;金屬裸支架
趙靜.經皮冠狀動脈介入治療后雙聯抗血小板治療療程研究進展[J].中國全科醫學,2017,20(21):2679-2682.[www.chinagp.net]
ZHAO J.Recent developments in duration of dual anti-platelet therapy after percutaneous coronary intervention[J].Chinese General Practice,2017,20(21):2679-2682.
急性冠脈綜合征(ACS)是指冠狀動脈下不穩定的粥樣硬化斑塊破裂或糜爛引起血栓形成所導致的心臟急性缺血綜合征[1]。對于合并ACS和藥物治療無效的穩定型心絞痛患者,經皮冠狀動脈介入治療(PCI)是臨床上一種有效的治療手段,但是由于支架的置入,可能會造成支架內血栓。為了預防支架內血栓的發生,目前臨床上多進行雙聯抗血小板治療(DAPT),常規給藥方案為阿司匹林+P2Y12受體抑制劑。但是DAPT在降低支架內血栓風險的同時也帶來了出血風險,而且若DAPT療程不足,已置入支架的患者支架內血栓發生風險更高[2],所以各國指南在DAPT療程方面均有嚴格推薦[3-16]。美國DAPT試驗顯示,對比DAPT療程12個月和30個月,30個月組支架內血栓、不良心腦血管事件、心肌梗死的發生率低于12個月組,但是中重度出血發生率高于后者,因此延長DAPT療程風險與收益并存[17]。如何平衡血栓和出血的風險,DAPT的療程多久最為適宜?這些問題被全球多國醫務工作者關注。本文針對DAPT療程的相關內容進行了匯總及分析,期望從中找出最優療程方案。
1 各國指南推薦療程
對于DAPT療程的長短,各國指南也不盡相同,詳見表1[1,3-16]。
2 DAPT療程的變遷
縱觀指南中的DAPT療程[1,3-16],發現近年來DAPT療程出現縮短趨勢,同時對患者的心臟疾病類型、置入支架類型、基礎疾病、危險分級也日趨細化,總體上進入了個體化給藥階段。目前針對DAPT療程的大規模數據試驗正在進行中[4]。
2.1 支架類型 早年PCI多用金屬裸支架(BMS),但是其發生血管再狹窄的風險高[18]。2002年上市的藥物洗脫支架(DES)由于置入了藥物,可降低血管再狹窄的風險[19]。第一代DES的支架材料為不銹鋼材質,所載的抗細胞增殖藥物為西羅莫司或紫杉醇,但是其支架內血栓風險高于BMS。第二代DES則以鈷鉻合金、鉑鉻合金為支架材料,同時其載藥種類也改進為依維莫司,并采用了新型親水性涂層,目的是減少支架局部炎性反應、降低再狹窄率和血栓風險。目前各國指南對于穩定性冠心病患者應用DES的DAPT療程推薦要長于BMS[3-4,7]。
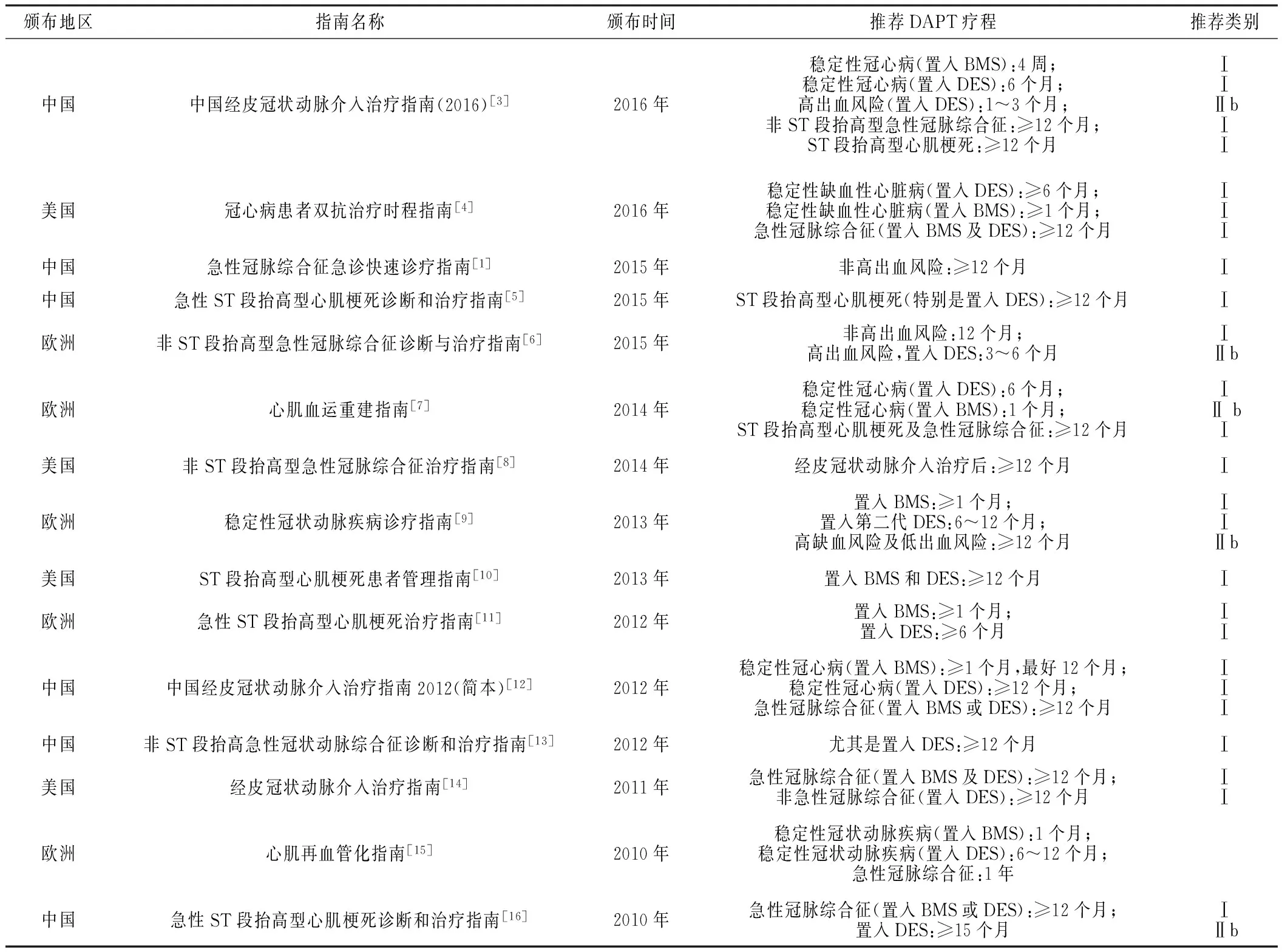
表1 各國指南中推薦的DAPT療程
注:DAPT=雙聯抗血小板治療,DES=藥物洗脫支架,BMS=金屬裸支架
但是有研究表明,對比置入第二代DES和BMS患者的支架內血栓發生率,前者優于后者[20]。THIM等[21]研究顯示,置入第一代DES患者DAPT過程中,對比停用氯吡格雷的療程,2個月組、3個月組、3~6個月組、6~12個月組不良心血管事件(心血管疾病導致的死亡、心肌梗死、支架內血栓)的發生率依次降低,但是3~6個月組與6~12個月組無顯著差異。GILARD等[22]研究顯示,對于置入第二代DES的患者,其DAPT療程6個月與24個月在死亡、心肌梗死、急診靶血管血運重建、卒中、嚴重出血復合終點事件發生率方面無顯著差異。上述研究表明,僅通過延長DAPT療程來降低不良心血管事件風險的考慮未必適宜。
2.2 基礎疾病 出血是長DAPT療程的最大風險,而避免DAPT患者合并出血的關鍵是預防,因此應早期進行臨床預后和出血風險的雙評估。最新美國《冠心病患者雙抗治療時程指南》推薦了DAPT評分表[4],將患者的年齡、既往病史、支架類型等方面進行了分值量化,認為≥2分的患者延長DAPT療程其收益大于風險;同時指南列出了增加缺血、支架內血栓(可考慮延長DAPT療程)、出血(可考慮縮短DAPT療程)風險的危險因素。可見,對于DAPT的給藥方案已經趨于個體化。
在基礎疾病方面,2011年美國《經皮冠狀動脈介入治療指南》[14]推薦既往上消化道出血病史的患者進行DAPT的同時預防性使用質子泵抑制劑(PPI)(推薦類別Ⅰ),上消化道出血高危患者(如高齡,合用華法林、甾體類抗炎藥、非甾體類抗炎藥,幽門螺桿菌感染)進行DAPT的同時長期應用PPI是有益的(推薦類別Ⅱa),但是反對對所有DAPT患者預防性使用PPI(推薦類別Ⅲ)。在合并糖尿病的患者中,對比置入DES患者的DAPT療程(6個月和12個月),12個月的患者可能獲益更大[23-24]。
糖尿病與血小板活化增加、血小板反應性和聚集增強有關,而這些均是血栓形成的危險因素。《中國經皮冠狀動脈介入治療指南(2016)》[3]對于特殊疾病患者的DAPT療程也進一步細化:合并糖尿病的患者,DAPT療程推薦≥12個月,且對于藥物的選擇也給予了明確推薦(阿司匹林+替格瑞洛);對于合并心房顫動的患者,根據非瓣膜病心房顫動患者的血栓栓塞危險評分系統(CHA2DS2-VAS)和房顫出血評分系統(HAS-BLED),推薦不同DAPT療程,HAS-BLED評分≤2分者推薦口服抗凝藥物+阿司匹林+氯吡格雷≥6個月(推薦類別Ⅱa),HAS-BLED評分≥3分者推薦口服抗凝藥物+阿司匹林+氯吡格雷至少1個月(推薦類別Ⅱa)。
中國《急性ST段抬高型心肌梗死診斷和治療指南》[16]和美國《經皮冠狀動脈介入治療指南》[14]中,早期對于穩定性冠心病患者PCI后的DAPT療程推薦與ACS并無差異,而近年來國際上對于穩定性冠心病患者的DAPT療程短于ACS的推薦日趨一致[3-4]。
3 小結及展望
通過對近年來國內外指南的回顧,不難看出,DAPT療程仍在優化過程中。指南中推薦的療程大多是來源于近年來DAPT臨床大規模數據試驗的結果,但是各國進行的DAPT試驗也存在著一定的局限性,如入組人群的選擇、樣本量的大小、支架類型不統一等,盡管如此,當前國際上對于DAPT療程的認識仍趨于一致[3,7],均是在綜合考慮患者的基礎疾病、置入支架的類型等因素,并在進行風險評估的基礎上推薦DAPT療程,摒棄一概而論,也不再一味地通過延長DAPT療程來達到降低支架內血栓風險的目的,而是權衡風險與獲益后確定該療程。精準化醫學體現在方方面面,隨著支架材質、藥物涂層的改進以及醫療技術的提升,相信DAPT將更加個體化治療。
本文無利益沖突。
[1]中國醫師協會急診醫師分會,中華醫學會心血管病學分會,中華醫學會檢驗醫學分會.急性冠脈綜合征急診快速診療指南[J].中華急診醫學雜志,2016,25(4):397-404.DOI:10.3760/cma.j.issn.1671-0282.2016.04.002. Emergency Medical Branch of Chinese Medical Doctor Association,Cardivascular Epidemiology Branch of Chinese Medical Association,Laboratory Medicine Branch of Chinese Medical Association.Emergency rapid diagnosis and treatment of guidelines acute coronary syndrome[J].Chin J Emerg Med,2016,25(4):397-404.DOI:10.3760/cma.j.issn.1671-0282.2016.04.002.
[2]GARG S,SERRUYS P W.Serruys,coronary stents:current status[J].J Am Coll Cardio1,2010,56(10 Suppl):S1-42.DOI:10.1016/j.jacc.2010.06.007.
[3]中華醫學會心血管病學分會介入心臟病學組,中國醫師協會心血管內科醫師分會血栓防治專業委員會,中華心血管病雜志編輯委員會.中國經皮冠狀動脈介入治療指南(2016)[J].中華心血管病雜志,2016,44(5):382-400.DOI:10.3760/cma.j.issn.0253-3758.2016.05.006. Section of Interventional Cardiology of Chinese Society of Cardiology of Chinese Medical Association,Specialty Committee on Prevention and Treatment of Thrombosis of Chinese College of Cardiovascular Physicians,Editorial Board of Chinese Journal of Cardiology.Chinese guideline for percutaneous coronary intervention(2016)[J].Chinese Journal of Cardiology,2016,44(5):382-400.DOI:10.3760/cma.j.issn.0253-3758.2016.05.006.
[4]LEVINE G N,BATES E R,BITTL J A,et al.2016 ACC/AHA guideline focused update on duration of dual antiplatelet therapy in patients with coronary artery disease:a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines[J].J Thorac Cardiovasc Surg,2016,152(5):1243-1275.DOI:10.1016/j.jtcvs.2016.07.044.
[5]中華醫學會心血管病學分會,中華心血管病雜志編輯委員會.急性ST段抬高型心肌梗死診斷和治療指南[J].中華心血管病雜志,2015,43(5):380-393.DOI:10.3760/cma.j.issn.0253-3758.2015.05.003. China Society of Cardiology of Chinese Medical Association,Editorial Board of Chinese Journal of Cardiology.Guideline on the diagnosis and therapy of ST-segment elevation myocardial infarction[J].Chinese Journal of Cardiology,2015,43(5):380-393.DOI:10.3760/cma.j.issn.0253-3758.2015.05.003.
[6]American College of Cardiology Foundation,American Heart Association Task Force on Practice Guidelines,Society for Cardiovascular Angiography and Interventions,et al.2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention:a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions[J].J Am Coll Cardiol,2011,58(24):E44-122.DOI:10.1016/j.jacc.2011.08.007.
[7]WINDECKER S,KOLH P,ALFONSO F,et al.2014 ESC/EACTS Guidelines on myocardial revascularization:the Task Force on Myocardial Revascularization of the European Society of Cardiology(ESC) and the European Association for Cardio-Thoracic Surgery(EACTS) developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions(EAPCI)[J].Eur Heart J,2014,35(37):2541-2619.DOI:10.1093/eurheartj/ehu278.
[8]AMSTERDAM E A,WENGER N K,BRINDIS R G,et al.2014 AHA/ACC Guideline for the Management of Patients with Non-ST-Elevation Acute Coronary Syndromes:a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines[J].J Am Coll Cardiol,2014,64(24):e139-228.DOI:10.1016/j.jacc.2014.09.017.
[9]Task Force Members,MONTALESCOT G,SECHTEM U,et al.2013 ESC guidelines on the management of stable coronary artery disease:the Task Force on the management of stable coronary artery disease of the European Society of Cardiology[J].Eur Heart J,2013,34(38):2949-3003.DOI:10.1093/eurheartj/eht296.[10]American College of Emergency Physicians,Society for Cardiovascular Angiography and Interventions,O′GARA P T,et al.2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction:a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines[J].J Am Coll Cardiol,2013,61(4):e78-140.DOI:10.1016/j.jacc.2012.11.019.
[11]Task Force on Myocardial Revascularization of the European Society of Cardiology(ESC) and the European Association for Cardio-Thoracic Surgery(EACTS),European Association for Percutaneous Cardiovascular Interventions(EAPCI),WIJNS W,et al.Guidelines on myocardial revascularization[J].Eur Heart J,2010,31(20):2501-2555.DOI:10.1093/eurheartj/ehq277.
[12]中華醫學會心血管病學分會介入心臟病學組,中華心血管病雜志編輯委員會.中國經皮冠狀動脈介入治療指南2012(簡本)[J].中華心血管病雜志,2012,40(4):271-277.DOI:10.3760/cma.j.issn.0253-3758.2012.04.003. Section of Interventional Cardiology,Chinese Society of Cardiology of Chinese Medical Association,Editorial Board of Chinese Journal of Cardiology.Chinese guideline for percutaneous coronary intervention 2012(pocket guideline)[J].Chinese Journal of Cardiology,2012,40(4):271-277.DOI:10.3760/cma.j.issn.0253-3758.2012.04.003.
[13]中華醫學會心血管病學分會,中華心血管病雜志編輯委員會.非ST段抬高急性冠狀動脈綜合征診斷和治療指南[J].中華心血管病雜志,2012,40(5):353-367.DOI:10.3760/cma.j.issn.0253-3758.2012.05.001. Chinese Society of Cardiology of Chinese Medical Association,Editorial Board of Chinese Journal of Cardiology.Guideline of non-ST segment elevation acute coronary syndrome[J].Chinese Journal of Cardiology,2012,40(5):353-367.DOI:10.3760/cma.j.issn.0253-3758.2012.05.001.
[14]ROFFI M,PATRONO C,COLLET J P,et al.2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation:Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology(ESC)[J].Eur Heart J,2016,37(3):267-315.DOI:10.1093/eurheartj/ehv320.
[15]Task Force on the management of ST-segment elevation acute myocardial infarction of the European Society of Cardiology(ESC),STEG P G,JAMES S K,et al.ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevataion[J].Eur Heart J,2012,33(20):2569-2619.DOI:10.1093/eurheartj/ehs215.
[16]中華醫學會心血管病學分會,中華心血管病雜志編輯委員會.急性ST段抬高型心肌梗死診斷和治療指南[J].中華心血管病雜志,2010,38(8):675-690.DOI:10.3760/cma.j.issn.0253-3758.2010.08.002. China Society of Cardiology of Chinese Medical Association,Editorial Board of Chinese Journal of Cardiology.Guideline for diagnosis and treatment of patients with ST-elevation myocardial infarction[J].Chinese Journal of Cardiology,2010,38(8):675-690.DOI:10.3760/cma.j.issn.0253-3758.2010.08.002.
[17]MAURI L,KEREIAKES D J,YEH R W,et al.Twelve or 30 months of dual antiplatelet therapy after drug-eluting stents[J].N Engl J Med,2014,371(23):2155-2166.DOI:10.1056/NEJMoa1409312.
[18]SERRUYS P W,STRAUSS B H,BEATT K J,et al.Angiographic follow-up after placement of a self-expanding coronary-artery stent[J].N Engl J Med,1991,324:13-17.DOI:10.1056/NEJM199101033240103.
[19]LAGERQVIST B,JAMES S K,STENESTRAND U,et al.Long-term outcomes with drug-eluting stents versus bare-metal stents in Sweden[J].N Engl J Med,2007,356(10):1009-1019.DOI:10.1056/NEJMoa067722.
[20]PALMERINI T,BIONDI-ZOCCAI G,DELLA RIVA D,et al.Stent thrombosis with drug-eluting and bare-metal stents:evidence from a comprehensive network meta-analysis[J].Lancet,2012,379(9824):1393-1402.DOI:10.1016/S0140-6736(12)60324-9.
[21]THIM T,JOHANSEN M B,CHISHOLM G E,et al.Clopidogrel discontinuation within the first year after coronary drug-eluting stent implantation:an observational study[J].BMC Cardiovasc Disord,2014,14:100.DOI:10.1186/1471-2261-14-100.
[22]GILARD M,BARRAGAN P,NORYANI A A L,et al.6- versus 24-month dual antiplatelet therapy after implantation of drug-eluting stents in patients nonresistant to aspirin:the randomized,multicenter ITALIC trial[J].J Am Coll Cardiol,2015,65(8):777-786.DOI:org/10.1016/j.jacc.2014.11.008.
[23]GWON H C,HAHN J Y,PARK K W,et al.Six-month versus 12-month dual antiplatelet herapy after implantation of drug-eluting stents:the Efficacy of Xience/Promus Versus Cypher to Reduce Late Loss After Stenting(EXCELLENT) randmized,multicenter study[J].Circulation,2012,125(3):505-513.DOI:10.1161/CIRCULATIONAHA.111.059022.
[24]王斌,高矩.經皮冠狀動脈介入術后雙聯抗血小板治療,縮短還是延長?[J].中國全科醫學,2015, 18(23) :2751-2753,2757.DOI:10.3969/j.issn.1007-9572.2015.23.001. WANG B,GAO J.Dual anti-platelet therapy after percutaneous coronary intervention:should it be shortened or prolonged? [J].Chinese General Practice, 2015, 18(23) :2751-2753,2757.DOI:10.3969/j.issn.1007-9572.2015.23.001.
(本文編輯:崔麗紅)
Recent Developments in Duration of Dual Anti-platelet Therapy after Percutaneous Coronary Intervention
ZHAOJing
DepartmentofPharmacology,TianjinBinhaiNewAreaofTraditionalChineseMedicineHospital,Tianjin300450,China
Dual anti-platelet therapy(DAPT) after percutaneous coronary intervention can be effective in preventing the risk of cardiovascular events,but it also brings the risk of bleeding.At present,the argument of the optimal duration is still controversial.In recent years,the international guidelines recommend continuous updates to the therapy duration,from "one kind of DAPT duration fits all" to multi-factor-based DAPT duration.Based on reviewing the guidelines and the clinical trials associated with DAPT duration at home and abroad,we analyzed and discussed the DAPT duration,and concluded that,it should be vary by the patients′ own special conditions,such as type of stent placed,underlying disease and risk of bleeding,and after balancing the risks and benefits,in order to achieve the effect of personalized and accurate treatment.
Acute coronary syndrome;Drug-eluting stents;Percutaneous coronary intervention;Dual anti-platelet therapy;Bare-metal stents
R 542.2
A
10.3969/j.issn.1007-9572.2017.21.024
2017-02-14;
2017-06-01)
300450 天津市濱海新區中醫醫院藥學科
猜你喜歡
保健醫苑(2022年5期)2022-06-10 07:46:12
小哥白尼(趣味科學)(2021年8期)2021-11-20 06:08:04
海洋信息技術與應用(2020年3期)2020-08-24 07:25:10
中國臨床醫學影像雜志(2019年5期)2019-08-27 02:48:00
中國生物醫學工程學報(2019年4期)2019-07-16 08:04:16
模具制造(2019年3期)2019-06-06 02:10:54
制造業自動化(2017年2期)2017-03-20 14:26:14
中國繼續醫學教育(2015年6期)2016-01-07 07:38:49
沈陽醫學院學報(2014年4期)2014-12-27 13:44:20
航天器工程(2014年5期)2014-03-11 16:35:55
