Ischemic stroke due to carbon monoxide intoxication:Two case reports
2018-03-17 01:58:13AtifBayramogluAbdullahOsmanKocakEsraKadioglu
Atif Bayramoglu, Abdullah Osman Kocak, Esra Kadioglu
Department of Emergency Medicine, Faculty of Medicine, University of Ataturk, Erzurum, Turkey
Dear editor,
Following its entrance into the human body through inhalation, carbon monoxide (CO) forms carboxyhemoglobin (COHb) by binding to hemoglobin(Hb) within the blood. Massive ischemic tissue necrosis occurs in 0.5%–1% of cases with CO poisoning.[1]The affinity of CO to Hb is 200–250 times more when compared to the affinity of oxygen. As a result of CO binding to Hb, oxygen delivery to the tissues is reduced,and tissue hypoxia develops. This affects mostly the brain and heart, which are the organs with the highest demand for oxygen. Hypoxia leads to oxidative stress,cellular necrosis, apoptosis, and inflammation in acute CO poisoning. Pathological changes in the brain observed in CO poisoning are hippocampal necrosis,demyelination of the cerebral white matter, and spongy necrosis of the globus pallidus and cerebral cortex.[2]
In this report, we aim to present our two cases where ischemic stroke developed following CO poisoning.
CASE 1
Our first case was a 29-year-old male patient. He was transferred to our emergency service for hyperbaric oxygen therapy from another center with the diagnosis of CO poisoning. Information obtained from the patient’s relatives revealed that three of six people living in the same house had died due to stove-poisoning. Our patient had cerebral palsy disorder, and hence he was bedridden and unable to speak. His vital signs were stable. His COHb value was 21% at the previous center. His biochemical test results revealed CK 563 U/L (1–171)and Troponin I 0.5 ng/mL (<0.04). His ECG showed a normal sinus rhythm. Since he had cerebral palsy, it was not possible to perform a neurological examination. His computerized cranial tomography revealed a hypodense area with irregular boundaries adjacent to the posterior horn of the left lateral ventricle (Figure 1A). Thereupon,diffusion-weighted MRI (DWI) was obtained for differential diagnosis. It revealed limitation of diffusion,hyperintense at B100 and hypointense at ADC, at the left occipitoparietal region, and with the gyral location, which was consistent with acute ischemia (Figure 1B). The patient underwent hyperbaric oxygen therapy for a total of five days. Continuous nasal oxygen and fluid support were administered. For ischemic infarct, in addition to his current treatment, single-dose oral aspirin 100 mg per day and subcutaneous clexane, 0.6 mL twice a day,were administered. Following cessation of his hyperbaric oxygen therapy and with no new disorder occurring during follow-up, he was discharged with full recovery.
CASE 2
A 22-year-old female patient was transferred to our emergency department in need of intensive care and hyperbaric oxygen therapy. During admission, her general status was poor, Glasgow Coma Score was 3, and she was intubated. Her medical history, obtained from her relatives, revealed that she had undergone aortic valve replacement six years ago, was using coumadin, and had no additional disorders. Her vital signs during admission were as follows: blood pressure 98/52 mmHg, pulse 108/minute, SpO293%. Her breath sounds were coarse bilaterally. There was an incision scar, approximately 10 cm in length, located at the anterior thoracic wall, probably secondary to her previous surgery. Her COHb was 45% at the previous center. Laboratory results at our hospital were as follows: CK 3,102 U/L (5–140), CKMB 492 U/L (1–24), ALT 46 U/L (1–50), AST 249 U/L (1–50), ALP 370 U/L (30–120); Troponin I 21.61 ng/mL (<0.04). Her ECG revealed sinus tachycardia (108/minute). Her PA chest X-ray revealed bilateral diffuse infiltrations together with findings of aspiration. Her echocardiography findings were normal. A cranial CT was obtained, which showed a suspicious hypodense area in the frontal region (Figure 2A). The presence of ischemic area was confirmed when an image consistent with acute-subacute phase infarct area was observed at the frontoparietal region in DWI obtained seven days later (Figure 2B). The patient was hospitalized in Intensive Care Unit, with the management plan of hyperbaric oxygen treatment for 10 days. On the sixth day, she was extubated. Following extubation,paresis of left upper and lower extremities, and facial paralysis was discovered, together with gait disturbance and speech disorder. During this period, in addition to hyperbaric oxygen therapy, 100 mg oral aspirin was administered as an antiaggregant, with low-molecular weight heparin (clexane 0.6 mL) subcutaneously.Following treatment, the patient was discharged with regression of all symptoms except facial paralysis.
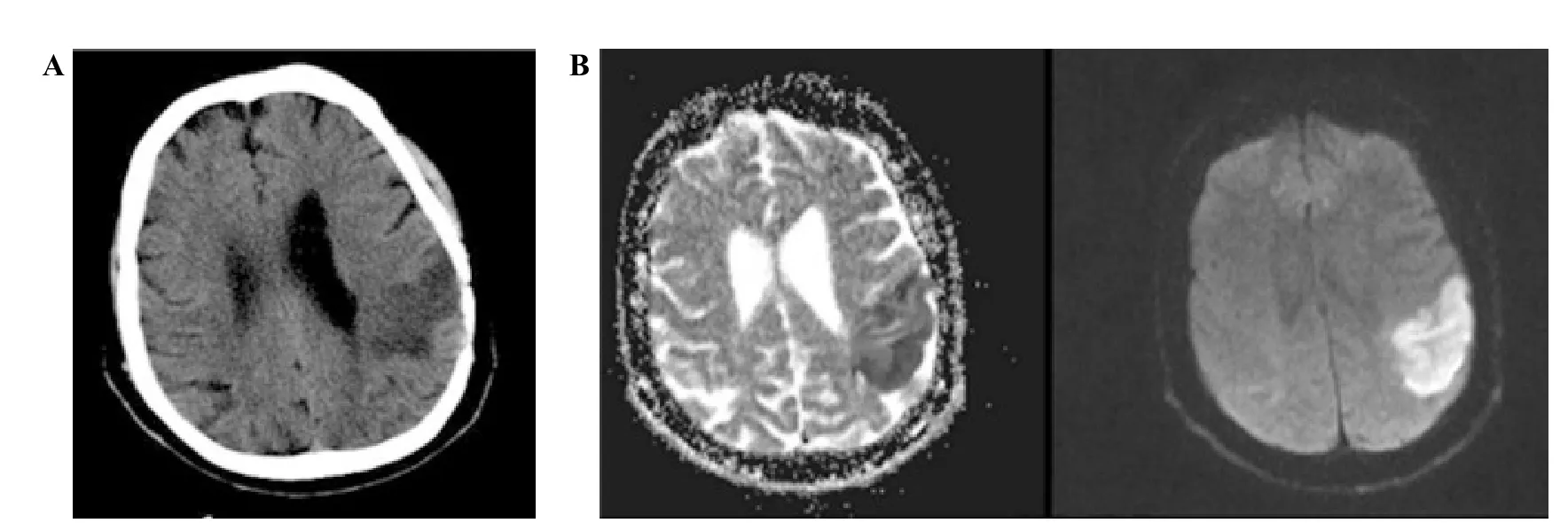
Figure 1. Results of computerized cranial tomography and diffusion-weighted MRI in case 1. A: His computerized cranial tomography revealed a hypodense area with irregular boundaries adjacent to the posterior horn of the left lateral ventricle; B: DWI revealed limitation of diffusion at the left occipitoparietal region and with gyral location, which was consistent with acute ischemia.
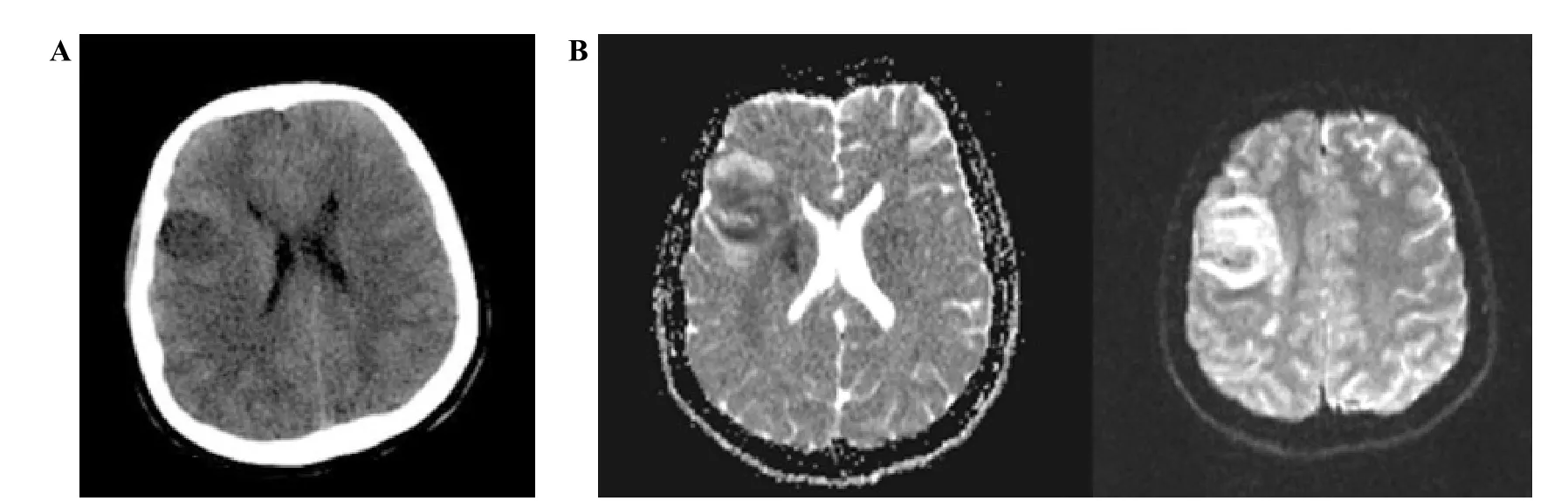
Figure 2. Results of computerized cranial tomography and diffusion-weighted MRI in case 2. A: Her cranial tomography showed hypodense area at the frontal region; B: DWI showed acute-subacute phase infarct area at the frontoparietal region.
DISCUSSION
Thromboembolic events related to CO intoxication are rare, and ischemic stroke is even rarer.[3]We have contributed to this sporadic clinical condition with two cases. In patients admitted with CO poisoning, a neurological examination may not be possible due to causes such as cerebral palsy and unconsciousness.
Our aim in presenting these cases was to give a reminder that ischemic stroke may develop due to CO intoxication and to avoid skipping its diagnosis. In patients with CO intoxication, the cranial CT findings may be normal during the acute phase, and the ischemic area may not be demonstrated.[4]Therefore, in patients with CO intoxication who cannot be evaluated by neurological examination, ischemic stroke related to CO intoxication should be kept in mind, and further investigations should be made. In this way, diagnosis can be made and treatment can be initiated earlier.
The release of nitric oxide (NO) related to the effect of CO gas on platelets takes place on the basis of thromboembolic events.[5]NO inhibits mitochondrial enzymes such as aconitase, NADPH, oxidoreductase,and succinate oxidoreductase that contain iron and are necessary for cell survival, impairing cellular functions.[6]Production of free oxygen radicals is increased together with their concentration in the blood. Free oxygen radicals may cause oxidative stress and lead to endothelial damage and stenosis of the arteries by affecting platelet aggregation and blood flow. Free oxygen radicals have been known to impair hemostasis. Additionally, they increase thrombus formation by affecting vascular tone and platelet functions.[5]
Atrial fibrillation (AF) is the most common cardiac arrhythmia in the world and is an independent risk factor for stroke.[7]However, since our cases had normal sinus rhythm in their ECGs, we considered that the clinical findings were manifested not because of an embolic event due to AF but due to the mechanism mentioned above, which was created by CO.
CO gas is a substance which can damage the vascular structures directly. In CO intoxication, focal intimal degeneration, cellular hypertrophy, detachment of the subintimal structures, and endothelial edema were demonstrated in mice. People who had COHb levels of 5% and higher have been found to have a 21-fold increase in the risk for atherosclerotic disorders.Atherosclerotic disorders have also been known to be an important factor in the formation of arterial and venous thromboses.[1]
In CO intoxication, cerebral lesions may also occur related to global hypoxia. In such cases, lesions are symmetrical. They usually manifest in the basal ganglia and central gray and white matter, which are regions with high oxygen demand.[8]In our cases, ischemic stroke,which developed unilaterally, affected the frontoparietal and occipitoparietal lobes. For this reason, we considered that ischemic stroke was not related to global hypoxia in our cases.
In CO poisoning, CT may skip the diagnosis of petechial bleeding in the brain. CT can demonstrate only the edema formed around the petechial bleeding. MRI is superior in detecting the presence of extravasated blood.[8]MRI has a high degree of sensitivity in showing the cerebral abnormalities related to CO poisoning, and the alterations can be discovered even at the first hour following exposure.[9]
The major difference between our first case and other cases with ischemic stroke following CO poisoning[3,9,10]is performing DWI in the early period. With DWI in the early period, ischemic stroke was diagnosed without delay, which may have been delayed otherwise.
CONCLUSION
In patients with carbon monoxide poisoning who are admitted in an unconscious state, ischemic stroke can be diagnosed in the early period by performing DWI, even if the cranial CT revealed normal results.Early implementation of thrombolytic treatment due to early diagnosis can have a positive impact on prognosis,reducing mortality and morbidity rates.
Funding:None.
Ethical approval:Not needed.
Conflicts of interest:The authors declare that there are no conflicts of interest relevant to the content of the article.
Contributors:AB proposed the study and wrote the first draft. All authors read and approved the final version of the paper.
1 Sevinc A, Savli H, Atmaca H. An interesting cause of pulmonary emboli: acute carbon monoxide poisoning. Clin Appl Thromb Hemost. 2005;11(3):353-7.
2 Beppu T. The role of MR imaging in assessment of brain damage from carbon monoxide poisoning: a review of the literature. AJNR Am J Neuroradiol. 2014;35(4):625-31.
3 Teodoro T, Geraldes R, Pinho e Melo T. Symptomatic internal carotid artery thrombosis in acute carbon monoxide intoxication. Am J Emerg Med. 2014;32(6):684 e5-6.
4 Moulin T, Cattin F, Crépin-Leblond T, Tatu L, Chavot D,Piotin M, et al. Early CT signs in acute middle cerebral artery infarction: predictive value for subsequent infarct locations and outcome. Neurology. 1996;47(2):366-75.
5 Yildirim C, Günay N, Büyükaslan H, Kü?ükdurmaz Z, Bozkurt S. A case of carbon monoxide poisoning with thrombus in the heart: a case report. Inhal Toxicol. 2005;17(14):797-801.
6 Marín J, Rodríguez-Martínez MA. Role of vascular nitric oxide in physiological and pathological conditions. Pharmacol Ther.1997;75(2):111-34.
7 Ment J. Direct oral anticoagulants: key considerations for use to prevent stroke in patients with nonvalvular atrial fibrillation.Vasc Health Risk Manag. 2015;11:317-32.
8 El Khashab M, Nejat F. Hemorrhagic cerebral infarction in carbon monoxide poisoning: a case report. Cases J. 2009;2:96.
9 Ahmad A, Sharma VK. Early subcortical ischemic infarction and delayed leucoencephalopathy after carbon monoxide poisoning. Intern Emerg Med. 2012;7 Suppl 1:S33-4.
10 Kara H, Bayir A, Ak A, Degirmenci S. Cerebrovascular ischaemia after carbon monoxide intoxication. Singapore Med J. 2015;56(2):e26-8.
 World journal of emergency medicine2018年1期
World journal of emergency medicine2018年1期
- World journal of emergency medicine的其它文章
- Understanding the effect of propofol and electrical cardioversion on the systolic blood pressure of emergency department patients with atrial fibrillation
- Perimortem caesarean section: A case report of an out-of-hospital arrest pregnant woman
- Drug calculation ability of qualified paramedics:A pilot study
- A Lazarus effect: A case report of Bupropion overdose mimicking brain death
- First-in-man implantation of the retrievable and repositionable VenusA-Plus valve
- Dose-related effects of dexmedetomidine on immunomodulation and mortality to septic shock in rats