Ablation of atrial fibrillation-patient selection,periprocedural anticoagulation,techniques,and preventive measures after ablation
2019-02-18 08:20:42童鴻
心電與循環(huán)
2019年1期
關(guān)鍵詞:手術(shù)
Patient Selection
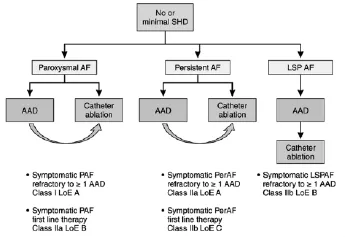
Figure 1 Selection of patients with no or minimal structural heart disease for atrial fibrillation(AF) ablation.AAD indicates antiarrhythmic drug;LoE,Level of Evidence;LSPAF,long-standing persistent atrial fibrillation;PAF,paroxysmal atrial fibrillation;and PerAF,persistent atrial fibrillation.
Patient selection for ablation is a shared decision by the patient and physician.The odds of a successful ablation not only are related to the technique of the procedure but also are critically to patient characteristics.The ideal patient with the highest likelihood of procedural success is one with paroxysmal AF,no underlying cardiac disease,and a nondilated left atrium(Figure 1).Paroxysmal AF is defined as AF <7 days in duration.Success rates with these patients approaches 80%.However,it has become clear in the last decade that even patients with persistent(>7 days)and long-standing persistent(continuous AF >1 year)AF may also benefit from AF ablation.In addition,patients with congestive heart failure or decreased left ventricular ejection fraction may be candidates for AF ablation(Figure 2).However,it is clear that the odds of a successful ablation are diminished with greater underlying heart disease.In particular,left atrial enlargement,mitral valve disease,and chronic heart failure are associated with poorer outcomes.It was once believed thatpatients need to failatleast1 antiarrhythmic agent before AF ablation.However,given the known toxicities of antiarrhythmic agents and the success of ablation,ablation is now acceptable as an initial rhythm control strategy,at least for paroxysmal AF.

Figure 2 Selection of patients with structural heart disease(SHD)for atrial fibrillation (AF)ablation.AAD indicates antiarrhythmic drug.
The latest AF ablation guidelines were updated in the United States in 2014 and in Europe in 2012(Table 1).For patients with symptomatic paroxysmal AF,the latest American Heart Association/American College of Cardiology recommendations give a ClassⅠrecommendation (is useful)for catheter ablation in patients with paroxysmal AF who have failed or are intolerant of classⅠorⅢantiarrhythmic agents.These same guidelines give a IIa recommendation(is reasonable)for those symptomatic patients with paroxysmal AF who wish to pursue ablation as an initial rhythm strategy and patients with symptomatic persistent AF who have failed or are intolerant to a classⅠorⅢantiarrhythmic agent.

Table 1 P atient Selection for AF Ablation According to US and European Guidelines
Repeat ablations are necessary in many patients,particularly in those with underlying heart disease.In general,a younger age,greater severity of symptoms,and contribution of AF to heart failure/cardiomyopathy factor into1the decision for repeat ablations.In many of these individuals,repeat ablations should be performed.
Anticoagulation
The vitamin K antagonist warfarin has been the gold standard for anticoagulation in AF.Its ability to lower the risk of thromboembolism has been established by large randomized,controlled trials (RCTs) in the 1980s and early 1990s.However,warfarin therapy is complicated bytheneed fordietarycompliance,sensitivity to multiple medications,frequent blood draws for monitoring, and often unexplained INR(international normalized ratio) fluctuations.Thus,there has been a widespread desire to develop warfarin substitutes that are safer and easier to administer.
Dabigatran,a direct thrombin inhibitor,and the direct factor Xa inhibitors rivaroxaban,apixaban,and edoxaban are currently available. All of these newer/direct anticoagulants were tested against warfarin;they have not been directly compared with one another in a clinical trial.Although the clinical results of the trials are similar,there are differences in trial design,patient thromboembolic risk,and end points that prevent their direct comparison.
The CHA2DS2-VASc score has largely supplanted the CHADS score for the estimation of stroke risk in patients with AF.The CHA2DS2-VASc score includes 7 clinical characteristics (congestive heart failure,hypertension,age,diabetes mellitus,stroke/transient ischemic attack,vascular disease,female sex)to stratify stroke risk.In the US guidelines,individuals with a CHA2DS2-VASc score of≥2 are recommended to undergo anticoagulation.ESC guidelines recommend anticoagulation for those with a CHA2DS2-VASc score of≥1(IIa;should be considered for those with a score of 1).The data on the risk of stroke in individuals with AF with a CHA2DS2-VASc score of 1 are conflicting and thus underlie the different recommendations in the United States and Europe.
Periprocedural prescription of anticoagulation is evolving.Initially,warfarin was held either with or without heparin bridging.Subsequent data emerged that showed that bleeding complications were actually lower with uninterrupted warfarin compared with a bridging strategy.In addition,uninterrupted strategies reduce both clinical and silent thromboembolic events.This pattern of withholding anticoagulation around the time of the ablation also applied to the direct anticoagulants,with some studies advocating bridging and others not.There is more concern about the treatment of bleeding complications with the direct anticoagulants because of the previous lack of reversal agents.Registry data have suggested that ablation can be performed without discontinuation of these agents,although often 1 or 2 doses are held before the procedure.In addition,the developmentofreversalagents forthese direct anticoagulants should provide more justification for uninterrupted anticoagulation at the time of the ablation.Continuation of anticoagulants should persist for at least 2 months after the procedure.Continuing anticoagulation for an extended time period depends on the CHA2DS2-VASc score.The 2012 ESC guidelines state that long-term anticoagulation is recommended in all patients with a CHA2DS2-VASc score of≥2,and the US guidelines agree that the decision for continued anticoagulation largely hinges on the CHA2DS2-VASc score.In the US guidelines,individuals with a low CHA2DS2-VASc score and successful ablation can likely stop anticoagulation after 2 to 3 months.Current guidelines do not recommend AF ablation for the sole purpose of discontinuation of anticoagulation.
Techniques
Techniques for AF ablation are maturing,and differences are not completely resolved.Techniques for the ablation of AF vary by energy source and location of atrial lesions(ie,lesion sets).
Energy sources available for AF ablation include radiofrequency,cryoablation,and laser.Radiofrequency and cryoablation are currently most commonly used.Radiofrequency creates a lesion with heat(typically up to 60℃)and can be delivered with or without saline irrigation at the tip of the catheter.Irrigated-tip catheters reduce the risk of char formation and improve lesion depth and size;in general,they are the most commonly used catheters for radiofrequency ablation.New catheters with the ability to quantify the force of contact have recently been developed and appear to give more consistent lesions than prior catheters.Cryoablation is administered via a left atrial balloon that occludes each PV individually and freezes to-50℃.Laser ablation is performed with special catheters designed to create a circumferential lesion set around each PV.
The location of ablation lesions is where the major controversies in AF ablation lie.It is reasonably acknowledged that for individuals with paroxysmal AF and no underlying heart failure,electric isolation of the PVs at the antral level is associated with a high degree of elimination of AF.This isolation can be accomplished with radiofrequency,cryoablation,or laser energy.Randomized,clinical trials in this patient population generally compare an ablative technique with antiarrhythmic drug therapy.
Whether one ablative technique to isolate the PVs is superior to the other is not clear.Limited registry data have compared radiofrequency with cryoablation.In the German Ablation Registry,the recurrence rate at 1 year after a single procedure was≈45%in both groups.There have now been 2 RCTs comparing radiofrequency and cryoablation.In FREEZE AF,the reported success rates in the radiofrequency and cryoablation groups were comparable at 1-year follow up(63.1%versus 64.1%after a single procedure and 70.7%versus 73.6%after multiple procedures in the radiofrequency and cryoablation group,respectively).In the recently published FIRE AND ICE (Cryoablation or Radiofrequency Ablation for Paroxysmal Atrial Fibrillation)trial comparing radiofrequency and cryoablation in 762 patients with paroxysmal AF,the 1-year recurrences were 35.9% and 34.6% ,respectively.
In patients with nonparoxysmal AF,there is currently no one clearly preferred approach.In these individuals,isolation of the PVs alone may not be adequate to prevent recurrences.These additional lesion sets can be anatomically based or electrically guided.Anatomic guidance creates ablation lines in particular locations.The most common location is the roof between the right and left superior PVs (roof line).Additional lines can be placed between the left and right inferior veins,left inferior PV,and mitral annulus(mitral line).A cavotricuspid right-sided isthmus line may also be placed.However,reports from RCTs documenting outcomesofadditionallinearlesionshave been contradictory.Some RCTs have demonstrated benefits of adjunctive linear lesions in increasing arrhythmia-free survival rates in patients with nonparoxysmal AF undergoing PV isolation.In contrast,other RCTs have reported no additional advantages of a linear ablation approach over PV isolation alone in patients with AF,and the lines required significantly more ablation time,higher radiation doses,and longer procedure durations.
Electric lesion sets can be guided electrically by complex fractionated electric potentials or focal/reentrant sources(also described as rotors or drivers).Complex fractionated electric potentials can be identified by individual operators or by special software analysis programs available in some commercial mapping systems.Focal/reentrant sources are currently mapped by an endocardial basket and specialized software FIRM(Focal Impulse and Rotor Mapping)or by surface mapping(Figure 6).FIRM-guided ablation of persistent AF has shown higher 3-year freedom from AF compared with conventional ablation(single-procedure freedom from AF at 890 days,75%versus 30%).
Relatively common periprocedural complications include groin hematomas,pericardial chest pain,and atrial irritability with atrial premature contractions and AF.Less common but more severe complications include cardiac perforation and tamponade(≈1%),stroke or transient ischemic attack(≈1%),vascular aneurysms or fistulas(≈1%),PV stenosis(common previously but rare currently),and phrenic nerve paralysis, particularly with cryoablation. Rare complications include mitral valve injury,myocardial infarction,air embolism,radiation injury,atrial esophageal fistula,gastric motility disorders,and death.
詞 匯
odds n.機(jī)會(huì)、機(jī)運(yùn)
candidates n.候選人、應(yīng)試者、考生
pursue v.追趕、追求、追隨、繼續(xù)
compliance n.順從、遵從、依從
fluctuation n.波動(dòng),起伏
substitute n.&v.&adj.替代物,替代者;替代,取代,接替;替代的,臨時(shí)的
prescription n.&adj.規(guī)定,處方,書面醫(yī)囑;憑處方供應(yīng)的
cryoablation n.冷凍消融
char n.&v.炭,燒焦物;燒成炭,打雜,做
antral adj.竇的,前庭的
rotor n.轉(zhuǎn)子,旋筒,旋翼
motility n.能動(dòng)
注 釋
1.factor into指“成為(影響)…的”因素,factor可作為動(dòng)詞使用,但以這種主動(dòng)形式出現(xiàn)的很少見,通常以“be factored into”形式出現(xiàn),如The comsumer's viewpoint should be factored into decision making.消費(fèi)者的觀點(diǎn)應(yīng)作為決策因素計(jì)入。
參考譯文
第87課 心房顫動(dòng)消融-患者選擇、圍手術(shù)期抗凝、技術(shù)及術(shù)后預(yù)防措施
患者選擇
患者消融的選擇由患者與醫(yī)師共同決策。成功消融的概率不但與手術(shù)技術(shù)有關(guān),也與患者的特征明顯相關(guān)。手術(shù)成功率最高的理想患者是陣發(fā)性心房顫動(dòng),無基礎(chǔ)心臟疾病和左心房擴(kuò)大(見圖1)。陣發(fā)性心房顫動(dòng)的定義是病程<7d。這類患者的成功率達(dá)80%。不過,最近10年已明確即使持續(xù)性心房顫動(dòng)(>7 d)和慢性心房顫動(dòng)也可從心房顫動(dòng)的消融中獲益。另外,充血性心力衰竭或射血分?jǐn)?shù)下降的患者也可選心房顫動(dòng)消融(見圖2)。但是,基礎(chǔ)心臟疾病較明顯者消融成功概率降低。特別是左心房擴(kuò)大、二尖瓣病變和慢性心力衰竭患者手術(shù)結(jié)果較差。先前認(rèn)為心房顫動(dòng)消融前至少有一種抗心律失常藥物無效。不過,鑒于抗心律失常藥物的已知毒性和消融的成功,消融術(shù)已成為初始節(jié)律控制的方案,至少適合陣發(fā)性心房顫動(dòng)。
最近的心房顫動(dòng)消融指南更新是2014美國和2012歐洲指南(見表1)。對(duì)于有癥狀的陣發(fā)……
登錄APP查看全文
猜你喜歡
環(huán)球時(shí)報(bào)(2022-12-23)2022-12-23 09:28:37
昆明醫(yī)科大學(xué)學(xué)報(bào)(2022年1期)2022-02-28 07:45:04
中老年保健(2021年11期)2021-08-22 03:13:36
昆明醫(yī)科大學(xué)學(xué)報(bào)(2021年2期)2021-03-29 07:42:46
河北畫報(bào)(2020年10期)2020-11-26 07:20:50
小學(xué)閱讀指南·低年級(jí)版(2017年1期)2017-03-13 20:07:35
中國衛(wèi)生標(biāo)準(zhǔn)管理(2015年3期)2016-01-14 03:41:47
中國醫(yī)療美容(2015年1期)2015-07-12 10:06:38
鄭州大學(xué)學(xué)報(bào)(醫(yī)學(xué)版)(2015年2期)2015-02-27 14:50:54
西南軍醫(yī)(2014年5期)2014-04-25 07:42:48