D-二聚體、纖維蛋白原、纖維蛋白(原)降解產物在強直性脊柱炎中的臨床意義
2019-11-14 13:01:45俞烜華黃惠娟
中國當代醫藥 2019年26期
俞烜華 黃惠娟
[摘要]目的 探討D-二聚體(DD)、纖維蛋白原(FIB)、纖維蛋白(原)降解產物(FDP)在強直性脊柱炎(AS)中的臨床意義。方法 選取2014年6月~2018年12月我院收治的60例AS患者及67例健康體檢人群作為研究對象,比較其血漿DD、FIB及FDP水平,分析其與C反應蛋白(CRP)、紅細胞沉降率(ESR)、血小板(PLT)及AS疾病活動指數評分(BASDAI)、AS功能指數評分(BASFI)的關系;同時將AS患者分為疾病活動組(BASDAI≥4分)和疾病緩解組(BASDAI<4分),比較分析兩組患者的年齡、病程、DD、FIB、FDP、CRP、ESR、PLT、BASFI水平。結果 ①AS患者血漿DD、FIB、FDP水平高于健康對照者(P<0.05)。②AS疾病活動組患者的DD、FIB、FDP、ESR、BASFI高于疾病緩解組(P<0.05);AS疾病活動組患者的病程長于疾病緩解組(P<0.05);兩組患者的年齡、CRP、PLT比較,差異無統計學意義(P>0.05)。③AS患者血漿DD、FIB、FDP水平與ESR、CRP、BASDAI、BASFI均成正相關(ρ=0.473、0.449、0.424、0.409,0.827、0.750、0.442、0.391,0.545、0.622、0.544、0.373;P<0.05)。④AS患者FDP與年齡成正相關(ρ=0.308,P<0.05),DD、FIB與年齡無相關性(P>0.05),DD、FIB、FDP與病程均無相關性(P>0.05)。結論 AS患者,尤其在疾病活動期凝血-纖溶系統異常,與AS心血管損害、病程、疾病活動指標及功能指數相關,DD、FIB、FDP可作為評價AS疾病活動、功能的指標。
[關鍵詞]D-二聚體;纖維蛋白原;纖維蛋白(原)降解產物;脊柱炎;強直性
[中圖分類號] R593.2 ? ? [文獻標識碼] A ? ? [文章編號] 1674-4721(2019)9(b)-0011-05
Clinical significance of D-dimer, fibrinogen and fibrinogen degradation products in ankylosing spondylitis
YU Xuan-hua1? ?HUANG Hui-juan2
1. Department of Rheumatology, People′s Hospital Affiliated to Fujian University of Traditional Chinese Medicine, Fujian Province, Fuzhou? ?350004, China; 2. Department of Preventive Treatment of Disease, People′s Hospital Affiliated to Fujian University of Traditional Chinese Medicine, Fujian Province, Fuzhou? ?350004, China
[Abstract] Objective To investigate the clinical significance of D-dimer (DD), fibrinogen (FIB) and fibrinogen degradation product (FDP) in ankylosing spondylitis (AS). Methods A total of 60 AS patients and 67 healthy people admitted to our hospital from June 2014 to December 2018 were selected as the subjects. The plasma levels of DD, FIB and FDP of them were compared and analyzed. The relationship between plasma levels of DD, FIB and FDP and C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), platelet (PLT), bath ankylosing spondylitis disease activity index (BASDAI) and bath ankylosing spondylitis functional index (BASFI) were analyzed. At the same time, AS patients were divided into disease active group (BASDAI≥4 points) and disease remission group (BASDAI<4 points). The levels of age and course of disease, DD, FIB, FDP, CRP, ESR, PLT, BASFI were compared and analyzed between the two groups. Results ① The plasma levels of DD, FIB and FDP in AS patients were significantly higher than those in healthy controls (P<0.05). ②The levels of DD, FIB, FDP, ESR and BASFI in AS disease active group were significantly higher than those in remission group (P<0.05). The course of disease in AS disease active group was longer than that in remission groupin AS disease active group were significantly higher than those in remission group (P<0.05). There was no significant difference in age, CRP and PLT between the two groups (P>0.05). ③ The levels of plasma DD, FIB and FDP in AS patients were positively correlated with ESR, CRP, BASFI and BASDAI (ρ=0.473, 0.449, 0.424, 0.409, 0.827, 0.750, 0.442, 0.391, 0.545, 0.622, 0.544, 0.373; P<0.05). ④ FDP was positively correlated with age in AS patients (ρ=0.308, P<0.05). There was no correlation between DD, FIB and age in AS patients (P>0.05), and there was no correlation between DD, FIB, FDP and course of disease either (P>0.05). Conclusion In AS patients, especially in active stage, coagulation-fibrinolysis system is abnormal, which are related to the cardiovascular damage, course of AS, disease activity index and function index. DD, FIB and FDP may be used as indicators to evaluate the activity, function of AS.
[Key words] D-dimer; Fibrinogen; Fibrinogen degradation product; Spondylitis; Ankylosing
強直性脊柱炎(ankylosing spondylitis,AS)是一種主要累及中軸關節的慢性炎癥性疾病,屬于脊柱關節炎(spinal arthritis,SpA)。相關研究顯示,AS患者心臟受累的患病率高達46.56%[1],常見的表現有主動脈炎、主動脈瓣關閉不全及房室傳導阻滯[2]。D-二聚體(D-dime,DD)是交聯纖維蛋白經纖溶酶水解作用所產生的一種特異性纖維蛋白降解產物[3]。纖維蛋白原(fibrinogen,FIB)介導血小板聚集,參與凝血過程,影響血液黏度,對血栓的形成具有重要意義,也是心血管病發生的重要危險因素[4]。纖維蛋白(原)降解產物(fibrinogen degradation product,FDP)是在纖溶酶的作用下,血液中的纖維蛋白/纖維蛋白原被溶解所產生的各種降解產物的總稱[5]。文獻報道類風濕關節炎(rheumatoid arthritis,RA)、系統性紅斑狼瘡(systemic lupus erythematosus,SLE)患者體內均有凝血-纖溶系統異常,凝血-纖溶指標DD、FIB、FDP參與RA、SLE病理過程并與病情活動、心血管事件的發生相關[6-8]。相關研究顯示,SpA患者的DD、FIB水平升高,與疾病活動度相關[9]。凝血-纖溶系統異常及指標在AS中的臨床意義目前研究報道少見。本研究通過檢測我院60例AS患者及67例健康對照者的DD、FIB、FDP水平,探討其與C反應蛋白(C-reactive protein,CRP)、紅細胞沉降率(erythrocyte sedimentation rate,ESR)、血小板(platelet,PLT)及AS疾病活動指數評分(bath ankylosing spondylitis disease activity index,BASDAI)、AS功能指數評分(bath ankylosing spondylitis functional index,BASFI)等指標的關系,現報道如下。
1資料與方法
1.1 一般資料
選取2014年6月~2018年12月我院收治的60例AS患者,其中男39例,女21例;年齡27~76歲,平均(47.57±13.70)歲;病程M=5年,P25~P75(3.00~10.38)年。所有AS患者按BASDAI[10]、BASFI[11]評分表評分進行分組:①疾病活動組(BASDAI≥4)28例,其中男18例,女10例;年齡(50.18±12.06)歲;病程M=10年,P25~P75(4.25~20.00)年。②疾病緩解組(BASDAI<4)32例,其中男21例,女11例;年齡(45.28±14.80)歲;病程M=5年,P25~P75(2.13~10.00)年。兩組患者的一般資料比較,差異無統計學意義(P>0.05),具有可比性。另隨機選取同期于我院體檢的健康人群67例作為對照,其中男44例,女23例;年齡28~68歲,平均(50.31±8.58)歲。健康對照者的年齡、性別等一般資料與AS患者比較,差異無統計學意義(P>0.05),具有可比性。本研究得到我院醫學倫理委員會批準,AS患者及健康對照者均簽署知情同意書。
1.2納入與排除標準
納入標準:診斷均符合1984年修訂的AS紐約分類標準[2]。
排除標準:①合并RA、SLE等自身免疫性疾病者;②合并腫瘤者;③1個月內使用過抗凝溶栓類藥物,合并動靜脈血栓性疾病者;④6個月內有手術、外傷史者;⑤肝、腎功能異常者。
1.3方法
按照所測項目要求采集入組AS患者及健康對照者的空腹靜脈血,留取全血,離心分離血漿,留取血清標本,所有項目均即時檢測。
1.3.1實驗儀器? DD、FIB、FDP采用日本希森美康CS 5100血凝儀檢測;CRP采用美國貝克曼-庫爾特(BECKMAN COULTER)IMMAGE 800儀器檢測;ESR采用意大利vital Diagnotincs血沉儀MONITOR20檢測。
1.3.2實驗試劑? DD、FIB試劑廠家為日本西門子公司(SIEMENS);FDP試劑為日本BIOLINKS CO、LTD,CRP試劑為BECKMAN COULTER。
1.3.3實驗方法? 檢測DD、FDP、CRP的實驗方法為免疫比濁法;FIB為凝固法。
1.4統計學方法
采用SPSS 25統計學軟件進行數據分析,符合正態分布的計量資料以均數±標準差(x±s)表示,兩組間比較采用獨立樣本t檢驗;偏態分布的計量資料,采用中位數(M)、四分位間距(P25~P75)表示,兩組間比較采用Mann-Whitney U檢驗;相關分析采用Spearman相關分析(相關系數ρ),以P<0.05為差異有統計學意義。
2結果
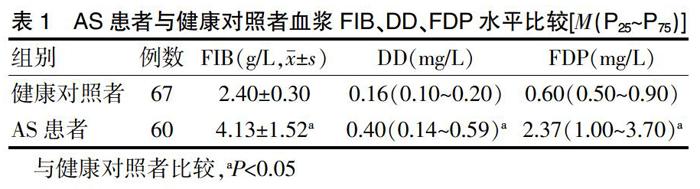
2.1 AS患者與健康對照者血漿DD、FIB、FDP水平的比較
AS患者的血漿DD、FIB、FDP水平高于健康對照者,差異有統計學意義(P<0.05)(表l)。
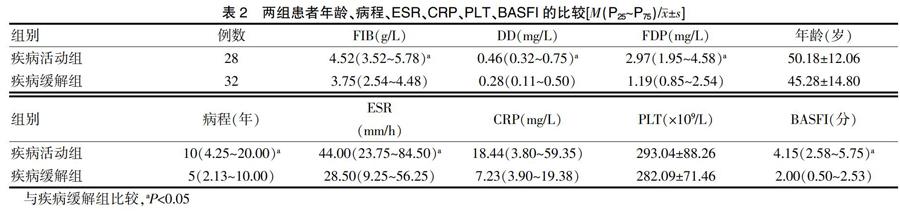
2.2兩組AS患者DD、FIB、FDP、年齡、病程、ESR、CRP、PLT及BASFI的比較
AS疾病活動組患者的血漿DD、FIB、FDP、ESR、BASFI高于疾病緩解組(P<0.05);AS疾病活動組患者的病程長于疾病緩解組(P<0.05);兩組AS患者的年齡、CRP、PLT比較,差異無統計學意義(P>0.05)(表2)。
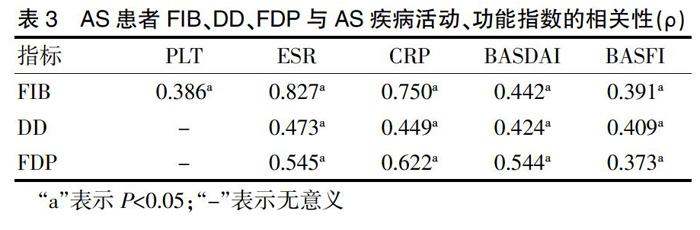
2.3 AS患者血漿DD、FIB、FDP與AS疾病活動、功能指數的相關性
綜上所述,AS患者存在凝血-纖溶系統指標異常,尤其是病程早、疾病活動時高凝狀態,可能有微血栓形成及繼發纖溶亢進,可能是AS易導致心血管損害的因素。病程長的AS患者更易出現疾病活動,DD、FIB、FDP與AS病情活動、功能指數相關指標相關。
[參考文獻]
[1]薛曉燕,李軍霞,李小峰.強直性脊柱炎患者心臟受累危險因素研究[J].中國當代醫藥,2016,23(12):22-25.
[2]Atzeni F,Corda M,Sarzi-Puttini P,et al.From Old to New Cardiovascular Complications in Ankylosing Spondylitis[J].Isr Med Assoc J,2017,19(8):506-509.
[3]曹清蕓,王素寧.毛細支氣管炎患兒血清TNF-α、VEGF、CK-MB及血漿D-二聚體水平的變化及臨床意義[J].國際檢驗醫學雜志,2019,(8):959-963.
[4]黃勁,尹小建,黃芳.纖維蛋白原相關藥物研究進展[J].藥學研究,2019,38(3):167-171.
[5]陸貞妮,劉小勇,許冠群,等.不同血凝儀試劑放置倉內時間對纖維蛋白(原)降解產物結果的影響[J].山西醫藥雜志,2018,47(14):1718-1720.
[6]曾惠瓊,扶忠超,黃新民,等.D-二聚體、纖維蛋白原、轉鐵蛋白水平對類風濕關節炎的臨床意義[J].檢驗醫學,2017, 32(10):883-885.
[7]李艷麗,喻雄杰,廖勇敢,等.抗環瓜氨酸肽、纖維蛋白原和D-二聚體與類風濕關節炎患者病情活動性的關系研究[J].醫學綜述,2016,22(7):1388-1390.
[8]薛曉倩,江洪耿,許百潔,等.D-二聚體、纖維蛋白原在系統性紅斑狼瘡及狼瘡腎炎中的價值[J].中國當代醫藥,2018, 25(31):18-21.
[9]王育凱.脊柱關節炎患者D-二聚體和纖維蛋白原檢測臨床意義初探[J].新醫學,2013,44(7):472-475.
[10]Sellas I Fernandez A,Juanola Roura X,Alonso Ruiz A,et al.Clinical utility of the ASDAS index in comparison with BASDAI in patients with ankylosing spondylitis (Axis Study)[J].Rheumatol Int,2017,37(11):1817-1823.
[11]Kviatkovsky MJ,Ramiro S,Landewé R,et al.The minimum clinically important improvement and patient-acceptable symptom state in the BASDAI and BASFI for patients with ankylosing spondylitis[J].J Rheumatol,2016,43(9):1680-1686.
[12]Park CJ,Choi YJ,Kim JG,et al.Association of acute myocardial infarction with ankylosing spondylitis:a nationwide longitudinal cohort study[J].J Clin Neurosci,2018,56:34-37.
[13]Prati C,Racadot E,Cedoz JP,et al.Thrombin generation in ankylosing spondylitis[J].Clin Rheumatol,2011,30(4):511-514.
[14]Tsang HHL,Chung HY.The discriminative values of the bath ankylosing spondylitis disease activity index,ankylosing spondylitis disease activity score,C-reactive protein,and erythrocyte sedimentation rate in spondyloarthritis-related axial arthritis[J].J Clin Rheumatol,2017,23(5):267-272.
[15]劉斌,郭傳友,劉文曲,等.血沉及C反應蛋白判定強直性脊柱炎病情活動的價值[J].中華內科雜志,2005,44(8):566-569.
[16]侯娜莉,張華,朱桂啟,等.D-二聚體與強直性脊柱炎病情活動度的相關性研究[J].風濕病與關節炎,2015,4(5):22-24.
[17]李振彬,路占忠,龍建國.D-二聚體檢測在強直性脊柱炎中的臨床意義[J].解放軍醫藥雜志,2015,27(1):56-59.
[18]李菁.強直性脊柱炎患者凝血、纖溶相關指標的臨床意義[J].交通醫學,2014,28(4):356-357.
[19]方利,劉健,朱福兵,等. 基于細胞因子/ NF-B信號通路探討強直性脊柱炎患者血液高凝狀態形成的機制[J].中華中醫藥雜志,2016,31(9):3756-3759.
[20]Tao K,Tang X,Wang B,et al.Distinct expression of chemokine-like factor 1 in synovium of osteoarthritis,rheumatoid arthritis and ankylosing spondylitis[J].J Huazhong Univ Sci Technolog Med Sci,2016,36(1):70-76.
[21]方妍妍,劉健,萬磊,等.基于關聯規則對423例強直性脊柱炎患者血小板參數與免疫炎癥代謝指標的數據挖掘研究[J].中國免疫學雜志,2018,34(7):1039-1043,1049.
[22]吳偉紅,張仕玉.強直性脊柱炎的臨床診斷與中醫方劑治療[J].湖北師范學院學報(自然科學版),2016,36(2):29-32.
[23]杜旭娜,李晏,張勝利,等.強直性脊柱炎病情活動度評分對強直性脊柱炎患者病情活動性判斷的價值[J].中華內科雜志,2012,51(3):206-209.
(收稿日期:2019-04-16? 本文編輯:閆? 佩)
猜你喜歡
現代臨床醫學(2022年4期)2022-09-29 07:38:00
少先隊活動(2022年5期)2022-06-06 03:45:04
家庭科學·新健康(2022年3期)2022-05-10 00:32:13
中老年保健(2021年2期)2021-08-22 07:31:10
昆明醫科大學學報(2021年4期)2021-07-23 01:21:50
少先隊活動(2021年1期)2021-03-29 05:26:36
快樂語文(2020年30期)2021-01-14 01:05:38
云南醫藥(2019年3期)2019-07-25 07:25:14
海峽姐妹(2018年3期)2018-05-09 08:20:40
海南醫學(2016年8期)2016-06-08 05:43:00