Three-dimensional computed tomography mapping of posterior malleolar fractures
2020-04-22 07:12:58QiHangSuJuanLiuYanZhangJunTanMeiJunYanKaiZhuJinZhangCongLi
World Journal of Clinical Cases 2020年1期
Qi-Hang Su,Juan Liu,Yan Zhang,Jun Tan,Mei-Jun Yan,Kai Zhu,Jin Zhang,Cong Li
Qi-Hang Su,Yan Zhang,Jun Tan,Mei-Jun Yan,Kai Zhu,Jin Zhang,Department of Orthopedics,Shanghai East Hospital,Tongji University School of Medicine,Shanghai 200120,China
Juan Liu,Department of the First Clinical Medical School,Shanxi Medical University,Taiyuan 030000,Shanxi Province,China
Jun Tan,Department of Orthopedics,Pinghu Second People's Hospital,Pinghu 314200,Zhejiang Province,China
Cong Li,Department of Trauma Surgery,Shanghai East Hospital,Tongji University School of Medicine,Shanghai 200120,China
Abstract
Key words: Three-dimensional imaging;Maps;Ankle fractures;Computed tomography
INTRODUCTION
Ankle fractures account for roughly 10% of all fracture cases,indicating that they are one of the most common injuries in clinical practice and often require surgical intervention[1].Posterior malleolar fractures have been reported to occur in < 40% of ankle fractures[2].Numerous research findings have demonstrated that the presence of posterior malleolar fragment (PMF) is widely regarded as a critical prognostic factor or outcome indicator following ankle fracture treatment[2-5].As previously reported,patients with PMF ankle fractures exhibit poor clinical outcomes in comparison with uni- or bi-malleolar ankle fractures[2].
Despite this,the optimal treatment procedures for posterior malleolar fractures remain controversial.The first treatment proposed by Reganet al[6]has been applied for decades,in which the fixation of coronoid fractures is based on size and articular involvement.More recently,it has been suggested that the patterns of coronoid fracture,especially their morphological features,are superior compared to the height of coronoid fracture[7-9].Similarly,through the use of computed tomography (CT)-based PMF mapping in a subset of patients (n= 45),Mangnuset al[10]found that the morphology of PMF can be more crucial than fragment size alone for clinical decision making.Specifically,Haraguchi type II can be considered as an individual fracture pattern.Recently,there has been increasing interest in the morphological characterization of such fractures and reaching a consensus on surgical treatment.
To examine the pathoanatomical or morphological features of PMF,various studies have utilized plain radiograph[11],CT scan[12]and three-dimensional (3D)reconstruction CT[13].Typically,the lateral view of plain radiograph can be used to assess PMF in ankle fractures.However,the plain radiographic assessment of PMF may be unreliable and inaccurate,even though the estimation of PMF size,including tibial articular surface,is feasible[14].Given the rising concerns toward big data analytics,3D CT-based fracture mapping has been commonly applied in orthopedic fields such as the characterization of scapular and thoracolumbar fractures[15,16],as initially described by Coleet al[17].
In the present study,our aims were to divide the position and prevalence of fracture lines of a series of posterior malleolar fractures into two groups:supinationexternal rotation grade IV (SER4) and pronation-external rotation grade IV (PER4)groups,as per the Lauge-Hansen classification system[18](Figure 1) and to produce fracture maps through 3D CT mapping.We postulated that the 3D maps of posterior malleolar fractures would demonstrate the fracture lines,fracture characteristics and recurrent patterns of PMF,which would have the potential to enhance surgeons'understanding and recognition of PMF during diagnostic intervention,preoperative planning,surgery and proper internal fixation.In addition,the 3D maps of medial malleolus and fibula were also obtained from the two groups.
MATERIALS AND METHODS
Patient cohort
A retrospective analysis was undertaken for the CT imaging data of patients diagnosed with PMF in our institution from January 2010 to December 2017.This data was obtained by searching the picture archiving and communication system database.All fractures were classified based on the Lauge-Hansen system[18],where the first term represents the position of the foot at the time of injury and the second term indicates the external force applied to the foot,in order to create specific fracture patterns.Inclusion criteria were as follows:(1) Participants must have either SER4 injuries or PER4 injuries;(2) Participants without pathological and osteoporotic posterior malleolar fractures;and (3) Good-quality CT images must be available.Participants were excluded if they:(1) Had fracture lines or anatomical landmarks obscured by foreign bodies;and (2) Had severe comminuted fractures in which the conditions of fracture lines were difficult to be determined.The data of participants were evaluated by a highly experienced orthopedic surgeon and senior investigator through the 3D CT rendering in the picture archiving and communication system database.
Fracture mapping
With increasing concern over the big data analytics,the distribution map of fracture lines (named fracture mapping) based on 3D CT has also been widely used in orthopedic fields to characterize fractures[16].The raw data in digital imaging and communications in medicine format were recorded by a 64-channel CT scanner(Siemens Somatom Sensation,Siemens,Erlangen,Germany) with the following parameters:0.5 mm interlayer spacing,1 mm slice thickness,200 mA tube current and 120 kV tube voltage.Subsequently,the digital imaging and communications in medicine data for all participants were inputted to Mimics 20.0 software (Materialise,Leuven,Belgium).Through threshold segmentation,the fragments of ankle joint were separated and reconstructed.Following this,the 3D reconstruction model of each fragment was generated using the STL file.The reconstructed model was then inputted to 3-matic 12.0 software (Materialise,Leuven,Belgium) in order to reposition the fragments.This was followed by overlapping and matching with the model of typical ankle through slight adjustment and standardization.Fracture lines were drawn on the typical ankle model in compliance with the existing fracture model,while the 3D maps were obtained by superimposing the fracture lines of all participants (Figure 2).
Statistical analysis
The fracture characteristics of patients were analyzed using the frequencies and percentages for categorical variables as well as arithmetic means for continuous variables.To compare whether gender is correlated with posterior malleolus fracture among SER and PER groups,a Pearsonχ2hypothesis test was conducted with the level of α = 0.05 (V20.0,SPSS,Chicago,IL,United States).Descriptive analyses were carried out for each group using a combination of 3D mapping generation.
RESULTS
The present study enrolled 112 patients,of which 80 were in the SER4 group and 32 in the PER4 group.Participants had an average age of 49 (SD = 15.09 years;Figure 3).Patient demographics are summarized in Table 1.The results of Pearsonχ2hypothesis test demonstrated that the value ofχ2was 1.600 andPvalue was 0.206 (P> 0.05).This indicated that there was no statistically significant difference between gender in the two groups.
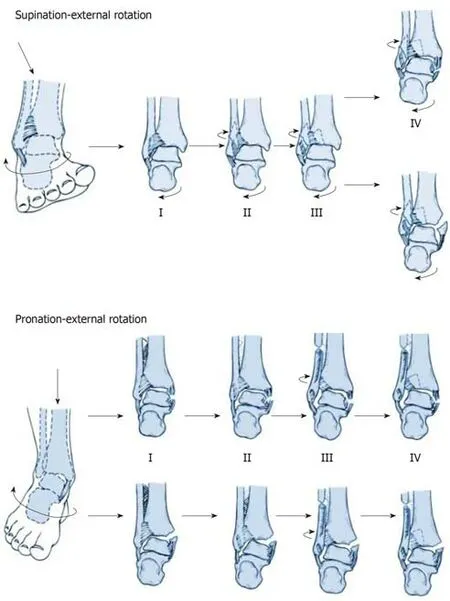
Figure1 The injury mechanisms of supination-external rotation grade IV and pronation-external rotation grade IV groups.
Comparison of the 3D maps of the two groups (SER group,Figure 4;PER group,Figure 5) revealed that the features shared by both groups was the presence of medial malleolus fractures and lateral malleolus fractures among all cases with posterior malleolus fracture.However,when compared to the PER4 ankle fracture,which demonstrated larger fragments following posterior ankle fracture,the posterior ankle fracture fragments resulting from SER4 ankle fractures exhibited relatively smaller fragments.In addition,distribution analyses on posterior malleolus fracture lines indicated that the SER group tended to have higher linear density but more concentrated and orderly distribution fracture lines compared to the PER group.This was supported by a number of posterior malleolus fracture lines extending to the medial malleolus.However,no significant difference in the distribution of medial malleolus fracture lines was found between the two groups.
In addition,an apparent difference was found in the distribution of lateral malleolus fracture lines between the two groups.Notably,the majority of lateral malleolus fracture lines in the SER group originated from the lower end of the fibula before extending upwards along the anterior-to-posterior portion at an oblique angle.Comparatively,the lateral malleolus fracture lines originated from a higher localization in the PER group,followed by generating a non-uniform random distribution.Most of them extended upwards along the anterior-to-posterior portion at an oblique angle with a spiral pattern,indicating that they tended to have a greater length.
DISCUSSION
Fractures of the posterior malleolar commonly occur and may result from a rotational injury.Although treatment for associated lateral and medial structures has been well founded,controversy exists regarding their management.

Figure2 The process of three dimensional fracture mapping in the software programs.
Typically,the fixation approach for posterior malleolus fracture is a precise reduction of bone fragment through ligament reconstruction,followed by fixation with screws along an anterior-to-posterior direction.Obviously,the advantage of this technique lies in the fact that patients remain in a supine position for a minimally invasive operation.However,its disadvantage is the high-failure rates of ligament reconstruction.In addition,it is impossible to remove the residual bone fragments in the joint.Some studies report the use of a posterolateral approach[19-23],which has gained considerable attention and recognition.The unique leverage of this method is its direct achievement of an anatomical reduction as well as a stable fixation along the posterior-to-anterior direction with screws or plates.This approach also enabled the removal of intra-articular loose bodies that may interfere with anatomic reduction.However,the drawback of this surgery is that it requires a prone or lateral position for patients.In addition,some retrospective clinical studies have demonstrated that the open posterolateral approach for fixing a posterior malleolus fracture is much greater than percutaneous anterior-to-posterior screw fixation.Nevertheless,these findings need to be further verified by prospective comparative trials[24].
Through the use of 3D-map analyses,our study clearly demonstrated theuniformity and enrichment of posterior malleolus fracture lines in the SER group.In spite of a less extensive distribution of corresponding fracture lines,several smaller fragments protruded easily into the joints between the tibia and fibula as well as the joints between the tibia and talus.It is worth noting that these fragments generally have a sizeable impact on ankle joint prognosis,given the difficulty of achieving a complete reduction indirectly by ligament repairing as well as the challenges of achieving stable fixationviascrews.This indicates that the functional rehabilitation of the ankle joint has been compromised to a large extent.Distribution analyses of the 3D maps revealed a scattered,non-uniform pattern of fracture lines in the PER group,many of which had extended to the medial malleolus with more severe degrees of fracture.In addition,the fracture surfaces of corresponding fragments appeared to have rough edges.It is interesting that this particular type of fracture fragment exhibits a better chance of achieving a positive effectviaindirect ligament reconstruction.Therefore,it is reasonable to believe that in most cases of SER4 injuries,it is possible to successfully apply the posterolateral approach for fracture reduction and fixation.In contrast,for PER4 injuries,screw fixation along the anterior-to-posterior direction can generally be applied,which leads to a great effect of reduction and fixation.
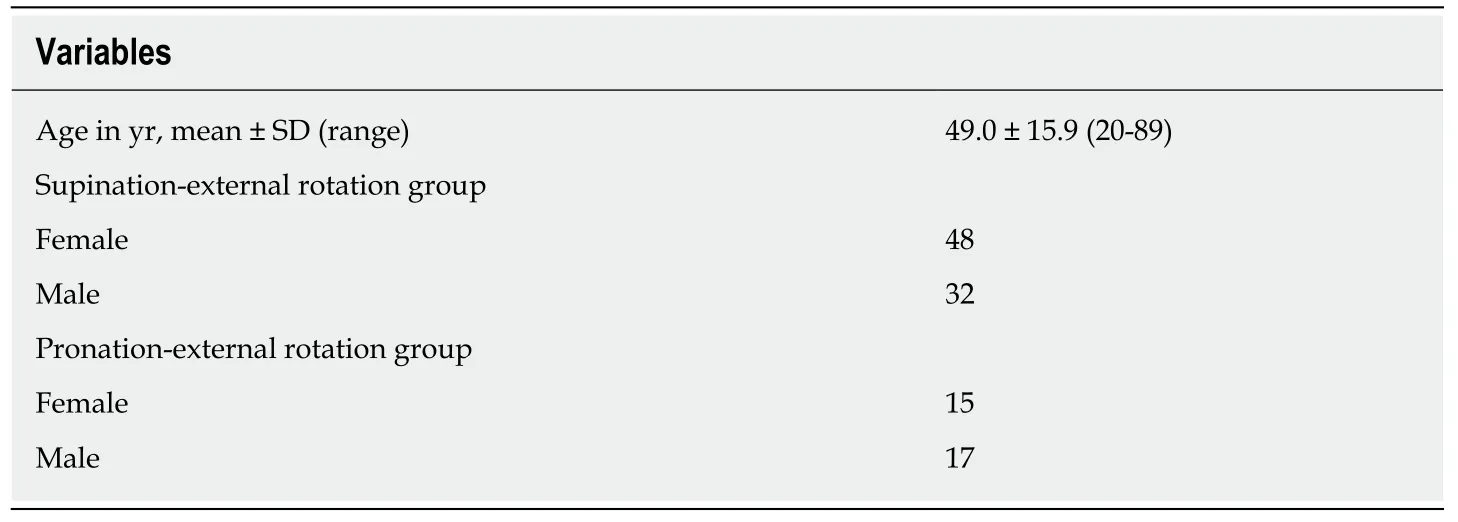
Table1 Patient demographics,n = 112
Several studies have reported a high rate (33.5%) of clinical- and/or radiologicdiagnosed osteoarthritis following posterior malleolar fractures.Besides,there is no significant effect of fragment size on long-term outcomes after conservative or surgical management of posterior malleolus fractures.However,Mingo-Robinetet al[25]and McDanielet al[26]have demonstrated that the outcome of posterior malleolus fractures can be improved if the fracture size is less than or equal to 25% of total distal articular surface without affecting the quality of reduction.Additionally,they recommend that the anatomic reduction of PMF may be required for greater fracture size (≥ 25%) and that failure to achieve a considerable reduction and correction of PMF subluxation does not change the overall outcome.However,our results,based on morphological analysis,seem to suggest otherwise.It is noted that if screw fixation is applied along the anterior-to-posterior direction,small PMFs may exert a greater impact on the functional rehabilitation of the ankle joint,even though this method does not achieve better reduction and fixation because the fracture fragments are typically small.
Nevertheless,it is unlikely that one single factor plays a decisive role in the functional rehabilitation of the ankle joint following posterior malleolus fracture,especially as trimalleolar fractures involve both medial malleolus and lateral malleolus.Instead,it is necessary to comprehensively evaluate the impact of a diverse set of potential risk factors,including the size,shape and location of fragments and the smoothness of fracture surface as well as other elements of fracture fixation,surgical approach and post-surgical rehabilitation.After comprehensive assessment,we recommend that individualized treatment is the best option.Moreover,we believe that most single-factor assessments deviating from the inclusion of comprehensive factors are defective and unreliable.Overall,multi-factor analyses and assessments,larger sample size,prolonged follow-up period and multicenter prospective controlled trials are needed for future investigations.
Fracture maps revealed the fracture characteristics and recurrent patterns of the posterior malleolar fractures,which might help to improve the understanding of ankle fracture as well as increase opportunities for follow-up research and aid clinical decision-making.
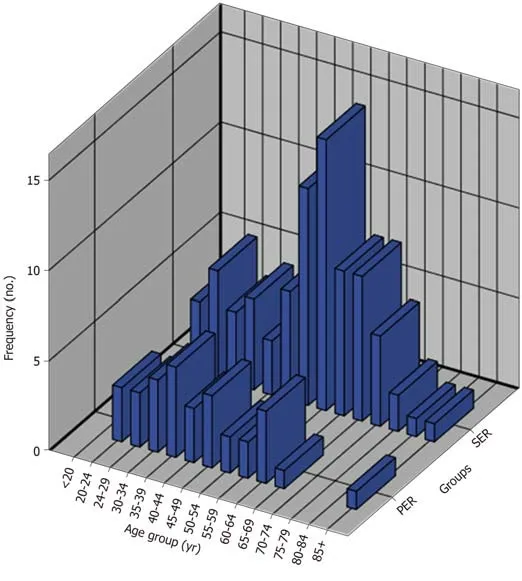
Figure3 Histogram of the age groups of all subjects.
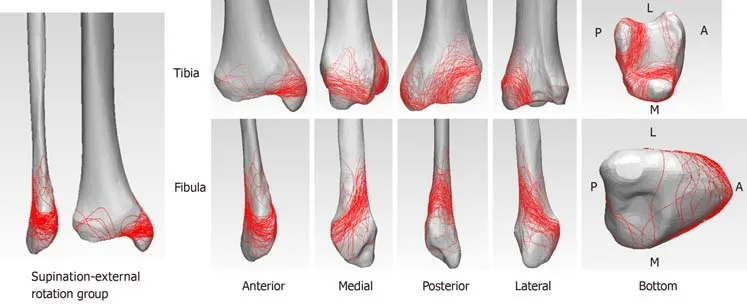
Figure4 The three dimensional fracture maps of supination-external rotation grade IV group.
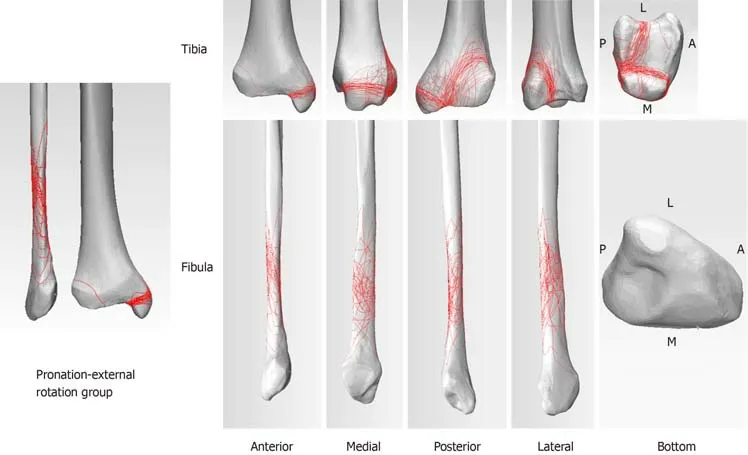
Figure5 The three dimensional fracture maps of pronation-external rotation grade IV group.
ARTICLE HIGHLIGHTS
Research background
Posterior malleolar fractures have been reported to occur in < 40% of ankle fractures,which is widely regarded as a critical prognostic factor or outcome indicator following ankle fracture treatment.The morphology of posterior malleolar fractures can be more crucial than fragment size alone for clinical decision making.
Research motivation
The optimal treatment procedures for posterior malleolar fractures remain controversial.The fracture characteristics and recurrent patterns of the posterior malleolar fractures are unclear.
Research objectives
In this study,the authors aimed to reveal the recurrent patterns and characteristics of posterior malleolar fractures by creating fracture maps of the posterior malleolar fractures through the use of computed tomography mapping.
Research methods
A consecutive series of posterior malleolar fractures was used to create three-dimensional reconstruction images to produce the distribution map of fracture lines through threedimensional computed tomography mapping in the Mimics and 3-matic software.
Research results
Three-dimensional maps showed that the posterior ankle fracture fragments in supinationexternal rotation grade IV fractures were relatively smaller than those in pronation-external rotation grade IV fractures after posterior malleolus fracture.In addition,the distribution analyses on posterior malleolus fracture lines indicated that supination-external rotation group tended to have higher linear density but more concentrated and orderly distribution fractures compared to pronation-external rotation group.
Research conclusions
Fracture maps revealed the fracture characteristics and recurrent patterns of the posterior malleolar fractures,which might help to improve the understanding of ankle fracture.
Research perspectives
Multifactor analyses and assessments,larger sample size,prolonged follow-up period and multicenter prospective controlled trials are needed for future investigations.
 World Journal of Clinical Cases2020年1期
World Journal of Clinical Cases2020年1期
- World Journal of Clinical Cases的其它文章
- Cluster headache as a manifestation of a stroke-like episode in a carrier of the MT-ND3 variant m.10158T>C
- Primary intestinal extranodal natural killer/T-cell lymphoma,nasal type:A case report
- Six families with balanced chromosome translocation associated with reproductive risks in Hainan Province:Case reports and review of the literature
- Clinical characteristics on manifestation and gene mutation of a transient neonatal cyanosis:A case report
- Sarcomatoid intrahepatic cholangiocarcinoma mimicking liver abscess:A case report
- Value of dynamic plasma cell-free DNA monitoring in septic shock syndrome:A case report