Utility of multiple endoscopic techniques in differential diagnosis of gallbladder adenomyomatosis from gallbladder malignancy with bile duct invasion:A case report
2020-04-22 01:51:58LiJiaWenJunHongChenYongJinChenKaiLiu
World Journal of Clinical Cases 2020年2期
Li-Jia Wen, Jun-Hong Chen, Yong-Jin Chen, Kai Liu
Li-Jia Wen, Jun-Hong Chen, Yong-Jin Chen, Kai Liu, Department of Hepatopancreatobiliary Surgery, The First Hospital of Jilin University, Changchun 130021, Jilin Province, China
Abstract
Key words: Gallbladder adenomyomatosis; Differential diagnosis; Endoscopic retrograde cholangio-pancreatography; Intraductal ultrasound; SpyGlass; Case report
INTRODUCTION
Gallbladder adenomyomatosis (GAM) is a benign tumor, and the imaging characteristics, such as thickening of the gallbladder wall and a focal mass, usually overlap with the findings in gallbladder malignancy.These similarities have posed considerable difficulties in making an accurate diagnosis of GAM, in particular,distinguishing GAM from gallbladder cancer.It has been reported that approximately 20% of suspected malignant biliary strictures were postoperatively confirmed as benign lesions[1].Computed tomography (CT) is widely used in the preoperative assessment of gallbladder lesions[2].However, CT imaging alone has been shown to reach an overall accuracy of only 70%-80% for biliary stenosis[3].Until now, there has been no definite consensus on the optimal clinical approaches for indeterminate biliary strictures.As such, it is necessary to improve the accuracy of GAM diagnosis and differential diagnosis between GAM and gallbladder cancer.In the present paper,we illustrate a case in which a preoperative diagnosis of GAM was made by a combination of endoscopic and imaging techniques.
CASE PRESENTATION
Chief complaints
A 40-year-old man was referred to our hospital chiefly for a fever and right upper abdominal pain with dark urine.
History of present illness
The patient's symptoms started 7 d ago with right upper pain and fever, which had worsened over the last 72 h.
History of past illness
He had no special medical history.
Personal and family history
None.
Physical examination upon admission
The patient had upper abdominal pain without abdominal distension or vomiting, as well as yellow sclera and film.He had a body temperature of 37.5 °C, heart rate of 72 bpm, blood pressure of 116/68 mmHg, and respiratory rate of 15.
Laboratory examinations
Total bilirubin was 138.8 μmol/L, direct bilirubin was 117.3 μmol/L, CA19-9 was 161.3 U/mL, CA-125 was 15.76 U/mL, AFP was 1.77 ng/mL, carcinoembryonic antigen was 1.29 ng/mL, C-reaction protein was 81.3 mg/L, neutrophil granulocyte percentage was 0.83, and IgG4 was 0.2 g/L.
Imaging examinations
An enhanced CT scan revealed a mass at the neck of the gallbladder involving the bile ducts (Figure 1A) and a shadow was visualized at the end of the common bile duct(Figure 1B).Endoscopic retrograde cholangio-pancreatography (ERCP) showed bile duct dilatation (Figure 2A) and gallstones at the end of the common bile duct (Figure 2B), intraductal ultrasound (IDUS) suggested a benign bile duct stricture (Figure 3),inflammatory change in the bile duct mucosa was visualized by SpyGlass Direct Visualization System imaging (Figure 4), and final pathological examination revealed GAM with chronic cholecystitis and acute suppurative inflammation (Figure 5).
FINAL DIAGNOSIS
GAM and choledocholithiasis.
TREATMENT
The patient underwent laparoscopic cholecystectomy.
OUTCOME AND FOLLOW-UP
Fortunately, neither recurrent GAM nor malignant tumor was observed in the patient during a 12-mo follow-up period.
DISCUSSION
Gallbladder carcinoma is the most common malignant tumor in the biliary system[4].Some benign gallbladder diseases are misdiagnosed as gallbladder carcinoma,resulting in unnecessary surgery.For instance, GAM is an excessively proliferative disease of the gallbladder epithelium with intramural diverticula (Rokitanskye Aschoff sinuses) extending into the thickened muscular layer[2]and its imaging features have some overlaps with those of gallbladder carcinoma when it presents as focal thickening at the body and fundus and a mass with irregularly soft tissue density in the gallbladder, which may simulate a malignancy, resulting in a falsepositive diagnosis of gallbladder carcinoma[5].On the contrary, patients who suffer from gallbladder cancer may present with acute cholecystitis, misdiagnosed as a benign lesion.It has been reported that the hidden incidence of gallbladder cancer combined with cholecystitis ranges from 1%-9%[4].Gallbladder carcinoma originating from the neck can invade the cystic and extrahepatic bile duct, making it difficult to distinguish from extrahepatic cholangiocarcinoma[6,7].When a stricture of the midportion of the extrahepatic bile duct is found in patients presenting with obstructive jaundice, careful evaluation of the cystic duct and gallbladder neck is necessary to rule out gallbladder cancer with metastasis.
With recently developed novel biomarkers and endoscopic techniques, unnecessary surgeries on benign strictures of the bile duct have been greatly reduced.However, no single approach has been reliable in the differential diagnosis of benign and malignant lesions in the gallbladder mainly due to insufficient sensitivity, low specificity, and inaccuracy.By reviewing the published systematic reviews and metaanalysis (Table 1), we identified the diagnostic indices for the evaluation of suspected malignant biliary strictures (Table 1)[1,8-14].We found that the clinical approach of various endoscopies in combination could significantly improve the diagnostic accuracy of indeterminate biliary stricture.It is worth noting in particular that contrast-enhanced ultrasound is very reliable in the differential diagnosis of gallbladder cancer with broad prospects[15,16].CA19-9 should be used cautiously for patients with biliary obstruction because of the potential for a pseudo increase[17].In this case report and review of the literature, we propose a strategy for the evaluation and preoperative diagnosis of gallbladder-occupying lesions with bile duct invasion(Figure 6), which may have great preoperative diagnostic utility.First, a detailed medical history should be obtained, with physical and laboratory examinations, along with abdominal ultrasound to provide the initial evidence for a non-invasive imaging method such as CT or magnetic resonance cholangiopancreatography.These imaging modalities can reveal both the hilar bile duct and gall bladder, which can guide future treatment.Second, an invasive method such as ERCP with IDUS/SpyGlass/probebased confocal laser endomicroscopy/fluorescencein situhybridization or pathology can be used as the primary measure.If endoscopy and laparoscopic cholecystectomy are positive, radical resection of hilar cholangiocarcinoma must be undertaken.If lymphatic metastasis or vascular invasion is found, ERCP stent implantation and radiofrequency ablation can be performed.Otherwise, 12 mo of follow-up is usually necessary.

Figure 1 Enhanced computed tomography imaging.
CONCLUSION
In summary, preoperative diagnosis of GAM is challenging, particularly when it presents imaging features similar to those of gallbladder carcinoma.The findings in this case study suggest that the use of multiple endoscopic techniques in combination may improve the accuracy of GAM diagnosis and benefit the differential diagnosis of GAM from gallbladder cancer.
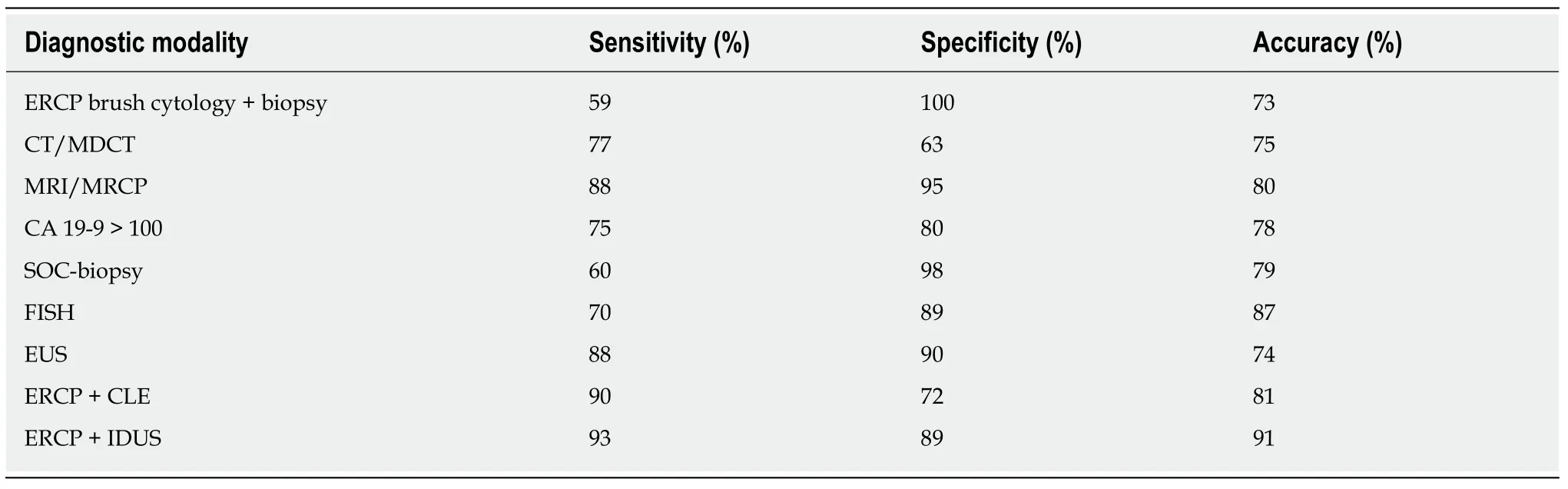
Table 1 Various diagnostic techniques for evaluation of suspected malignant biliary strictures
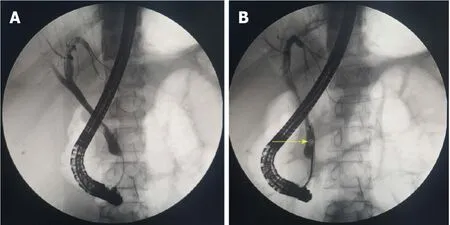
Figure 2 Endoscopic retrograde cholangio-pancreatography.
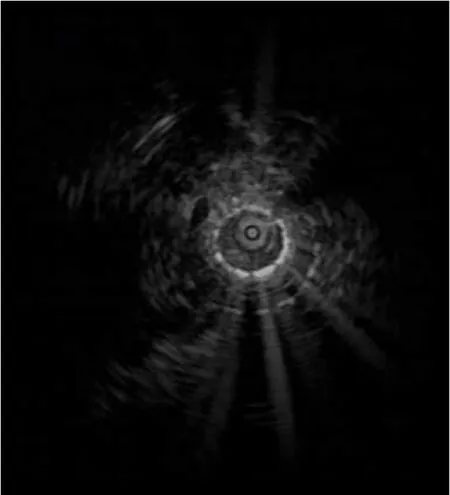
Figure 3 lntraductal ultrasound imaging.
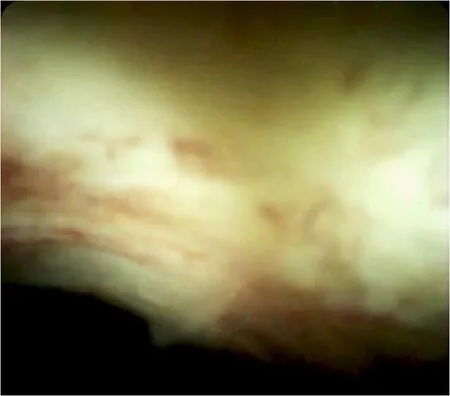
Figure 4 SpyGlass Direct Visualization System imaging.
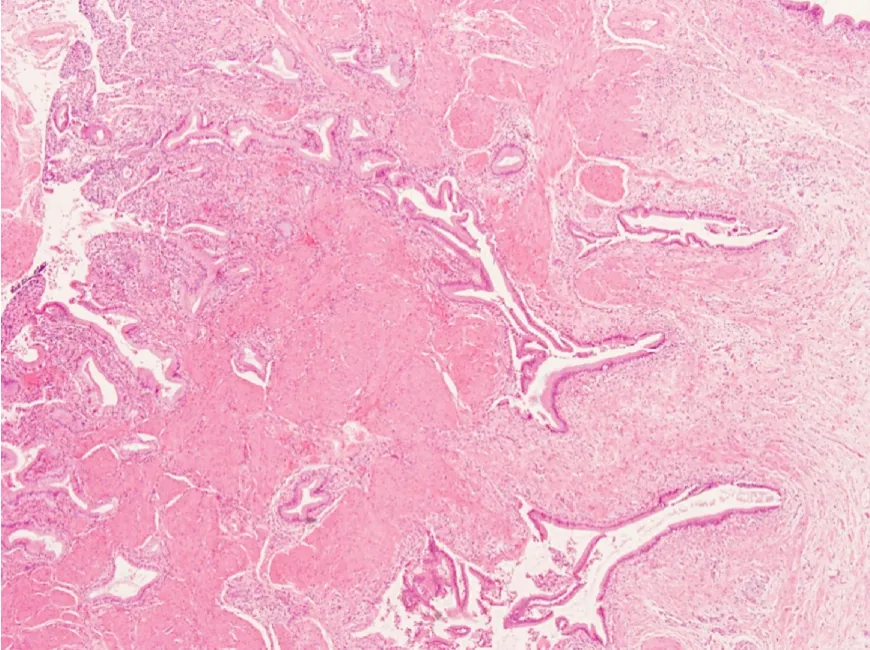
Figure 5 Pathological examination.
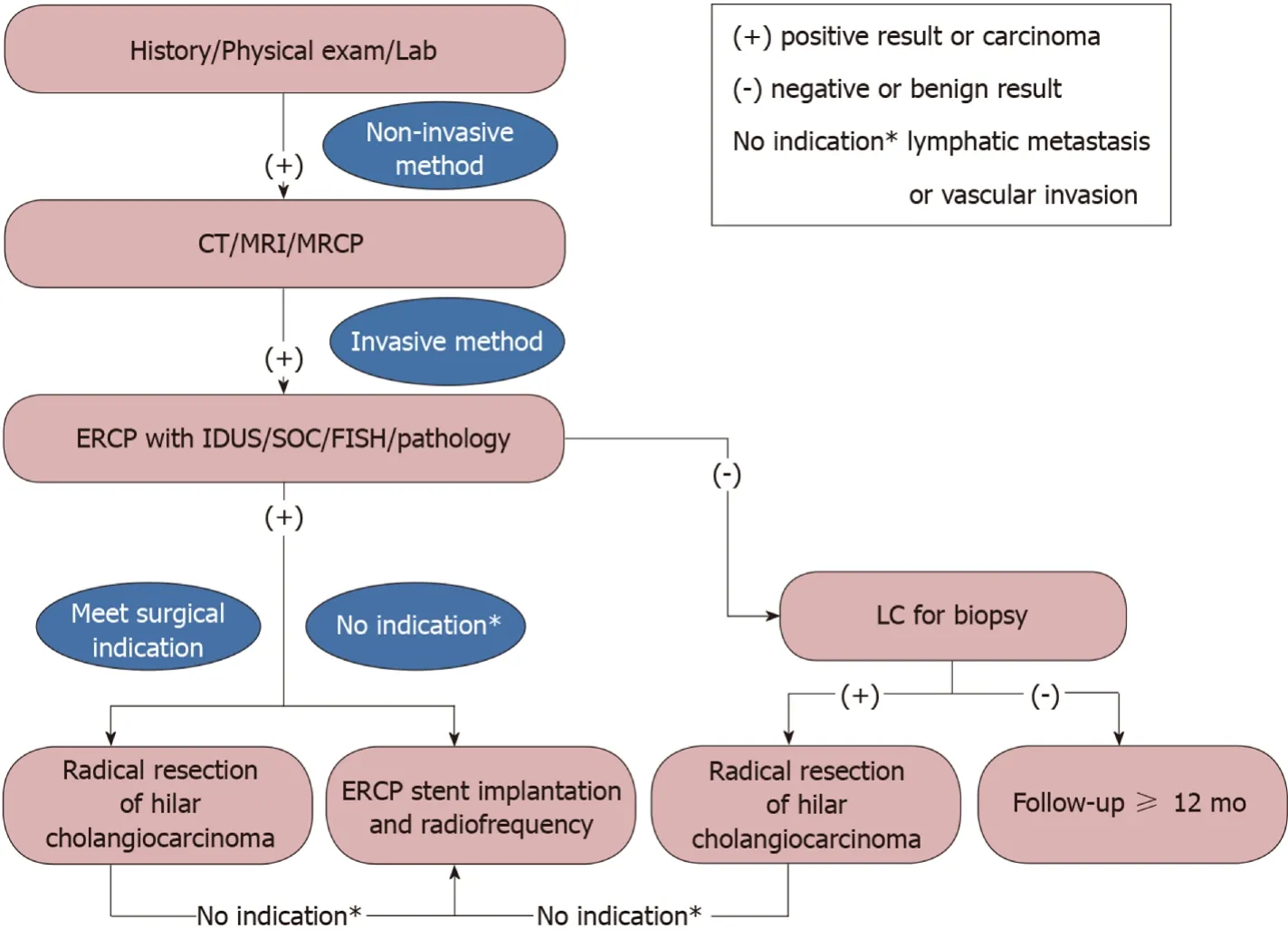
Figure 6 Various endoscopic and radiological imaging modalities for evaluation and preoperative diagnosis of gallbladder occupying lesions with bile duct invasion.
 World Journal of Clinical Cases2020年2期
World Journal of Clinical Cases2020年2期
- World Journal of Clinical Cases的其它文章
- Multiple organ dysfunction and rhabdomyolysis associated with moonwort poisoning:Report of four cases
- Transorbital nonmissile penetrating brain injury:Report of two cases
- Analysis of pathogenetic process of fungal rhinosinusitis:Report of two cases
- Efficacy of comprehensive rehabilitation therapy for checkrein deformity:A case report
- Spontaneous regression of stage III neuroblastoma:A case report
- Excellent response of severe aplastic anemia to treatment of gut inflammation:A case report and review of the literature