Long-term survival of two patients with recurrent pancreatic acinar cell carcinoma treated with radiofrequency ablation:A case report
2020-04-23 06:04:02MariacristinaDiMarcoRiccardoCarloniStefaniaDeLorenzoElisaGrassiAndreaPalloniFrancescaFormicaStefanoBrocchiDariaMariaFilippiniRitaGolfieriGiovanniBrandi
World Journal of Clinical Cases 2020年7期
Mariacristina Di Marco,Riccardo Carloni,Stefania De Lorenzo,Elisa Grassi,Andrea Palloni,Francesca Formica,Stefano Brocchi,Daria Maria Filippini,Rita Golfieri,Giovanni Brandi
Mariacristina Di Marco,Riccardo Carloni,Stefania De Lorenzo,Andrea Palloni,Francesca Formica,Daria Maria Filippini,Giovanni Brandi,Department of Experimental,Diagnostic,and Specialty Medicine - DIMES,Sant'Orsola-Malpighi Hospital,University of Bologna,Bologna 40138,Italy
Elisa Grassi,Medical Oncology,Ospedale degli Infermi,Faenza 48018,Italy
Stefano Brocchi,Rita Golfieri,Radiology Unit,Department of Diagnostic Medicine and Prevention,Sant'Orsola-Malpighi Hospital,University of Bologna,Bologna 40138,Italy
Abstract
Key words: Acinar cell carcinoma;Pancreas;Liver metastasis;Radiofrequency ablation;Case report
INTRODUCTION
Pancreatic acinar cell carcinoma (PACC) is a rare type of malignant pancreatic cancer originating from acinar cells of the exocrine pancreas that represents approximately 1% of all pancreatic neoplasms[1,2].For patients with operable disease,surgical resection is the first choice for treatment.Chemotherapy and radiotherapy have also been used for locally advanced or metastatic PACC;however,there is a lack of controlled,prospective studies due to the very low disease incidence,and there are no definitive guidelines for treating patients with advanced or recurrent disease[3].Although PACC is associated with improved stage-specific survival compared to pancreatic ductal adenocarcinoma (PDAC),the high rate of recurrence after surgery(mainly in the liver) is the primary limitation of treatment[4-7].
Radiofrequency ablation (RFA) is a well-established treatment for hepatocellular carcinoma and represents a good alternative to surgery for colorectal liver metastases[8].There is also a potential role and survival benefit of hepatic ablation in carefully selected patients with non-colorectal liver metastases,such as breast cancer and neuroendocrine tumours (NETs)[9,10].However,for metastatic PDAC,the evidence is inconsistent with regard to metastasectomy or local ablative therapies,even for oligometastatic patients[11].Moreover,only a few cases of PACC liver metastases treated with RFA have been reported in the literature.Here,we describe two PACC patients with long-term survival and recurrent PACC in the liver treated with RFA in addition to chemotherapy.
CASE PRESENTATION
Chief complaints
Case 1:A 43-year-old man without any symptoms who was monitored for familial adenomatous polyposis.
Case 2:A 49-year-old man presenting with a palpable abdominal mass and postprandial abdominal pain over the previous 3 mo.
History of past illness
Case 1:In 1994,the patient was diagnosed with familial adenomatous polyposis (APCgene variant c.847C > T) and treated with prophylactic proctocolectomy with ileoanal pouch.
Case 2:The patient had no relevant past history.
Personal and family history
Case 1:His brother is a carrier of the sameAPCgene mutation,and his father died at the age of 40 due to colorectal cancer.
Case 2:No significant personal or family history.
Physical examination upon admission
Case 1:Unremarkable.
Case 2:A clinical examination revealed a large,palpable abdominal mass.
Laboratory examinations
Case 1:CEA,CA 19-9,and alpha-fetoprotein were negative.
Case 2:CEA,CA 19-9,neuron-specific enolase,Chromogranin A and alphafetoprotein were negative.
Imaging examinations
Case 1:Computed tomography (CT) revealed a hypodense mass measuring 5 cm in the head of the pancreas.F-18 fluorodeoxyglucose positron emission tomography CT(18-FDG PET-CT) showed a hypermetabolic lesion.There was no evidence of metastatic disease after a complete examination.
Case 2:CT indicated a very large,low-density tumour involving most of the pancreas with a multicystic component compressing the surrounding organs,without evidence of metastatic disease.No pathologic deposits were found by somatostatin-analogue scintigraphy.
FINAL DIAGNOSIS
Case 1
Pathological examination of surgical specimens revealed PACC with positive retroperitoneal surgical margin (R1),vascular and perineural invasion and regional lymph node negativity.
Case 2
Histologic examination of surgical specimens revealed PACC with a neuroendocrine component < 25% with negative regional lymph nodes.
TREATMENT
Case 1
Considering the lack of evidence of distant metastases based on CT,the patient underwent a pylorus-preserving pancreaticoduodenectomy in October 2007,and the histopathological examination revealed PACC in the head of the pancreas measuring 5 cm in diameter,a positive retroperitoneal surgical margin (R1),vascular and perineural invasion and regional lymph node negativity (pT3N0Mx,AJCC 8th edition).Due to his slow recovery after surgery,which was characterized by a bilioenteric fistula,no adjuvant chemotherapy or radiotherapy was administered,and the patient started a follow-up programme.He remained disease-free until August 2009,when CT and 18-FDG-PET-CT showed two hepatic lesions in segments II and VII.The lesion in segment II was biopsied and was demonstrated to be PACC metastasis(Figure 1A).Considering the lack of evidence in the literature,a decision was made to use a first-line treatment that was currently administered to PDAC patients.He was treated with gemcitabine and oxaliplatin (gemcitabine 1000 mg/m2plus oxaliplatin 100 mg/m2in a 14-d cycle).However,the first radiologic assessment after six courses of therapy demonstrated an increase in the diameter of the previously reported metastases (Figure 1B) and the appearance of new small lesions.In January 2010,the chemotherapy regimen was switched to gemcitabine plus capecitabine (gemcitabine 1000 mg/m2on days 1 and 8 and capecitabine 1300 mg/m2for 14 d).Except for neutropoenia (G3) and anaemia (G2),the treatment was well tolerated and was administered for a total of 22 cycles until April 2012;the patient achieved a partial response,and only the lesion localized to segment II remained detectable by CT(Figure 1C).This lesion was treated in June 2012 with RFA without any complications(Figure 1D).The patient was then treated with another four cycles of gemcitabine plus capecitabine until November 2012,when he started a follow-up programme.In March 2013,both CT and 18-FDG PET-CT showed a hepatic lesion highly suspicious of relapse,and the patient restarted treatment with gemcitabine plus capecitabine,achieving a complete response according to 18-FDG PET-CT and CT after three cycles.Considering the absence of any sign of disease and the long-term treatment,chemotherapy was stopped.Since June 2013,there have been no signs of tumour relapse.
Case 2
Considering the relevant symptoms caused by the mass and the lack of evidence of distant metastases by CT,in January 2009,the patient was treated with total pancreatectomy,total gastrectomy,splenectomy,extended right hemicolectomy and left adrenalectomy.Pathology revealed a PACC with a neuroendocrine component <25% in the pancreas,measuring 20 cm in diameter with negative regional lymph nodes (pT3N0Mx,AJCC 8th edition).A postoperative CT showed two hepatic metastases at segments I and V (Figure 2A).He was started on treatment with gemcitabine plus oxaliplatin and achieved stable disease for 27 wk until October 2009.Due to peripheral neuropathy (oxaliplatin-related neurotoxicity),the patient was treated with gemcitabine plus capecitabine for eight cycles and achieved a partial response.Considering the long-term disease control,RFA was performed for the remaining hepatic metastasis at segment I in September 2010,and another eight cycles of gemcitabine plus capecitabine were administered until July 2011 (Figure 2B).The patient remained disease-free until June 2012,when both CT and 18-FDG-PET-CT indicated peritoneal relapse (Figure 2C).Treatment with gemcitabine plus capecitabine was restarted,but after four cycles,progressive disease in the peritoneum was documented.In November 2012,therapy was switched to capecitabine plus irinotecan (irinotecan 200 mg/m2on day 1 and capecitabine 2000 mg/m2on days 1 to 15 every 21 d),leading to good disease control for nearly two years.Twenty cycles were administered,with a considerable reduction in 18F-FDG uptake (a standardized uptake value of 2.3vs4.8) and stable disease based on CT.In November 2014,CT showed progression in the peritoneum;we performed a biopsy of a peritoneal nodule,and pathology confirmed the initial diagnosis of PACC.Considering both the lack of evidence in the literature in favour of other treatments and the long time since the last administration of gemcitabine plus capecitabine,this treatment was reintroduced.However,this systemic treatment caused severe myelotoxicity after four cycles,and the patient was thus administered only metronomic capecitabine until July 2015,when chemotherapy was stopped due to persistent anaemia and thrombocytopaenia.CT was performed in December 2015 and documented further progressive disease in the peritoneum and new liver metastases.The patient died in March 2016,seven years after the first relapse.
to crash in Russia,killing all 71 people on board,investigatorssay.
OUTCOME AND FOLLOW-UP
Case 1
Since June 2013,there have been no signs of tumour relapse.
Case 2
CT was performed in December 2015 and documented further progressive disease in the peritoneum and new liver metastases.The patient died in March 2016,seven years after the first relapse.
DISCUSSION

Figure1 Computed tomography evaluation of Case 1.
PACC is a rare tumour accounting for approximately 1% of all exocrine pancreatic neoplasms and mostly occurs in late adulthood,with a peak incidence in the sixth decade of life and a male to female ratio of 3.6:1[3].PACC often has a large size at detection,with a diameter > 10 cm;nevertheless,most patients have no specific symptoms,such as weight loss (52%),abdominal pain (32%),nausea and vomiting(20%),melena (12%),weakness,anorexia or diarrhoea (8%)[5].There are some remarkable differences in the driver mutations and patterns of genetic alterations in PACC compared to PDAC.The patient described in case 1 was affected by familial adenomatous polyposis,presenting theAPCgene variant c.847C > T.Alterations in APC are frequently involved in the pathogenesis of PACC;indeed,alterations in APC,mainly represented by loss (48%) and methylation (56%),are observed in approximately one-half of PACC patients;in contrast,mutations,such as in our patient,are less frequently observed (7%)[12].For this reason,it is not surprising that people with familial adenomatous polyposis appear to be particularly predisposed to developing PACC[13],although there are only a few cases reported in the literature of patients with familial adenomatous polyposis affected by PACC[14].Studies have reported lower rates of EGFR and KRAS mutations in PACC than in PDAC,though more than 70% of PACCs display a reduction in or loss of DCC expression based on immunohistochemistry.This appears to be an early genetic change that is different from what occurs in PDAC[15].Furthermore,the differences in genetic alterations between PACC and PDAC are reflected in the different prognoses.For example,in a retrospective study involving 865 patients with PACC,the five-year stage-specific survival was significantly better for resected PACC than PDAC (stage I:52.4%vs28.4%;II:40.2%vs9.8%;III:22.8%vs6.8%;and IV:17.2%vs2.8%)[4].Nevertheless,approximately half of these patients have metastatic disease at diagnosis;the liver is the most common site of metastasis,and a high rate of disease recurrence after surgery has been documented by several studies and ranges from 50% (median follow-up 27.1 mo) to 100%,with recurrence mainly located in the liver[5,6,16].
With this high rate of disease recurrence and a relatively less aggressive biological behaviour than PDAC,some authors have suggested that aggressive multimodal treatments such as multiple lines of chemotherapy combined with loco-regional techniques or reiterative surgery should be considered for patients with advanced or recurrent disease,as overall survival might improve[16,17].Hartwiget al[18]compared the long-term survival of six patients with limited metastatic disease (3 patients with synchronous hepatic metastases,1 patient with synchronous omental metastases and 2 patients with metachronous liver metastases) who underwent both primary and metastatic lesion resection with that of nonmetastatic patients,and there were no differences between the two groups.Other promising survival outcomes have been reported in some case series and case reports for patients who underwent an aggressive surgical approach[19-22].

Figure2 Computed tomography evaluation of Case 2.
RFA is based on protein denaturation with thermal coagulation caused by electrodes that are directly inserted into the centre of the tumour.It is a wellestablished treatment for hepatocellular carcinoma and represents a good alternative to surgery for colorectal and NET liver metastases[8,10];however,there are only a few reports about RFA for the treatment of metastatic PACC (Table 1).As an example,Armstronget al[23]reported a survival of over five years for metastatic PACC treated with multiple RFAs,cryotherapy,stereotactic radiosurgery and several lines of chemotherapy based on genomic profiling and cell line development.In addition,a case series of Butturiniet al[16]described a patient with recurrent PACC in the liver 28 mo after surgery;the patient was not suitable for surgical resection and was treated with chemotherapy (gemcitabine,oxaliplatin and capecitabine),RFA and chemoembolization,achieving an overall survival of 45 mo.Cananziet al[24]described an 11-year survival outcome of a patient with PACC who had liver metastasis and was treated with reiterative surgery,RFA and multiple lines of chemotherapy.Additionally,a patient who was treated with radiotherapy for primary tumour and RFA for hepatic metastases after responding well to gemcitabine plus oxaliplatin was reported by Béchadeet al[25].However,the follow-up was too brief to draw conclusions.
In contrast to previously reported cases,our patients were treated with only chemotherapy and RFA,without other local ablative therapies or reiterative surgery.In addition,our patients presented resectable disease at diagnosis,whereas most of the previously reported patients had metastasis at diagnosis.For our patients,the decision to apply RFA was made based on the oligometastatic nature of the disease and the good response to chemotherapy.For cases 1 and 2,one liver metastasis was treated with RFA,resulting in a disease-free survival of 9 and 21 mo,respectively.No relevant complications or recurrence of the treated metastases occurred.In both patients,chemotherapy was administered after RFA.We believe that this case study may help to obtain a better understanding of the real impact of local ablative therapies such as RFA for this rare disease.Nevertheless,a limitation of this report is the small number of cases,which was due to the rarity of PACCs.For this reason,it is impossible to offer strong recommendations.
Due to the very low incidence of this disease,there are no prospective studies focusing on chemotherapy for PACC,and data are available from only case series and case reports;making it is unclear what is the most appropriate first-line chemotherapy regimen.Nevertheless,combination fluoropyrimidine-based chemotherapies appear to be the best choice,as they are associated with higher rates of disease control than gemcitabine-based chemotherapies,as shown in a systematic review by Glazeret al[26].Additionally,platinum-based chemotherapy shows promising results in terms of overall survival.In a retrospective study by Brunettiet al[27],which included 23 PACCpatients treated with chemotherapy,10 of 12 patients who had an overall survival equal to or longer than the median reported overall survival were treated with platinum-based chemotherapy.Furthermore,according to Yooet al[28],oxaliplatincontaining regimens may have improved activity against PACC than gemcitabine.The activity of platinum salts may be explained by the fact that approximately half of PACC patients (45%) have inactivating genomic alterations in DNA repair genes and that BRCA2 mutations are detected in 20% of PACC patients[29].No data support the activity of gemcitabine alone,and promising results were not obtained with the combination of gemcitabine plus nab-paclitaxel[20,27].Our findings are in line with previous studies that showed the efficacy of fluoropyrimidine-based chemotherapy.Both patients obtained a partial response to gemcitabine plus capecitabine,and in case 1,we also observed a complete response to the treatment of the second relapse.In addition,patient 2 was treated with capecitabine plus irinotecan as a third-line therapy and achieved stable disease for nearly two years.

Table1 Overview of case reports and case series with metastases of pancreatic acinar cell carcinoma treated with radiofrequency ablation
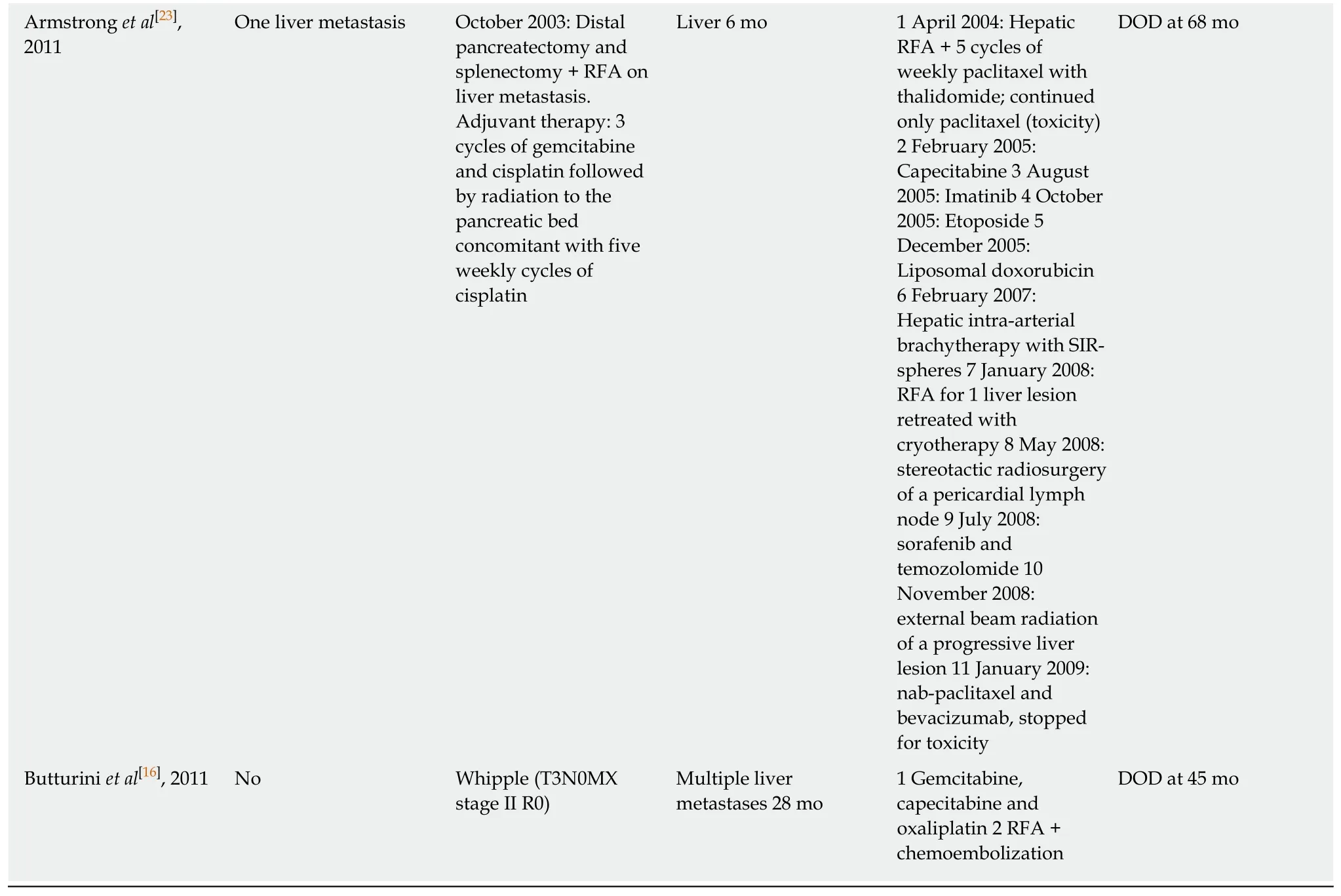
DOD:Dead of disease;RFA:Radiofrequency ablation;GEMOX:Gemcitabine,oxaliplatin;PD:Progressive disease.
CONCLUSION
We report two cases of long-term PACC survivors who were effectively treated with RFA in addition to fluoropyrimidine-based chemotherapy.Our cases highlight the different biological behaviour of PACC and PDAC and the importance of multidisciplinary treatment involving local ablative therapies for metastatic PACC.As previously demonstrated in the treatment of liver metastases of other types of cancers,we suggest that RFA should also be considered for PACC patients and that it may improve the prognosis of oligometastatic PACCs,which are chemo-responsive.
 World Journal of Clinical Cases2020年7期
World Journal of Clinical Cases2020年7期
- World Journal of Clinical Cases的其它文章
- CD56+ lymphoepithelioma-like carcinoma of the lung:A case report and literature review
- Systemic treatment for severe concentrated sulfuric acid burns in an adult male at high altitude:A case report
- Clinical effects of apatinib mesylate for treatment of multiple brain micrometastases:Two case reports
- Disseminated histoplasmosis in primary Sj?gren syndrome:A case report
- Severe venous thromboembolism in the puerperal period caused by thrombosis:A case report
- Multiple neurofibromas plus fibrosarcoma with familial NF1 pathogenicity:A case report