Hypertransaminasemia in the course of infection with SARS-CoV-2:Incidence and pathogenetic hypothesis
2020-05-14 01:53:54
World Journal of Clinical Cases 2020年8期
Maddalena Zippi, Giuseppe Occhigrossi, Unit of Gastroenterology and Digestive Endoscopy,Sandro Pertini Hospital, Rome 00157, Italy
Sirio Fiorino, Unit of Internal Medicine, Maggiore Hospital, Local Health Unit of Bologna,Bologna 40133, Italy
Wandong Hong, Department of Gastroenterology and Hepatology, First Affiliated Hospital of Wenzhou Medical University, Wenzhou 325000, Zhejiang Province, China
Abstract
In patients infected with severe acute respiratory syndrome coronavirus 2, the respiratory symptoms, such as fever, cough and dyspnea, are the most frequent clinical manifestations. These patients may also present with less well-defined symptoms like diarrhea, nausea, vomiting and/or abdominal discomfort both at the time of diagnosis and during the clinical course. In a few cases, these symptoms may also present before the appearance of respiratory symptoms. To penetrate the body, Severe acute respiratory syndrome coronavirus 2 uses ACE2 receptors, which are present not only in respiratory epithelium but also in gastrointestinal mucosa and liver cholangiocytes. In several cases, viral RNA is detectable in the stool of patients with coronavirus disease 2019 (COVID-19). The liver damage seems to show a multifactorial origin. About 2%-11% of patients with COVID-19 have known underlying hepatic pathologies. In 14%-53% of COVID-19 cases, there is an alteration of the indices of liver cytolysis and is more frequently observed in severe forms of COVID-19, especially during hospitalization.
Key words: Coronavirus; COVID-19; Hypertransaminasemia; Liver; Meta-analysis;SARS-CoV-2
INTRODUCTION
As of December 2019, a viral infection defined as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), caused by the pathogen of coronavirus disease 2019(COVID-19), belonging to the Coronavirus family, has developed suddenly and has had and has a strong impact worldwide[1]. This virus is similar to other two preceding coronavirus sharing 79% of its genome with those of the 2003 severe acute respiratory syndrome (SARS-CoV) and 50% with those of the 2012 Middle Eastern respiratory syndrome (MERS-CoV)[2]. All these viruses are able to cause liver damage, in addition to the well-known respiratory manifestations[2]. In a recent Comment, Zhanget al[3]have analyzed the effects of the virus on liver and concluded that this pathogen can alter liver enzymes [alanine aminotransferase (ALT) and aspartate aminotransferase(AST)] in 14%-53% of cases, SARS-CoV-2 and as such an infection is present in 2%-11% of patients with known hepatic pathologies (chronic viral hepatitis, nonalcoholic fatty liver disease, alcoholic hepatitis, immune-mediated liver disease).
The aim of this mini-review is to identify those studies who have considered liver involvement, especially hypertransaminasemia that occurred during COVID-19 infection, by searching through MEDLINE/PubMed and Google Scholar. In particular, the following keywords were searched: “liver”, “SARS-CoV-2”, “COVID-19”, “transaminases”, “AST”, and “ALT”. We would like to emphasize that we used updated data at the time of submission of the present work, as these are continuously being updated.
PATHOGENETIC HYPOTHESIS
Hepatic involvement due to a predominant respiratory virosis is unclear. Liver damage appears to be of multifactorial origin. (1) Direct damage: Caused by the virus itself as it can bind to ACE-2 receptors, which are expressed in lung, kidney, and gastrointestinal tract[4,5]. The ACE-2 receptors are particularly present in endothelial cells of the liver[6]; (2) Intestinal translocation: It has been observed how about 2%-10%of affected patients have diarrhea, and SARS-CoV-2 RNA has been detected both in stool as well as blood samples. This could lead to a greater “translocation” from the intestinal lumen[3,7-9]. In fact, we know that gut integrity, especially during abdominal sepsis, may be altered, leading to increased cellular apoptosis with subsequent altered barrier permeability[10,11]; (3) Drug hepatotoxicity: In their study, Zhanget al[3]have observed that liver function tended to alter both during and after the ongoing infection (COVID-19); they hypothesized a “residual effect” on the liver due to the drugs taken to counteract the infection. As underlined by Rismanbafet al[12], we must also consider the side effects of the therapies used in virosis on the liver. In their Letter, the authors emphasized how the currently used drugs, like Oseltamivir,Lopinavir, Ritonavir, Ribavirin, and Chloroquine Phosphate or Hydroxy Chloroquine Sulfate, are all metabolized in the liver[12]. In a recent multicenter retrospective study,Liuet al[13]analyzed 32 patients, of which 28 (87.5%) had a mild or moderate disease and 4 (12.5%) had severe one, observing how liver damage was prominent in severe patients under medical therapy; and (4) Immune-mediated inflammation: the hepatic involvement that occurs during this infection must be considered as it may cause a“cytokine storm”, especially, in severe forms of COVID-19[14]. In this patient cohort,increased levels of interleukin (IL)-2, IL-7, interferon-γ and tumor necrosis factor-α were observed[15]. Adhikariet al[16]reviewing 65 research articles found how a surgery history before admission for Covid-19 was one of the factors that make people more likely to contract the infection. In fact, surgical stress can exacerbate “cytokine storm”and the COVID-19 disease progression (Figure 1).
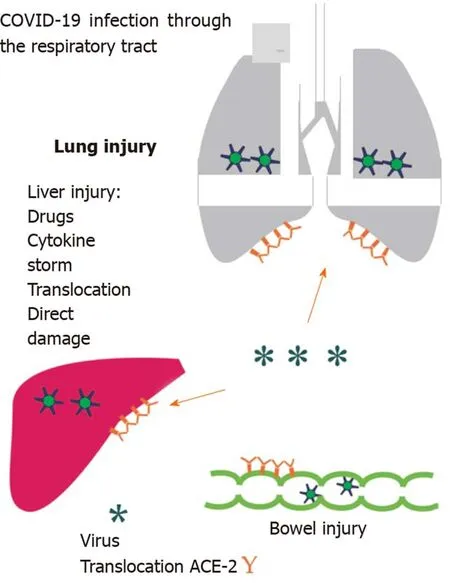
Figure 1 Possible mechanisms underlying the liver damage. COVID-19: Coronavirus disease 2019.
AVAILABLE STUDIES
To date, looking in the available literature, we could identify 16 papers relating to the evaluation of hepatic impairment in SARS-CoV-2 patients. These results are available in Table 1.
In a similar study, not included in Table 1, it is reported that out of 128 patients affected by COVID-19, there was an increase in transaminases only in severe cases[32].Guanet al[17]further analyzed in a subgroup the increase in transaminases based on the degree of disease severity. They reported elevated levels of AST in 39.4% (56/142 patients) patients with severe disease compared with 18.2% (112/615 patients)patients with mild/moderate disease. Also, the levels of ALT were higher in the severe form (28.1%vs19.8% of mild/moderate conditions)[17]. Huanget al[18]reported an increase in AST level in 62% of 13 patients recovered in Intensive Care Unit. A further confirmation comes from the work of Shiet al[21], in which patients with pulmonary involvement, assessed by computed tomography, showed a significant increase in AST level compared to those suffering from a subclinical form. A final consideration is given by Yanget al[23], who reported no significant difference in increased transaminase between survivors (30%) and non-survivors (28%).
STATISTICAL ANALYSIS
We used forest plots for estimating pooled effect sizes and the effect of each study,with 95%CI, to provide a visual summary of the data. Heterogeneity among studies was evaluated by Cochran Q-test and I-squared index, with I2 values above 75% as thresholds for high heterogeneity. When heterogeneity was present, we used a random effects model (DerSimonian-Laird model); otherwise, a fixed effects model(Mantel-Haenszel) used to compute overall effects[33]. A total of 9 studies were enrolled in the current pooled analysis. The incidence of liver injury in individual studies ranged from 12% to 78%. Due to extensive heterogeneity between studies (I-squared = 96.6%), a random effect model was used. The pooled incidence of liver injury in patients with COVID-29 infection was 0.36 (95%CI: 0.21-0.52) (P< 0.001)(Figure 2).
CONCLUSION
Hepatic involvement during SARS-CoV-2 infection is not uncommon. Altered transaminases are most frequently reported in the available works. This finding does not support the hypothesis of a hypoxic hepatitis, as their elevated levels are present also in not critically ill patients, especially in those ones without mechanicalventilation[34]. The increase in cytolysis indices may be due to several causes, including the antiviral drugs. In this regard, the histological description of liver biopsies performed on a 50-year-old subject who died owing to COVID-19 is interesting. It shows a mild lobular and portal activity associated with a moderate microvascular steatosis, as to indicate how liver damage may have been caused either directly by the virus or by the administered drugs[35]. The increase in transaminases observed in the reviewed works could also be partly due to the increased risk of toxicity when the optimal therapeutic dose is reached. As the etiology of this phenomenon can be traced back to various factors, currently there is no therapeutic approach or management for it. What can be deduced, from the available literature to date, is keeping monitoring the level of transaminases during hospitalization. As underlined by Al-Busafiet al[36],the serum alanine aminotransferase and aspartate aminotransferase are the best markers of hepatocellular injury and their highest levels tend to indicate a more severe liver damage. It’s known that drugs with their respective dosages play a fundamental role in hepatotoxicity, especially in patients undergoing polytherapy. In a “normal” situation, the European Association for the Study of the Liver recommends to discontinue the involved agent, but in this type of patient it is not possible to suspend the antiviral medications[37]. Limited data are available about liver involvement in infected children with COVID-19, especially for infected infants. Cuiet al[38]described a case of a 55-d-old case with COVID-19 in China who presented with altered hepatic function during hospitalization. Recently, Sunet al[39]described the laboratory findings in 8 severe patients in the ages between 2 mo and 15 years,including 6 males and 2 females. Their results showed AST in norm and ALT increased in 4 cases (50%).
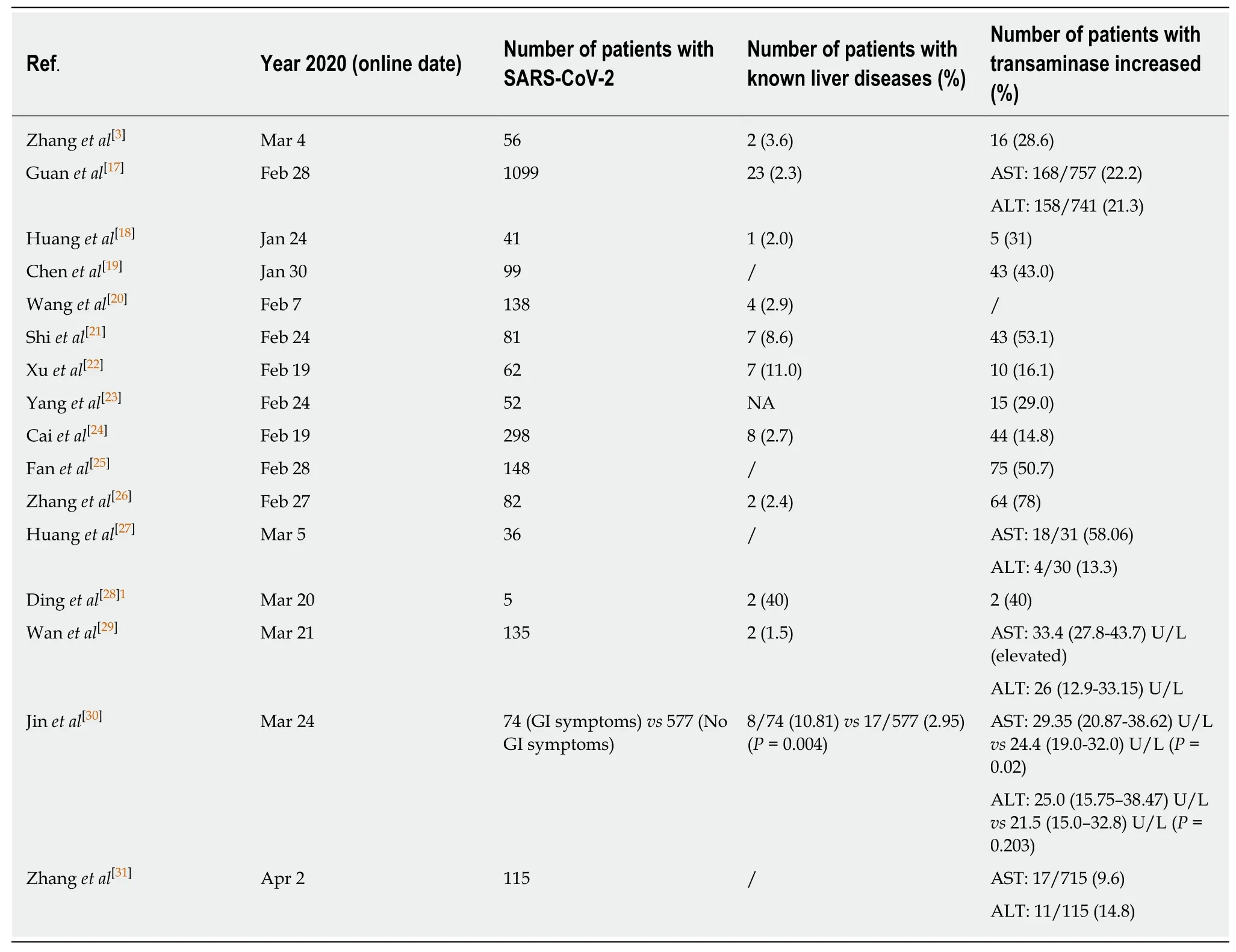
Table 1 Studies considering liver function in patient with severe acute respiratory syndrome coronavirus 2
In conclusion, hypertransaminasemia present in these patients may be due to several reasons. Further studies will be needed to understand the main cause of this phenomenon in order to guide the best treatment.
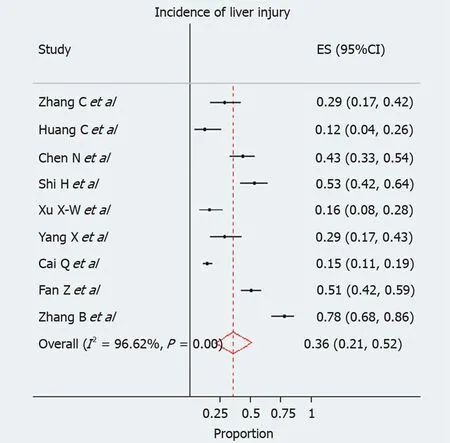
Figure 2 Meta-analysis of the studies focusing on hypertransaminasemia in coronavirus disease 2019 patients.
 World Journal of Clinical Cases2020年8期
World Journal of Clinical Cases2020年8期
- World Journal of Clinical Cases的其它文章
- Clinicopathological differences and correlations between right and left colon cancer
- Bedside score predicting retained common bile duct stone in acute biliary pancreatitis
- Stability and infectivity of coronaviruses in inanimate environments
- Status, challenges, and future prospects of stem cell therapy in pelvic floor disorders
- Unusual presentation of congenital radioulnar synostosis with osteoporosis, fragility fracture and nonunion: A case report and review of literature
- Predictive factors for central lymph node metastases in papillary thyroid microcarcinoma