Suicide attempt using potassium tablets for congenital chloride diarrhea: A case report
2020-05-14 01:54:00ShigeoIijima
World Journal of Clinical Cases 2020年8期
Shigeo Iijima
Shigeo Iijima, Department of Pediatrics, Hamamatsu University School of Medicine,Hamamatsu 4313192, Japan
Abstract
BACKGROUND
Congenital chloride diarrhea (CCD) is a rare inherited disorder of intestinal electrolyte transport that results in a large wastage of electrolytes and water.Advances in substitution therapy using sodium chloride (NaCl) and potassium chloride (KCl) have dramatically improved survival for patients with CCD. Slowrelease KCl is widely prescribed as a potassium supplement; however, it has also occasionally been used in suicide attempts, as potassium poisoning can generate life-threatening hyperkalemia.
CASE SUMMARY
A 26-year-old female presented to the emergency department (ED) with selfpoisoning, having taken 30 tablets of slow-release KCl (total: 240 mmol potassium) following an auditory hallucination. The patient had been undergoing substitution therapy with NaCl and KCl for CCD and been followed up in the pediatric department. One month prior, she developed insomnia and anxiety and had consulted a psychiatrist. At the ED, although her general condition was good, she appeared agitated. Her serum potassium level was 7.0 mmol/L, indicating hyperkalemia, and electrocardiographic changes showed tenting of the T-waves. She responded to the administration of calcium gluconate, sodium bicarbonate, and insulin with glucose, and the serum potassium level improved. Finally, she was diagnosed with schizophrenia.
CONCLUSION
In CCD management, physicians should pay careful attention to patients’extraintestinal issues, including psychological disorders that may emerge in adulthood.
Key words: Congenital chloride diarrhea; Substitution therapy; Suicide; Potassium overdose; Schizophrenia; Case report
INTRODUCTION
Congenital chloride diarrhea (CCD, OMIM 214700) is a rare autosomal recessive disease of impairment in intestinal Cl?/HCO3?exchange, due to mutations in the solute carrier family 26 member 3 (SLC26A3, OMIM 126650) gene, and is characterized by persistent, life-long, watery diarrhea with a high fecal chloride concentration (> 90 mmol/L)[1]. Worldwide, more than 250 cases of CCD have been reported[2]. Without treatment, most children die in infancy or survive with severely delayed psychomotor development. Advances in substitution therapy with sodium chloride (NaCl) and potassium chloride (KCl) have dramatically improved the survival of these patients, and the long-term prognosis of appropriately managed CCD has been reported to be favorable[3].
Although KCl is extensively used to supplement potassium as a therapeutic modality, potassium administration is also known to be a means in suicide/homicide attempts or in lethal procedures for state-sanctioned capital punishment. Potassium poisoning can cause life-threatening hyperkalemia, as harmful effects on the electric activity of the heart are the most important consequences of hyperkalemia. When serum potassium levels exceed 7 mmol/L, remarkable arrhythmic changes can be observed using electrocardiography. With serum potassium levels ≥ 8 mmol/L,sudden cardiac arrest can occur[4].
We encountered an adult patient with CCD who had attempted suicide through ingesting a large number of KCl tablets that had been prescribed for substitution therapy. No previous studies have focused on mental or psychiatric disorders involving patients with CCD, and no studies have reported the challenges facing patients with CCD related to life-long substitution therapy.
CASE PRESENTATION
Chief complaints
A 26-year-old female presented to the emergency department (ED) complaining of epigastric discomfort and nausea.
History of present illness
One month prior, the patient had developed insomnia and anxiety due to domestic difficulties. She consulted a psychiatrist and was prescribed anti-anxiety and hypnotic medications relevant to a diagnosis of adjustment disorders. On the day of the ED visit, she had experienced an auditory hallucination and had ingested 30 tablets of slow-release KCl (each tablet containing 8mmol potassium) in a suicide attempt. She then called her father because of the epigastric discomfort and nausea and he transported her to the ED four hours after ingestion.
History of past illness
At 16 months old, this patient was diagnosed with CCD based on hypochloremic alkalosis, hyponatremia, hypokalemia with increased plasma renin and aldosterone levels, and high fecal Cl?. In this case, because repeated sweat testing showed normal Cl?concentration and because pulmonary illness did not develop during her clinical course, we are sure that the patient did not have cystic fibrosis. She has undergone substitution therapy with NaCl and KCl. On follow-up, watery diarrhea persisted, but she developed normally. In adulthood, she married and produced a healthy child after an uneventful pregnancy at the age of 24 years. Subsequently, the patient continued to visit the pediatric outpatient clinic four times a year. Her usual serum electrolyte concentrations were as follows: Na+: 140-143 mmol/L; K+: 2.8-3.4 mmol/L,and Cl?: 96-100 mmol/L, with a daily substitution of 48 mmol slow-release KCl. In this case, genetic diagnosis was considered; however, the patient did not approve of this diagnostic method and therefore, it was not performed.
Personal and family history
This patient was born with polyhydramnios at 36 wk gestation and weighing 2550 g.Both her parents are healthy but consanguineous. Her grandmother's brother died immediately after birth; however, the cause of death was unclear.
Physical examination
The patient was agitated, but her general condition was good. Her pulse rate was 105 beats/min and her blood pressure was 101/77 mmHg.
Laboratory examinations
Initial laboratory blood test results were as follows: pH: 7.419; partial pressure of carbon dioxide (CO2): 30.8 mmHg; bicarbonate (HCO3?): 20.0 mmol/L; base excess(BE): -5.0; Na+: 139 mmol/L; K+: 7.0 mmol/L; Cl?: 105 mmol/L; urea nitrogen: 7.3 mg/dL, and creatinine: 0.52 mg/dL.
Imaging examinations
Electrocardiographic changes of hyperkalemia were observed, with tenting of T-waves and smaller P-waves.
FINAL DIAGNOSIS
Hyperkalemia due to self-poisoning with slow-release KCl tablets in a suicide attempt.
TREATMENT
The hyperkalemia was treated with an intravenous injection of 8.5% calcium gluconate (20 mL) and 8.4% sodium bicarbonate (40 mL), and insulin with glucose infusion therapy (5 units of regular insulin (Humulin-R) and 20 g of glucose/hour)was started. The patient responded to treatment and, at six hours post-initiation of treatment, the serum potassium level had corrected to 4.0 mmol/L.
OUTCOME AND FOLLOW-UP
The patient was referred to the psychiatry department and was diagnosed with schizophrenia. She was subsequently admitted to an inpatient unit for treatment of her acute presentation with atypical antipsychotics (aripiprazole and risperidone),and she showed significant improvement. Concerning her present CCD management,the substitution therapy with slow-release KCl has been continued with very careful monitoring of this patient because of the lack of an alternative.
DISCUSSION
This is the first report focusing on mental or psychiatric disorders involving patients with CCD and the challenges facing these patients related to life-long substitution therapy. Despite persistent diarrhea, it has been reported that most patients with CCD appear to adjust to their condition and experience only minimal social disadvantage[5].Moreover, ≥ 90% of patients with CCD are reported to consider their general health as excellent or good[3]. The patient presented in this report had acceptable growth,normal development, an uneventful pregnancy, and the delivery of a healthy child.Nevertheless, she had attempted suicide and was diagnosed with schizophrenia. The relationship between CCD and mental or psychiatric disorders remains unclear.Episodes of dehydration can result in mental and psychomotor impairment. In fact,this patient had often been hospitalized with dehydration due to acute gastroenteritis.In a clinical analysis of 21 Finnish patients with CCD published in 1977[6], one patient was reported to have had severe psychological difficulties, the details of which are not known, and the authors in that report indicated that those psychological issues were apparently unrelated to CCD. A recently published nationwide study in Japan reported that 23% of children with CCD had a neurodevelopmental or neuropsychiatric disorder in terms of their long-term outcomes[7]; however, the prevalence of various psychiatric disorders such as depression and schizophrenia in adult patients has not been reported. It is likely that long-term clinical outcomes have neither been captured nor recorded consistently in a standardized manner. Some patients with CCD have been reported to have developed inflammatory bowel disease (IBD)[2,8]. In IBD, psychiatric comorbidity is well recognized[9], and one recent study found a higher incidence of schizophrenia in an IBD cohort compared to controls[10]. Furthermore, an increased risk of a suicide attempt or ideation has been noted as a concern in patients with IBD[11]. Schizophrenia is a very common form of mental illness and its onset is significantly influenced through environmental factors or stressors[12]. One study showed that 30% of patients with schizophrenia had attempted suicide at least once during their lifetime[13]. A systematic review exploring suicide risk in patients with schizophrenia suggested that the risk factors leading to suicide appeared mainly related to stress[14]. In CCD, soiling remains common at all ages and, in adulthood, minor soiling has been reported to occur at night when sleeping or during physical exertion[3]. In addition to stress from persistent diarrhea,patients with CCD who appear socially adjusted may come under considerable physical or social stress after gaining independence from their parents and taking responsibility for their own lives. Following the critical childhood period, most patients with CCD visit the outpatient clinic only once or twice a year for routine examinations and prescriptions[3]. Moreover, most patients with CCD have previously only been followed by a pediatrician[4], who may not be able to recognize or address psychological problems unique to adulthood. Challenges facing adult patients with CCD, including mental health issues, should be investigated in detail, and psychological counseling may be required to improve a patient’s quality of life.
Regarding the therapeutic management of CCD, substitution using NaCl and KCl involves physiological changes and normally has no side-effects[5]. However, an overdose of KCl can generate severe hyperkalemia, leading to serious sequelae.Although poisoning events using drugs and chemicals are common, reports of potassium poisoning, especially in regard to oral self-poisoning, are rare. There are no large case series concerning potassium overdoses in the medical literature. An extensive medical literature search revealed only 13 case reports involving a total of 19 patients having had slow-release potassium poisoning (Table 1)[4,15-26]. Cases involving fatalities and survivors have both been reported. According to those case reports, even in previously healthy patients, ingestion of more than 20 tablets of slowrelease potassium at once can cause severe hyperkalemia to develop over several hours, requiring intensive care. However, it takes a much smaller dose of ingested potassium to produce lethal toxicity in patients with compromised renal function than in those with normal renal function[19]. Although our patient had normal renal function, a relatively high incidence (28%) of chronic kidney disease was reported in a Finnish study of patients with CCD[2].
Therefore, when a patient with CCD develops a psychiatric disorder that may risk an attempt at suicide, other medication should be considered. However, therapeutic attempts to manage diarrhea using cholestyramine, omeprazole, and butyrate have not been as successful as hoped, suggesting that NaCl and KCl supplementation will continue to be more important than antidiarrheal therapy[1-3,7].
CONCLUSION
In patients with CCD, diarrhea is life-long and various extraintestinal issues may also emerge as patients become older unless an optimal radical therapy is established.Therefore, physicians need to pay careful attention not only to patients’ physical conditions but also to their mental health throughout their long-term follow-up, to ensure that any subsequent psychiatric disorders do not adversely affect CCD outcomes.
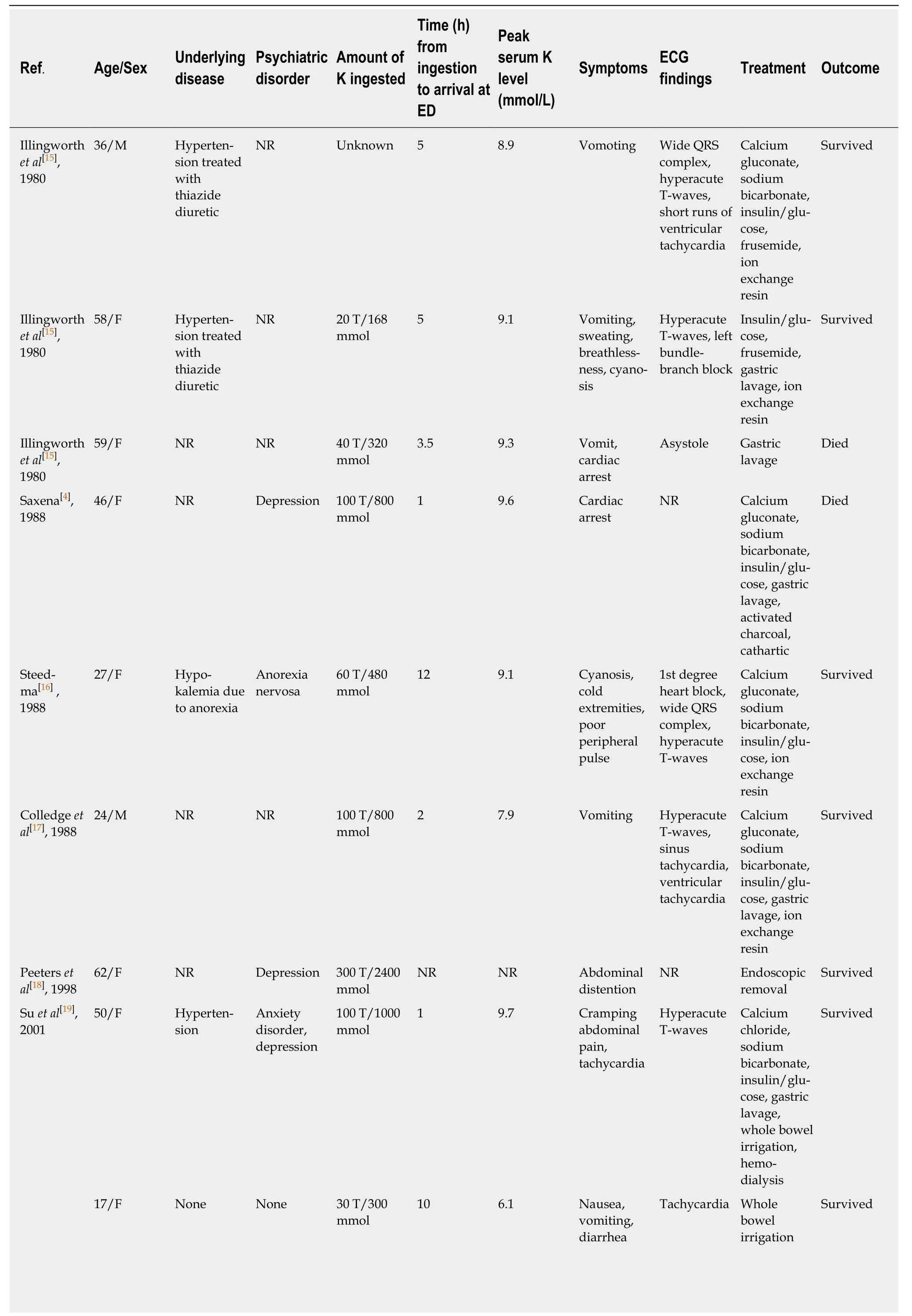
Table 1 Cases of suicidal poisonings associated with an oral intake of slow-release potassium chloride

W a n e t a l[20], 2 0 0 7 8 6/M H y p e r t e n-s i o n t r e a t e d w i t h t h i a z i d e d i u r e t i c D e m e n t i a 7 0 T/5 6 0 m m o l N R 6.8 U n k n o w n N o f e a t u r e o f h y p e r-k a l e m i a C a l c i u m g l u c o n a t e,s o d i u m b i c a r b o n a t e,i n s u l i n/g l u-c o s e S u r v i v e d H ? j e r e t a l[21], 2 0 0 8 2 8/F 1 U n k n o w n d i s e a s e w i t h p a c e m a k e r i n s i t u B o r d e r l i n e p e r s o n a l i t y d i s o r d e r 1 0 0 C/1 0 0 0 m m o l 3 9.2 C a r d i a c a r r e s t P a c e m a k e r c a p t u r e C a l c i u m g l u c o n a t e,s o d i u m b i c a r b o n a t e,i n s u l i n/g l u-c o s e, g a s t r i c l a v a g e,a c t i v a t e d c h a r c o a l, i o n e x c h a n g e r e s i n, h e m o-d i a l y s i s S u r v i v e d 2 8/F 1 U n k n o w n d i s e a s e w i t h p a c e m a k e r i n s i t u B o r d e r l i n e p e r s o n a l i t y d i s o r d e r 1 0 0 C/1 0 0 0 m m o l 1 6.9 C a r d i a c a r r e s t P a c e m a k e r r h y t h m C a l c i u m g l u c o n a t e,s o d i u m b i c a r b o n a t e,i n s u l i n/g l u-c o s e, g a s t r i c l a v a g e,a c t i v a t e d c h a r c o a l, i o n e x c h a n g e r e s i n S u r v i v e d 2 8/F 1 U n k n o w n d i s e a s e w i t h p a c e m a k e r i n s i t u B o r d e r l i n e p e r s o n a l i t y d i s o r d e r 7 0 C/7 0 0 m m o l 2.5 7.1 N R H y p e r a c u t e T-w a v e s S o d i u m b i c a r b o n a t e,i n s u l i n/g l u-c o s e, i o n e x c h a n g e r e s i n S u r v i v e d B o s s e e t a l[22], 2 0 1 1 5 6/F N R D e p r e s s i o n 6 0 T/4 8 0 m m o l 5 1 1 L e t h a r g y C o m p l e x s i n e-w a v e r h y t h m C a l c i u m g l u c o n a t e,s o d i u m b i c a r b o n a t e,i n s u l i n/g l u-c o s e S u r v i v e d G u n j a[23],2 0 1 1 4 2/F 2 N R B i p o l a r d i s o r d e r 4 0 T/3 2 0 m m o l 1.5 5.5 N R S i n u s t a c h y c a r d i a,t a l l T-w a v e s I n s u l i n,w h o l e b o w e l i r r i g a t i o n S u r v i v e d 4 2/F 2 N R B i p o l a r d i s o r d e r 1 0 0 T/8 0 0 m m o l 5 8.5 T a c h y c a r d i a S i n u s t a c h y c a r d i a,t a l l T-w a v e s C a l c i u m c h l o r i d e,s o d i u m b i c a r b o n a t e,i n s u l i n,h e m o-d i a l y s i s S u r v i v e d N i l s s o n e t a l[24], 2 0 1 2 3 0/F N R D e p r e s s i o n 3 0 0 T/3 0 0 0 m m o l 5 1 0.3 D r o w s i n e s s,d a z e S i n e-w a v e t a c h y c a r d i a C a l c i u m g l u c o n a t e,s o d i u m b i c a r b o n a t e,i n s u l i n/g l u-c o s e, g a s t r i c l a v a g e, i o n e x c h a n g e r e s i n, h e m o-d i a l y s i s,s u r g i c a l r e m o v a l S u r v i v e d G u i l l e r m o e t a l[25],2 0 1 4 4 2/F N R B o r d e r l i n e p e r s o n a l i t y d i s o r d e r 1 0 0 T/8 0 0 m m o l 2 3.9 S o m n o l e n c e S i n u s t a c h y c a r d i a G a s t r i c l a v a g e,a c t i v a t e d c h a r c o a l,e n d o s c o p i c r e m o v a l S u r v i v e d
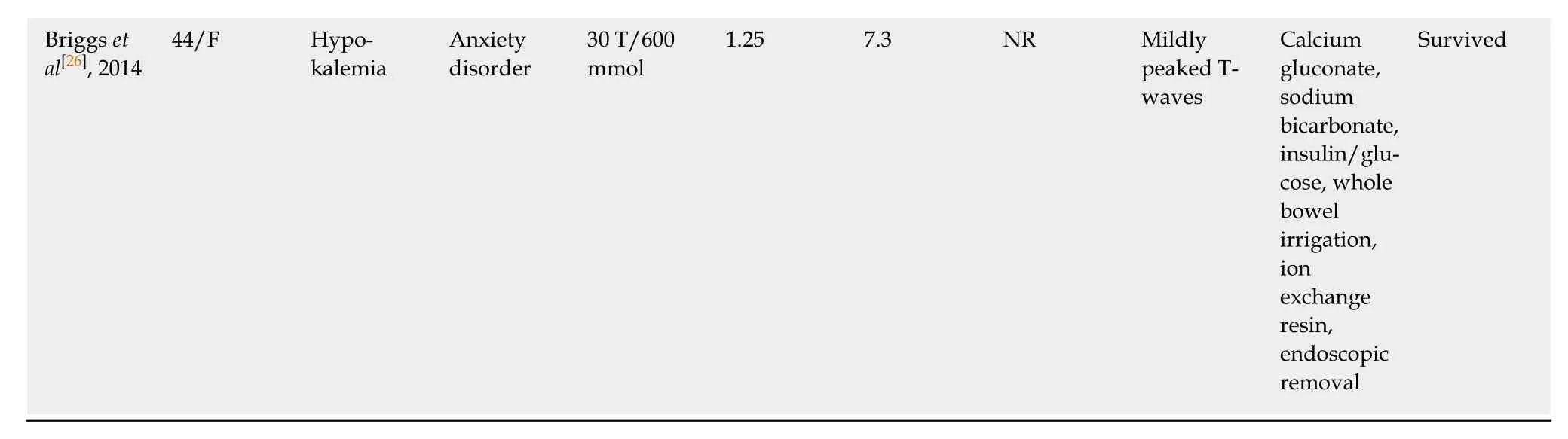
1,2: Same patient, respectively; C: Capsule; ECG: Electrocardiogram; ED: Emergency department; F: Female; K: Potassium; M: Male; NR: Not reported; T:Tablet.
 World Journal of Clinical Cases2020年8期
World Journal of Clinical Cases2020年8期
- World Journal of Clinical Cases的其它文章
- Clinicopathological differences and correlations between right and left colon cancer
- Bedside score predicting retained common bile duct stone in acute biliary pancreatitis
- Stability and infectivity of coronaviruses in inanimate environments
- Status, challenges, and future prospects of stem cell therapy in pelvic floor disorders
- Unusual presentation of congenital radioulnar synostosis with osteoporosis, fragility fracture and nonunion: A case report and review of literature
- Predictive factors for central lymph node metastases in papillary thyroid microcarcinoma