Primary cutaneous mantle cell lymphoma: Report of a rare case
2020-05-14 01:51:14
World Journal of Clinical Cases 2020年8期
Xiao-Dan Zheng, Yan-Lin Zhang, Jian-Lan Xie, Xiao-Ge Zhou, Department of Pathology, Beijing Friendship Hospital, Capital Medical University, Beijing 100050, China
Abstract
BACKGROUND
We describe the case of a 74-year-old man diagnosed with primary cutaneous mantle cell lymphoma (MCL), an extremely rare and controversial condition that is not included in the World Health Organization-European Organization for Research and Treatment of Cancer classification for cutaneous lymphomas.
CASE SUMMARY
The patient presented diffuse cutaneous erythematous plaques and nodules throughout the body. Skin lesions were biopsied and histopathological examination showed diffuse monomorphic lymphocyte infiltration in the dermal and subcutaneous layers, sparing the epidermis. Immunohistochemical staining revealed CD20, cyclin-D1, CD5, and SOX-11 expression. Fluorescence in situ hybridization showed CCND1/IGH gene rearrangement. Correct diagnosis of primary cutaneous MCL requires ensuring that no other parts are involved; these cases require close follow-up to monitor their possible progression to systemic disease and for treating relapsed cutaneous disease. In this case, positron emission tomography scanning and clinical staging revealed no systemic involvement, and follow-up examination at 20 mo after diagnosis showed no evidence of systemic disease. The prognosis of primary cutaneous MCL is relatively good. Our patient received six cycles of chemotherapy, and the cutaneous manifestations presented almost complete remission.
CONCLUSION Primary cutaneous MCL is rare, and its prognosis is relatively favorable.However, correct diagnosis is a prerequisite for proper treatment.
Key words: Primary; Cutaneous; Mantle cell lymphoma; Diagnosis; Treatment; Prognosis;Case report
INTRODUCTION
Mantle cell lymphoma (MCL) is a mature B-cell neoplasm characterized by uncontrolled proliferation of small to medium-sized lymphoid cells within the mantle zone[1]. More than 95% of cases of MCL show the CCND1 chromosomal translocation t(11;14)(q13;q32), which triggers cyclin D1 overexpression[2,3]. Lymph nodes are the most frequently involved sites. The spleen and bone marrow, with or without peripheral blood involvement, are also important sites of the disease. Other frequently involved extra-nodal sites include the gastrointestinal tract and Waldeyer’s ring.However, skin involvement in MCL is rare, and most cases occur due to secondary cutaneous dissemination by widespread disease[4-8]. Primary cutaneous MCL is even rarer, and mostly isolated cases have been documented previously and the majority of such patients typically present with systemic lymphoma in later stages[4,9-13]. The World Health Organization-European Organization for Research and Treatment of Cancer (WHO-EORTC) does not classify primary cutaneous MCL as a cutaneous lymphoma[14]. Here, we report a rare case of primary cutaneous MCL and describe its clinical, histopathological, immunohistochemical, and genetic features, as well as its treatment and prognosis.
CASE PRESENTATION
Chief complaints
Diffuse cutaneous erythematous plaques and nodules (Figure 1).
History of present illness
In May 2018, a 74-year-old man showed diffuse cutaneous erythematous plaques and nodules with irregular borders on the chest; the effect of anti-allergy treatment was not prominent.
History of past illness
The patient’s history of past illness was not remarkable.
Personal and family history
The patient’s father had a history of hypertension, and his mother had a history of breast cancer.
Physical examination upon admission
After the first examination, the number of cutaneous lesions increased progressively and involved the entire body, with diameters ranging from 0.5 to 1 cm. The patient’s overall physical condition was good, without B symptoms.
Laboratory examinations
Skin lesions on the trunk and scrotum were biopsied. Histopathological examination showed diffuse monomorphic lymphocyte infiltration in the dermal and subcutaneous layers, but not in the epidermis (Figure 2A and B). The lymphoid cells were mostly small to medium in size, with irregular nuclear contours (Figure 2C).

Figure 1 Clinical cutaneous features of this case. A: Diffuse, irregular cutaneous erythematous nodules and plaques on the trunk; B: Diffuse, irregular cutaneous erythematous nodules and plaques on the scrotum.
Immunohistochemistry (Figure 3) showed the following phenotypic characteristics:CD21 and CD23 staining displayed a broken follicular dendritic cell network; staining for other markers was as follows: Cyclin D1+, SOX11+, CD5+, CD20+, CD43+, BCL2+,BCL-6 scattered+, CD10-, LEF1-, CD56-, CD30-, CD2-, TIA1-, CD4-, CD8-, and Ki-67+.Tumor cells showed a proliferation index of approximately 20%.In situhybridization revealed the absence of EBER+tumor cells. Fluorescencein situhybridization (FISH)revealedCCND1/IGHgene rearrangement, a distinctive feature of the t(11;14)(q13;q32) chromosomal translocation (Figure 4). Altogether, these clinical phenotypes were consistent with the diagnosis of cutaneous MCL. The clinical data revealed no lymphadenopathy, bone marrow biopsy and peripheral blood examination were normal, and there was no spleen or liver involvement.
Imaging examinations
Positron emission tomography did not reveal systemic involvement.
FINAL DIAGNOSIS
Primary cutaneous MCL was the ultimate diagnosis.
TREATMENT
The patient received six cycles of rituximab, cyclophosphamide, doxorubicin,vincristine, and prednisolone (R-CHOP) chemotherapy.
OUTCOME AND FOLLOW-UP
The cutaneous manifestations presented almost complete remission without recurrence and progression.
The patient underwent a follow-up examination in January 2020, 20 mo after diagnosis, and no evidence of systemic disease was observed. The peripheral blood test results and bone marrow biopsy at this time were normal.
DISCUSSION
Skin involvement in MCL is very uncommon, accounting for 2%-6% of all cases[6].Cutaneous manifestations in MCL occur primarily in cases with systemic disease.Secondary skin involvement in MCL has been described in several studies, but primary cutaneous MCL has seldom been reported[4-13]. Indeed, the presence of primary cutaneous MCL is controversial. It is not included in the WHO-EORTC classification[14]and in the WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues[2]for cutaneous lymphomas. A primary cutaneous lymphoma following the WHO-EORTC definition[14], refers to a lymphoma that presents in the skin without extracutaneous disease during the process of diagnosis. Some studies[11,15]have pointed out that a conclusive diagnosis of primary cutaneous MCL can only be achieved if there are no extracutaneous lesions during 6 mo of clinical follow-up with adequate staging. Our patient showed no signs of extracutaneous lesions during the process of diagnosis and up to 20 mo after diagnosis.
A review of the literature reveals less than 50 reported cases of cutaneous MCL. Senet al[4]reported five cases of cutaneous MCL in 2002, Motegiet al[5]reviewed 17 cases of skin involvement in MCL in 2006, Wehkampet al[6]reported 14 cases in 2015, and Gruet al[7]reviewed ten cases in 2016. In addition, several case reports are available in literature[9,12,13]. Of these cases, only eight were thought to be primary cutaneous MCL,of which only five were found as clear cases of this condition[4,10-13]. The clinical features and follow-up information of these cases are summarized in Table 1. The lesions of the described cases were limited to the skin without systemic involvement.Our 74-year-old male patient presented diffuse cutaneous erythematous plaques and nodules.
Gruet al[7]reported that among the cases studied, they observed tumor cell infiltration into the dermis and subcutaneous tissue, with cell-free infiltration zone between the dermis and epidermis. The lymphocytes were mostly small to intermediate in size, with two of ten cases belonging to the blastoid variant. A previous study by Senet al[4]reported that most cases of cutaneous MCL had blastoid morphology and should be classified as blastoid variants. Recently, the largest case study on cutaneous MCL was conducted by Wehkampet al[6], who also found that all of their analyzed cases, except two, had blastoid morphology, and this type was considered extensively aggressive. The median survival of patients with classic histological features was 50 mo, whereas that for patients with blastoid morphology was 18 mo[16]. The five previously reported cases of primary cutaneous MCL showed that the tumor cell sizes were predominantly intermediate to large. However, our case showed a diffuse monomorphic small to medium-sized lymphocyte infiltration,which did not belong to the blastoid variant.
MCL refers to a B-cell lymphoma with characteristic immunohistochemical and molecular features such as the expression of cyclin D1 and t(11;14)(q13;q32)translocation. More than 95% of MCL cases express cyclin D1, whereas only a few cases are negative[17]. In MCL cases, SOX11 has emerged as an effective marker for diagnosis, with approximately 93%-95% of MCL cases being SOX11-positive.Combined immunohistochemistry tests for cyclin D1 and SOX11 exhibited a specificity and sensitivity of both 100% for diagnosing MCL[18]. Accurate differentiation of MCL from other cutaneous lymphomas is thus possible by using the characteristic immunohistochemical and genetic features. Our case was positive for both cyclin D1 and SOX11 and showed CCND1 translocation.
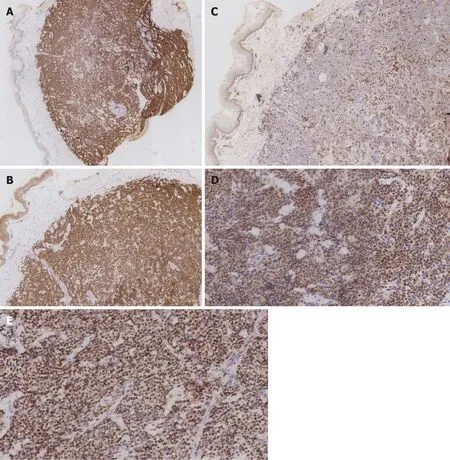
Figure 3 Immunohistochemical features of this case. A: Positivity for CD20 (×25); B: Positivity for CD5 (×50); C: Negativity for CD3 (×50); D: Positivity for cyclin D1 (×200); E: Positivity for SOX-11 (×200).
Skin involvement in MCL mainly appears in cases with systemic disease, which show invasive clinical progression and poor prognosis because of a high recurrence rate. According to previous studies[19,20], systemic chemotherapy is the standard treatment for MCL. However, the therapy of choice for primary cutaneous MCL is difficult to confirm as this condition has been not reported frequently; it is thus unclear whether the standard treatment for systemic disease can be applicable to a localized manifestation. Of the five previously reported cases of primary cutaneous MCL in addition to the current case, four patients received chemotherapy, whereas the remaining two showed isolated skin nodules and were treated with local radiotherapy or surgery. The prognoses of all six patients were relatively good, with nearly complete remission of the skin lesions after 6-31 mo of follow-up.
CONCLUSION
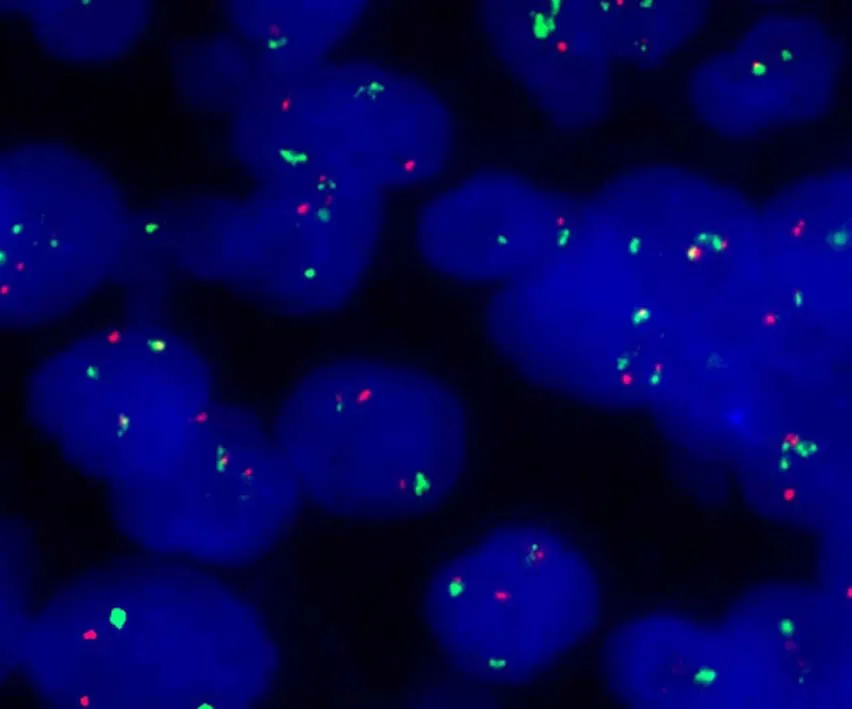
Figure 4 Fluorescence in situ hybridization analysis of this case. Fluorescence in situ hybridization analysis demonstrated fusion of the CCND1 gene locus (orange) and the immunoglobulin heavy chain gene locus (green).
In conclusion, primary cutaneous MCL is rare and has been the subject of isolated case reports. Correct diagnosis of primary cutaneous MCL requires ensuring that no other parts are involved, and these cases require close follow-up to monitor the possible progression to systemic disease and for the treatment of relapsed cutaneous disease. The prognosis of primary cutaneous MCL is relatively favorable, provided that the diagnosis is conclusive, and treatment options should comply with the clinical condition of the patient. For localized disease, radiotherapy or surgical resection followed by frequent observation should be the treatment of choice;however, chemotherapy should be considered efficient for prolonged survival.
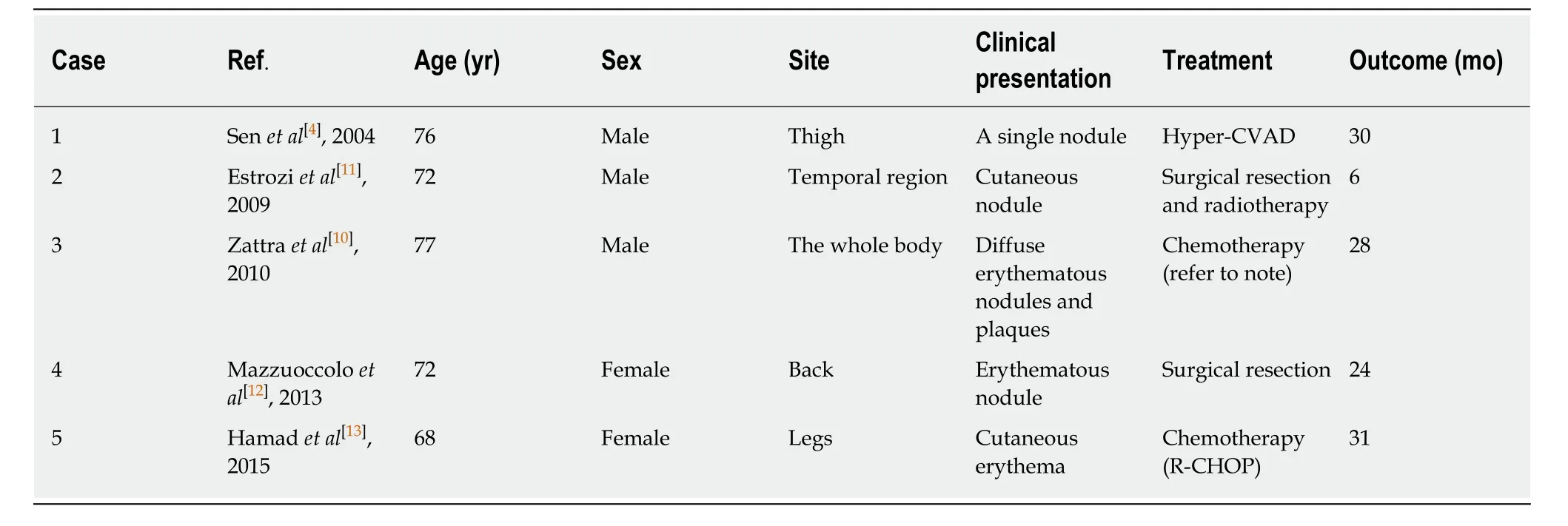
Table 1 Clinical features of five cases of primary cutaneous mantle cell lymphoma reported previously
ACKNOWLEDGEMENTS
The authors would like to thank Lan Sun from our department for performing and providing the FISH results and corresponding images.
 World Journal of Clinical Cases2020年8期
World Journal of Clinical Cases2020年8期
- World Journal of Clinical Cases的其它文章
- Clinicopathological differences and correlations between right and left colon cancer
- Bedside score predicting retained common bile duct stone in acute biliary pancreatitis
- Stability and infectivity of coronaviruses in inanimate environments
- Status, challenges, and future prospects of stem cell therapy in pelvic floor disorders
- Unusual presentation of congenital radioulnar synostosis with osteoporosis, fragility fracture and nonunion: A case report and review of literature
- Predictive factors for central lymph node metastases in papillary thyroid microcarcinoma