Nomogram using F-18 fluorodeoxyglucose positron emission tomography/computed tomography for preoperative prediction of lymph node metastasis in gastric cancer
2020-05-16 03:05:12BongIlSong
Bong-Il Song
Bong-Il Song, Department of Nuclear Medicine, Keimyung University Dongsan Hospital,Keimyung University School of Medicine, Daegu 42601, South Korea
Abstract
Key words: Gastric cancer; Lymph node metastasis; Positron emission tomography/computed tomography; Fluorodeoxyglucose; Prognostication; Standardized uptake value
INTRODUCTION
Gastric cancer (GC) is one of the most commonly diagnosed malignancies and the second leading cause of cancer-related deaths worldwide[1]. The status of lymph node(LN) metastasis is an important prognostic factor in GC, and complete dissection of the metastatic LNs is the only curative treatment for GC[2]. Although contrastenhanced computed tomography (CT) and endoscopic ultrasonography (EUS) are used for the diagnosis of LN metastasis in GC, the accuracy of diagnostic performance for LN metastasis is imperfect[3,4].
Positron emission tomography/computed tomography (PET/CT) with18Ffluorodeoxyglucose (F-18 FDG) has become a useful diagnostic modality for staging,treatment response evaluation, and detection of recurrence in GC[5,6]. However, F-18 FDG PET/CT has shown relatively low sensitivity in the detection of LN metastasis in GC[7,8]. Recently, metabolic information of the primary tumor obtained using F-18 FDG PET/CT has been suggested as a promising predictive marker for LN metastasis[9-11].Glucose metabolism in the primary tumor reflects not only the total tumor burden,but also the aggressiveness of cancer associated with LN metastasis. Therefore, a combination of the metabolic information of the primary tumor and metastatic LN could be useful in predicting LN metastasis in GC.
Recently, a few studies have been undertaken to develop a nomogram for the prediction of LN metastasis in GC[12,13]. However, these LN metastasis prediction models are based on postoperative parameters. Nevertheless, a preoperative LN metastasis prediction model, based on the tumor metabolic information as measured by F-18 FDG PET/CT, does not exist for GC. This model would be crucial for clinicians to determine the most effective treatment strategy.
The aim of this retrospective study was to determine whether the metabolic information of LN, as well as the primary tumor, could be prognostic factors for the prediction of LN metastasis in GC and to develop a preoperative nomogram for the prediction of LN metastasis in GC.
MATERIALS AND METHODS
Patients
Between January 2008 and December 2010, the medical records of 873 consecutive patients who underwent surgery for primary GC at Keimyung University Dongsan Medical Center (Daegu, South Korea) were retrospectively reviewed. Of these, 566 patients who underwent preoperative F-18 FDG PET/CT and subsequent surgical treatment without any preoperative intervention were enrolled in this study. The exclusion criteria were as follows: any other treatment prior to surgery such as gastric endoscopic submucosal dissection or chemotherapy, multiple primary malignancies,surgery for recurred GC, unavailable clinicopathological report, or an interval over 1 month between F-18 FDG PET/CT and surgery. A total of 566 GC patients were randomly divided into 377 of the training cohort and 189 of the internal validation cohort (2:1) (Figure 1). This retrospective study was approved by the Institutional Review Board of Keimyung University Dongsan Medical Center. The need for informed consent was waived, and all data were anonymized prior to the analysis.
All patients underwent subtotal or total gastrectomy along with D1+β or D2 lymphadenectomy in early GC and D2 lymphadenectomy in advanced GC.Clinicopathological data, including age at surgery, sex, location of the tumor,pathologic T (pT) stage, serum white blood cell (WBC) count, blood hemoglobin and serum albumin levels, platelet count, neutrophil count, lymphocyte count, platelet to lymphocyte ratio (PLR), neutrophil to lymphocyte ratio (NLR), preoperative carcinoembryonic antigen (CEA), and carbohydrate antigen (CA) 19-9 were retrieved from the patients' medical records. The pT stage was classified according to the 8th edition of the American Joint Committee on Cancer (AJCC) tumor-node-metastasis(TNM) staging system.
F-18 FDG PET/CT scan and image analysis
All the patients fasted for at least 6 h before F-18 FDG injection, and the blood glucose level was managed to be lower than 150 mg/dL. The PET/CT scan was performed 60 min after F-18 FDG was administered. PET/CT scans were performed using a Discovery STE PET/CT scanner (GE Healthcare, Milwaukee, WI, United States). First,a low-dose CT scan (peak voltage of 120 kVp, automated tube current ranging from 60 to 150 mA, and slice thickness of 3.75 mm) for attenuation correction without contrast enhancement was acquired. After CT scan, PET scan was performed immediately with an acquisition time of 3 min per bed position in 3D mode. The PET images were reconstructed using an ordered-subset expectation maximum iterative reconstruction algorithm.
由此,針對游客在景區(qū)的核心需求,如何運(yùn)用化繁為簡的方式獲得最全面的游玩方式,是值得我們思考的問題。這樣既可以最大程度的節(jié)省游客時(shí)間,全面統(tǒng)一的查看某個(gè)景點(diǎn)的景觀魅力,又可以讓游客們感覺到旅游的輕松便捷,自由自在。
All the F-18 FDG PET/CT images were retrospectively interpreted on an Advantage Workstation 4.3 (GE Healthcare), blinded to the status of LN metastasis.First, all F-18 FDG PET/CT images were visually assessed and classified as positive or negative with respect to F-18 FDG uptake by the primary tumor or LN. A positive uptake was defined as abnormally increased F-18 FDG uptake that exceeded the physiologic uptake by the surrounding stomach wall and corresponding cancer lesions on esophagogastroduodenoscopy. Consequently, the maximum standardized uptake value (SUVmax) of the primary tumor (T_SUVmax) was obtained only in positive F-18 FDG uptake lesions. In case of LNs, SUVmax of LN (N_SUVmax) was acquired in the highest focal F-18 FDG avid LN on PET image regardless of size on CT. A spherical volume of interest was manually drawn over the maximum F-18 FDG uptake lesions on the attenuation-corrected transaxial F-18 FDG PET images for semiquantitative analysis. The SUVmax was calculated using the following formula:SUVmax = maximum activity in the region of interest (MBq/g)/ [injected dose(MBq)/body weight (g)].
Statistical analysis
Numeric data were expressed as the mean ± SD. First, all the factors that were significantly associated (P< 0.05) with LN metastasis were identified in univariate analysis, and these significant factors were then evaluated to determine the variables independently associated with LN metastasis using multivariate logistic regression.Second, the LN metastasis prediction model was developed using the multivariate logistic analysis with a stepwise backward elimination method in the training cohort,and validated in the internal validation cohort. All variables withP< 0.05 in the univariate logistic analysis were selected for multivariate logistic analysis in the training cohort, and deleting the variable whose loss gives the most statistically insignificant deterioration of the prediction model fit. Lastly, we developed a nomogram as a graphical tool for calculating the risk of LN metastasis in individual patients. All statistical analyses were performed using R version 3.5.0 software(http://www.r-project.org, R Foundation for Statistical Computing, Vienna, Austria).AP< 0.05 was considered statistically significant.
RESULTS
Patient characteristics
The characteristics of the enrolled patients and the associations of these characteristics with LN metastasis in the training cohort (n= 377) and internal validation cohort (n=189) are summarized in Table 1. Of the 566 patients enrolled in the present study, 232(41.0%) had pathologically confirmed LN metastasis and 334 patients (59.0%)presented with no LN metastasis. The sensitivity, specificity, and accuracy of F-18 FDG PET/CT for the diagnosis of LN metastasis in GC patients were 28.9%, 97.3%,and 69.3%, respectively. Clinicopathological findings; tumor location, pT stage, blood hemoglobin levels, platelet count, lymphocyte count, PLR, NLR, CA 19-9, serum albumin, and metabolic parameters; T_SUVmax, and N_SUVmax were significantly different between the two groups (with or without LV metastasis); however, no significant differences were found with respect to age, sex, WBC count, neutrophil count, and serum CEA in the training cohort.
Uni- and multivariate logistic regression analyses
Univariate logistic regression analysis revealed that tumor location, blood hemoglobin levels, platelet count, lymphocyte count, PLR, NLR, CA 19-9, serum albumin,T_SUVmax, and N_SUVmax were significantly associated with LN metastasis in the training cohort. In multivariate analysis, T_SUVmax (OR = 1.08; 95%CI: 1.02-1.15;P=0.011) and N_SUVmax (OR = 1.49; 95%CI: 1.19-1.97;P= 0.002) were found to be independent predictive factors for LN metastasis in the training set (Table 2). Also,T_SUVmax (OR = 1.17; 95%CI: 1.07-1.29;P< 0.001) and N_SUVmax (OR = 1.60;95%CI: 1.09-2.69;P= 0.038) were independent predictive factors for LN metastasis in the test set (Table 3).
LN metastasis prediction model and nomogram
The result of the stepwise backward regression showed that a prediction model that combines T_SUVmax, N_SUVmax, serum albumin, and CA 19-9 was the best model to predict the risk of LN metastasis in the training cohort. The Hosmer and Lemeshow test generated aPvalue of 0.484, indicating that this predictive model fits well. A nomogram for predicting the probability of LN metastasis using pretreatment F-18 FDG PET/CT parameters and laboratory findings was successfully developed (Figure 2). The performance of this LN metastasis prediction model was good with the area under the receiver operating characteristic curve (AUC) of 0.733 (95%CI: 0.683-0.784,P= 0.025) in the training cohort and AUC of 0.756 (95%CI: 0.678-0.833,P< 0.001) in the test cohort (Figure 3).

Table 1 Patient characteristics
DISCUSSION
In the present study, the incidence of LN metastasis in GC patients was 41% and the diagnostic performance of F-18 FDG PET/CT was highly specific for LN metastasis status; however, it had a limitation due to its relatively low sensitivity. The present study revealed that T_SUVmax and N_SUVmax measured by preoperative F-18 FDG PET/CT are independent predictive factors for LN metastasis in patients with GC.Moreover, the combination of these metabolic parameters with clinical laboratory findings (albumin and CA 19-9) significantly improved prediction of LN metastasis,compared with each parameter alone.
從目前認(rèn)定情況看,申請人主要以病理學(xué)或藥理學(xué)專家工作小組或聯(lián)盟為主,他們對生物標(biāo)志物的研究并不依托于特定藥物研發(fā)項(xiàng)目,而是致力于推動制藥行業(yè)研發(fā)水平的整體提升。同時(shí),已經(jīng)認(rèn)定的生物標(biāo)志物以非臨床研究階段應(yīng)用為主,但對于藥物臨床試驗(yàn)階段的安全性、有效性研究也可以提供支持,F(xiàn)DA臨床審查部門也可以根據(jù)具體情況決定如何將其更好地使用在臨床研發(fā)項(xiàng)目中。
Several previous studies demonstrated that F-18 FDG PET/CT had relatively low sensitivity in detecting LN metastasis in GC patients[7,8,14]. In agreement with those studies, the results of the present study showed relatively low sensitivity. Despite the high specificity in the detection of LN metastasis, routine use of F-18 FDG PET/CT for GC stating is still controversial due to its low sensitivity[14-16]. A few studies have found that F-18 FDG uptake by the primary gastric tumor may predict LN metastasis status. Ohet al[17]reported that the peak-SUV of the primary gastric tumor is a useful indicator for LN metastasis. Kimet al[18]demonstrated that the T_SUVmax was the only independent factor to be significantly related to sensitivity for LN metastasis.However, no study has evaluated the predictive value of the combination of T_SUVmax and N_SUVmax for LN metastasis in GC. Notably, the present study showed that T_SUVmax and N_SUVmax were independent predictive factors for LN metastasis in the validation cohort as well as the training cohort.
Several studies have found that F-18 FDG uptake by the primary tumor ispositively correlated with the status of LN metastasis in various cancers[9,19,20]. The present study also suggested that T_SUVmax was an independent prognostic factor for LN metastasis in patients with GC. This result could be explained by the fact that T_SUVmax reflects not only the tumor's metabolic information, but also the tumor aggressiveness[21,22]. In this regard, T_SUVmax could have an additional value in predicting LN metastasis by reducing the high false-negative rate of F-18 FDG PET/CT for LN metastasis in patients with GC.

Table 2 Uni- and multivariate logistic regression analyses for regional lymph node metastases in the training cohort
Some studies have found that pretreatment serum albumin[23,24]and CA 19-9[25-27]levels are correlated with LN metastasis. The chronic systematic inflammatory state increases the vascular permeability and loss of serum protein. Hypoalbuminemia,therefore, results from and reflects the systematic inflammatory condition. The inflammatory component contributes to tumor proliferation, angiogenesis, and metastasis[28]. For this reason, the serum albumin level is associated with LN metastasis. Meanwhile, CA 19-9 is a tumor-associated antigen and has recently been demonstrated to be a marker of digestive tract malignancies, especially pancreatic cancer[29]. Accordingly, the pretreatment serum albumin and CA 19-9 levels could be promising predictive factors for LN metastasis in patients with GC.
Meanwhile, the positive rate of LN differs by T stage, and the clinical significance of preoperative prediction of LN also depends on T stage. However, the endpoint of this study was the development of the preoperative LN metastasis prediction model.Therefore, despite the positive rate of LN differing by T stage, T stage could not be considered as a predictive parameter in this study. Although, there are several studies for the precise diagnosis of T stage using endoscopic ultrasonography (EUS), the accuracy of EUS for T stage ranged between < 50% and > 90%[30-33]. In GC, accurate preoperative prediction of LN status according to the specific T stage could provide more detailed pretreatment decision making. Since T stage is one of the most important factors for not only LN status prediction but also treatment decision making, establishment of reliable and objective method for the accurate T stage could be a useful co-consideration parameter for the prediction of LN metastasis and GC treatment.
Recently, validation of nomograms for calculating the risk of LN metastasis in GC has been reported[12,13]. However, no study has yet established a nomogram for prediction of LN metastasis using preoperative clinical parameters. The present study successfully developed an effective nomogram to predict LN metastasis in GC using T_SUVmax, N_SUVmax, serum albumin, and CA 19-9. Considering the feasibility of F-18 FDG PET/CT in the preoperative setting of GC, F-18 FDG PET/CT could be used as a non-invasive diagnostic tool for assessment of LN metastasis status in patientswith GC and can be used to optimize current treatment strategy for patients with GC patients. The accurate preoperative prediction of LN can support clinicians in classifying patients who could receive minimal surgery or may derive greater clinical benefit from more extensive treatment.

Table 3 Uni- and multivariate logistic regression analyses for regional lymph node metastases in the test cohort
This study had a few limitations. First, this study was a single-institution,retrospective study that might have been subject to selection bias. External validation is necessary to assess transferability of the LN prediction model. Second, the SUV of the small-sized primary tumor and LNs could be underestimated due to partialvolume effects. Lastly, since F-18 FDG uptake can be elevated by not only the malignant cell, but also the inflammatory lesion, SUVmax might be overestimated in some patients.
In conclusion, T_SUVmax and N_SUVmax were independent prognostic factors for the prediction LN metastasis in GC patients. Further, a prediction model using metabolic parameters (T_SUVmax and N_SUVmax) and laboratory findings (albumin and CA 19-9) could provide a more precise prediction of LN metastasis in the preoperative setting. The use of preoperative F-18 FDG PET/CT could be a useful tool for LN metastasis evaluation and treatment planning in patients with GC.
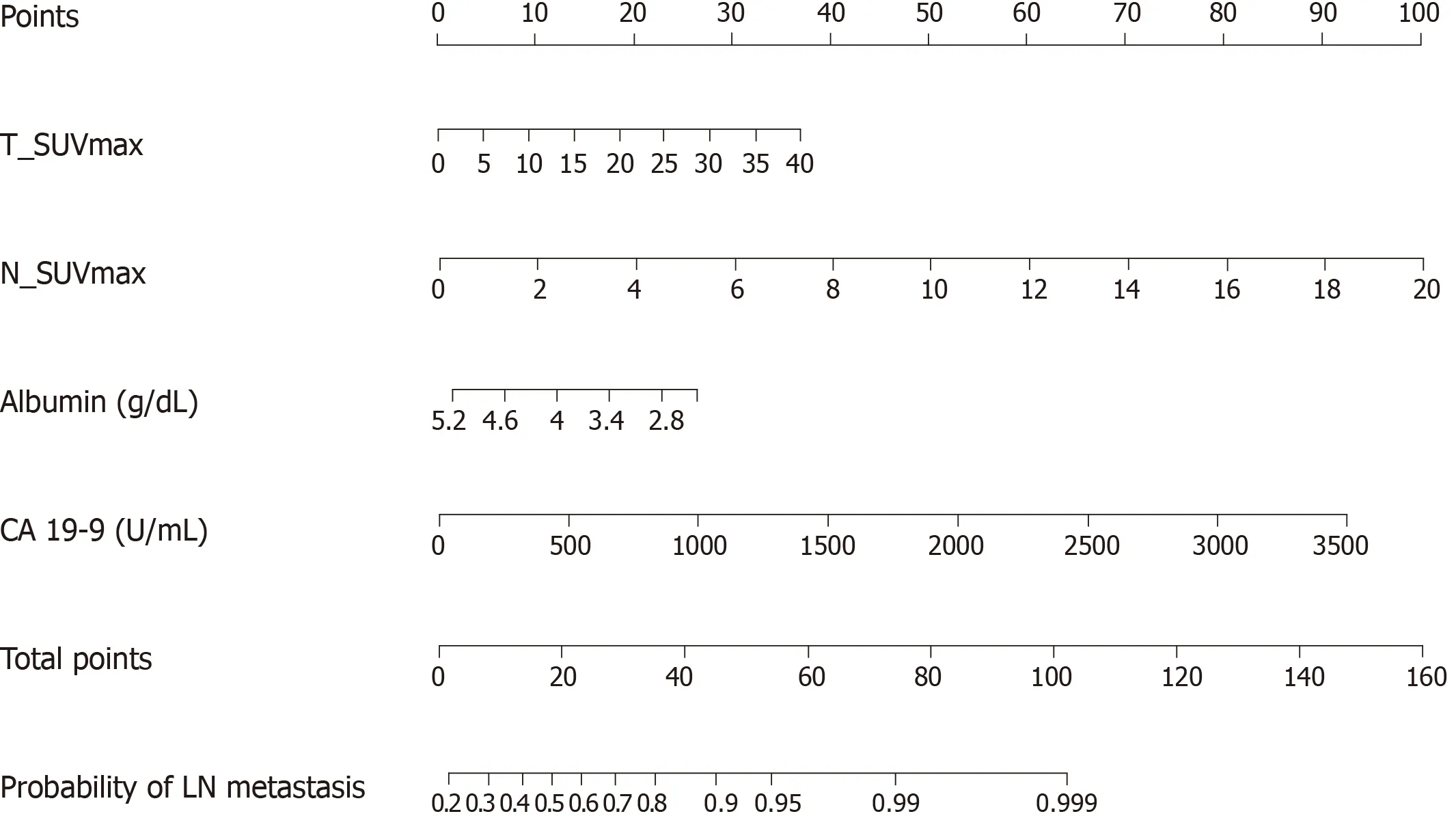
Figure 2 Nomogram for predicting the risk of lymph node metastasis using preoperative F-18 Fluorodeoxyglucose positron emission tomography/computed tomography and laboratory parameters. First, the number of points for each parameter -maximum standardized uptake value of primary tumor, maximum standardized uptake value of lymph node, albumin, and CA 19-9 - should be determined by drawing a vertical line from the exact value of variables to the points row. Subsequently, total points can be obtained by sum of four variables. The individual predictive risk of lymph node metastasis can be calculated by drawing a vertical line from the total points row to the probability of regional lymph node metastasis. T_SUVmax: Maximum standardized uptake value of primary tumor; N_SUVmax: Maximum standardized uptake value of lymph node; LN: Lymph node.

Figure 3 C-statistic of the combination model using metabolic parameters (maximum standardized uptake value of primary tumor and maximum standardized uptake value of lymph node) and laboratory findings (albumin and CA 19-9). C-statistic using receiver operating characteristic curve analysis, the area under the curve was 0.733 (95%CI: 0.683-0.784, P = 0.025) for lymph node metastasis prediction performance in the training cohort (black line), and area under the curve was of 0.756 (95%CI: 0.678-0.833, P < 0.001) in the test cohort (red line). AUC: Area under the curve.
ARTICLE HIGHLIGHTS
Research background
Gastric cancer (GC) is one of the most commonly diagnosed malignancies and the second leading cause of cancer-related deaths worldwide. The status of lymph node (LN) metastasis is an important prognostic factor in patients with GC. However, the evaluation of LN metastasis status in the preoperative setting is not accurate.
Research motivation
A few studies have been conducted to develop a nomogram for the prediction of LN metastasis in GC. However, a preoperative LN metastasis prediction model, based on the tumor metabolic information as measured by F-18 fluorodeoxyglucose (F-18 FDG) positron emission tomography/computed tomography (PET/CT) and laboratory findings, does not exist for GC.The purpose of this study was to develop a preoperative nomogram for LN metastasis in patients with GC.
Research objectives
This study aims to identify predictive factors and to develop a preoperative nomogram for the prediction of LN metastasis using F-18 FDG PET/CT and preoperative laboratory findings in patients with GC.
Research methods
Between 2008 and 2010, a total of 566 GC patients who underwent preoperative F-18 FDG PET/CT and subsequent surgical treatment without any preoperative intervention were analyzed. The LN metastasis prediction model was developed in the training cohort (n= 377)and validated in the internal validation cohort (n= 189). Clinicopathological data were retrieved from the patients' medical records and the F-18 FDG PET/CT images were retrospectively interpreted. Univariate and multivariable logistic regression was performed to validate the preoperative predictive factors for LN metastasis.
Research results
The multivariate logistic analysis showed that the combination of maximum standardized uptake value (SUVmax) of the primary tumor (T_SUVmax) and SUVmax of LN (N_SUVmax),serum albumin, and carbohydrate antigen (CA) 19-9 was the best model to predict the risk of LN metastasis. The preoperative nomogram for the prediction of LN metastasis using T_SUVmax,N_SUVmax, serum albumin, and CA 19-9 showed good performance in the validation cohort as well as the training cohort.
Research conclusions
The combination of preoperative F-18 FDG PET/CT metabolic parameters (T_SUVmax and N_SUVmax) and laboratory findings (albumin and CA 19-9) could be a useful tool for LN metastasis assessment and treatment planning in patients with GC.
Research perspectives
The preoperative nomogram for the prediction of LN should be verified on a larger and external validation cohort for widespread acceptance.
猜你喜歡
天天愛科學(xué)(2022年9期)2022-09-15 01:12:54
體育科技文獻(xiàn)通報(bào)(2022年3期)2022-05-23 13:46:54
天天愛科學(xué)(2022年4期)2022-05-23 12:41:48
當(dāng)代水產(chǎn)(2022年3期)2022-04-26 14:26:56
天津外國語大學(xué)學(xué)報(bào)(2021年3期)2021-08-13 08:32:18
遼金歷史與考古(2021年0期)2021-07-29 01:06:54
科學(xué)大眾(2021年9期)2021-07-16 07:02:54
軍事文摘(2020年20期)2020-11-28 11:42:50
航空世界(2020年10期)2020-01-19 14:36:20
科技傳播(2019年22期)2020-01-14 03:06:54
 World Journal of Gastrointestinal Oncology2020年4期
World Journal of Gastrointestinal Oncology2020年4期
- World Journal of Gastrointestinal Oncology的其它文章
- Adjuvant chemotherapy in curatively resected rectal cancer: How valid are the data?
- Expression and significance of miR-654-5p and miR-376b-3p in patients with colon cancer
- Evaluation of the value of multiparameter combined analysis of serum markers in the early diagnosis of gastric cancer
- Prognostic significance of systemic immune-inflammation index in patients with intrahepatic cholangiocarcinoma undergoing hepatic resection
- Perineural invasion of hilar cholangiocarcinoma in Chinese population: One center's experience
- Diagnostic ability of multi-detector spiral computed tomography for pathological lymph node metastasis of advanced gastric cancer