Role of IL-17 gene polymorphisms in osteoarthritis: A meta-analysis based on observational studies
2020-06-17 05:54:10HaoYuYangYuZhouLiuXinDieZhouYongHuangNanWeiXu
World Journal of Clinical Cases 2020年11期
Hao-Yu Yang, Yu-Zhou Liu, Xin-Die Zhou, Yong Huang, Nan-Wei Xu
Hao-Yu Yang, Yu-Zhou Liu, Department of Orthopedics, Wuxi 9th People’s Hospital affiliated to Soochow University, Wuxi 214000, Jiangsu Province, China
Xin-Die Zhou, Yong Huang, Nan-Wei Xu, Department of Orthopedics, The Affiliated Changzhou No.2 People’s Hospital of Nanjing Medical University, Changzhou 213003, Jiangsu Province,China
Abstract
Key words: Interleukin-17; Polymorphism; Osteoarthritis; Meta-analysis; Odds ratio;Confidence interval
INTRODUCTION
Osteoarthritis (OA) is a common form of arthritis that can cause progressive loss of joint function[1]. OA is characterized by softening, splitting, and fragmentation of articular cartilage, which is usually accompanied by subchondral bone sclerosis, bone cysts, and bony outgrowths at the joint margins[2]. OA is the combined result of complex pathogenic factors, including mechanical, biochemical, environmental,endocrine, metabolic, and genetic factors, which account for nearly 50% of the risk of OA development[3-6]. Some previous genome-wide association studies[7,8]have suggested that polymorphisms in some genes may affect OA pathogenesis. Genetic markers, in combination with imaging (such as X-ray, magnetic resonance imaging and ultrasound[9,10]) and biochemical markers, have the potential to assist in identifying and diagnosing OA in the early stage[11].
One of the most important family of genes associated with OA is the inflammatory cytokines gene family[12]. Inflammatory cytokines [such as interleukin-1β (IL-1β), IL-6,tumor necrosis factor-α, matrix metalloprotein-13] and moderate physical activity together play a possible biological role in the development of OA[13,14]. IL-17 involves five confirmed receptors and six members (IL-17A-F)[15,16]. Recent evidence has shown that IL-17 was detectable in serum samples and synovial fluid from OA subjects, and a direct correlation between the IL-17 concentration and the severity of OA was observed[17,18]. IL-17 induces the release of chemokines by chondrocytes and synovial fibroblasts, which contributed to synovial infiltration and cartilage collapse in OA[19].Although the pathogenesis and etiology of OA are not known, it is likely that IL-17 might play an important role in OA development.
To date, several studies[12,20-24]have explored the relationship between polymorphisms of theIL-17gene and OA susceptibility. The association betweenIL-17gene single nucleotide polymorphisms (SNPs) and OA susceptibility may provide novel research directions for OA studies[2]. However, the results of previous studies are inconclusive and conflicting due to clinical heterogeneity, different ethnic populations and small sample sizes. Meta-analysis is a statistical system for assembling results from different studies to produce a single approximate of the major effect with enhanced precision, especially when the results from single casecontrol studies are incomprehensive and conflicting. Therefore, in the present study we aimed to pool available data and investigated whetherIL-17gene polymorphisms were associated with OA susceptibility.
MATERIALS AND METHODS
The current meta-analysis was performed by following the PRISMA statement[25].
Search strategy
We systematically conducted a literature search using the following electronic databases: PubMed, EMBASE, MEDLINE, Cochrane Library, and Google Scholar to identify epidemiological studies published up to September 2019 to retrieve genetic association studies on OA. The terms “Interleukin-17”, “IL-17”, “SNP”,“polymorphism”, “variant”, “osteoarthritis” and “OA” were used to identify all publications reportingIL-17gene polymorphisms and OA risk. No language or other restrictions were placed on the search. Eligible studies were retrieved and cautiously evaluated. Furthermore, the reference lists of all related citations were screened to identify any missing studies.
Inclusion and exclusion criteria
Articles were filtered by two independent reviewers (Yang HY and Liu YZ) to assess the appropriateness of the articles selected using a standardized protocol and data collection form. The inclusion criteria were as follows: (1) Case-control studies on humans; (2) Comparison between OA patients and controls; (3) Studies evaluating the association betweenIL-17gene polymorphisms and OA susceptibility; and (4) Studies with sufficient genetic frequency for extraction. The exclusion criteria were as follows:(1) Studies with lack of information for data extraction; (2) Non-human studies,abstracts only, comments, reviews, editorials or letters, mechanistic studies, and studies missing controls; and (3) Duplicate or overlapping publications. All questionable publications were discussed and addressed by consensus.
Data extraction and quality assessment
From each eligible study, two reviewers (Yang HY and Liu YZ) independently extracted the following data: Authors, publication date, country, ethnicity, sample size, type of OA, source of controls, allele, and genotype frequency distribution. In addition, the two reviewers independently assessed the methodological quality of the included studies according to the Newcastle-Ottawa Scale (NOS)[26]. NOS criteria were scored based on three aspects: (1) Subject selection, 0-4; (2) Comparability of subjects,0-2; and (3) Exposure, 0-3. The NOS score ranged from 0 (lowest) to 9 (highest). The Hardy-Weinberg equilibrium (HWE) in controls was tested with Pearson’sχ2test(http://ihg.gsf.de/cgi-bin/hw/hwa1.pl).
Statistical analysis
Quantitative meta-analysis was employed using STATA 11.0 software (STATA Corporation, College Station, TX, United States). To assess the association betweenIL-17gene polymorphisms and the risk of OA, pooled odds ratios (ORs) with 95%confidence intervals (CIs) were calculated. Due to a lack of original data (sex and age),crude ORs were calculated, and five genetic models were included.P< 0.05 was considered statistically significant. Heterogeneity across studies was assessed by Q statistics with itsPvalue andI2statistics[27,28]. IfI2> 50% andP< 0.10, a random effects model was used in the calculations; otherwise, a fixed effects model was applied.Subgroup analyses were carried based on ethnicity and type of OA. Moreover, the Begg’s test and Egger’s linear regression analysis were applied to prevent publication bias[29]. To evaluate the precision and consistency of the primary meta-analysis,sensitivity analysis was performed to verify the effects associated with any individual study. Furthermore, false-positive report probability (FPRP) was conducted to evaluate the significant findings and rule out any false associations due to multiple tests[30]. Generally, the FPRP value for a given association betweenIL-17gene polymorphisms and OA risk was calculated with different prior probability. An association with a FPRP value < 0.2 at a prior probability of 0.1 indicated a significant relationship.
RESULTS
Characteristics of the included studies
In this study, the literature search yielded 132 citations, among which 46 duplicates were removed. Then, 78 of the 86 remaining citations were excluded after reviewing the titles and abstracts. The remaining 8 citations were sent for full text review, which resulted in exclusion of 1 citation due to the lack of detailed genotype data and 1 non-SNP study. Finally, 6 citations (2131 cases and 2299 controls) involving 8 studies and 4 SNPs were included in this study. The year of publication ranged between 2014 and 2019. In four of the included citations[20-22,24], the association betweenIL-17gene polymorphisms in an Asian population were investigated, and in two included citations[12,23]focus was on the Caucasian population. In all 6 citations[12,20-24], the association between rs2275913/rs763780 polymorphisms of theIL-17gene and risk of OA were studied. Detailed characteristics of the included citations are shown in Tables 1 and 2. A flowchart of reviews, showing the detailed selection process, is illustrated in Figure 1. The NOS scores ranged from 6 to 7 stars.
Association between rs2275913 polymorphism and OA susceptibility
General analysis showed that the polymorphism rs2275913 of theIL-17Agene increased OA risk [OR and 95%CI: 1.26 (1.08, 1.47) in AvsG; 1.25 (1.01, 1.55) in AA +GAvsGG; 1.53 (1.30, 1.81) in AAvsGA + GG; 1.71 (1.42, 2.06) in AAvsGG; and 1.15(1.01, 1.32) in GAvsGG, Table 3 and Figure 2]. Stratification analysis by ethnicity showed that the rs2275913 polymorphism increased the risk of OA among Asians [OR and 95%CI: 1.40 (1.18, 1.67) in AvsG; 1.44 (1.13, 1.82) in AA + GAvsGG; 1.62 (1.34,1.96) in AAvsGA + GG; 1.89 (1.52, 2.34) in AAvsGG; and 1.25 (1.06, 1.46) in GAvsGG, Table 3 and Figure 3); however, this was not observed in Caucasians. Subgroup analysis by OA type revealed that the rs2275913 polymorphism increased the risk of both knee and hip OA. A change in conclusion was not observed after eliminating a study[24]that did not meet the HWE.
Sensitivity analysis was used to determine the pooled ORs regarding the effects of this SNP on OA risk. Taken together, the results indicated that our data were stable and credible. Neither Egger’s nor Begg's tests revealed obvious publication bias for the rs2275913 polymorphism (Figure 4).
Association between rs763780 polymorphisms and OA susceptibility
Results of the pooled analysis on the association betweenIL-17Fgene rs763780 polymorphism and OA risk are shown in Table 3 and Figure 5 [OR and 95%CI: 1.32(1.06, 1.64) in CvsT; 1.32 (1.02, 1.72) in CC + TCvsTT; 2.08 (1.30, 3.32) in CCvsTC +TT; and 2.19 (1.37, 3.51) in CCvsTT]. Moreover, subgroup analysis by ethnicity indicated that rs763780 polymorphism increased OA risk among Caucasians in Allele/Dominant/Heterozygote models [OR and 95%CI: 1.75 (1.16, 2.66) in CvsT;1.82 (1.11, 3.00) in CC + TCvsTT; and 1.84 (1.06, 3.17) in TCvsTT], whereas among Asians in Recessive/Homozygote models [OR and 95%CI: 2.17 (1.32, 3.59) in CCvsTC + TT; and 2.28 (1.37, 3.77) in CCvsTT]. Stratification analysis by OA type revealed that the rs763780 polymorphism increased the risk of both knee and hip OA. A change in conclusion was not observed after eliminating a study[24]that did not meet the HWE. Both sensitivity analysis and the publication bias test revealed that our data were stable and credible (data not shown).
FPRP analysis result
For all statistically significant results, the FPRP values are summarized in Table 4. For a prior probability of 0.1 and crude ORs, the FPRP analysis indicated that the significant association between IL-17A rs2275913 polymorphism and OA risk was significant for all subjects (allele: FPRP = 0.052, recessive: FPRP = 0.009, and homozygous comparison: FPRP = 0.009), Asians (allele: FPRP = 0.013, dominant:FPRP = 0.048, recessive: FPRP = 0.009, homozygous: FPRP = 0.009, and heterozygous comparison: FPRP = 0.103), and knee OA (recessive comparison: FPRP = 0.010).Similarly, the association of theIL-17Frs763780 polymorphism with OA risk also deserved attention in the overall population, especially among Caucasians and individuals with knee/hip OA. In our study, greater values were observed of FPRP >0.2 for other positive findings betweenIL-17gene polymorphisms and OA risk, which may be attributed to the limited sample size. For future studies, additional validation will be needed using studies with a larger sample size.
DISCUSSION
Although the definite pathogenesis of OA remains unclear, genetic factors are considered to be strong determinants. IL-17 is a cytokine that is mainly synthesized by activated T cells, and its receptors are present in osteoblasts. IL-17 can enhance proinflammatory cytokines, including tumor necrosis factor-α, IL-1 and IL-6, that together play a key role in cartilage degradation and the inhibition of cartilage repair[31,32]. Furthermore, in patients with OA, IL-17 stimulates the release of vascularendothelial growth factor in synovial fibroblasts that was isolated from their joints[19].Therefore, an increasing number of studies focused on the association between theIL-17gene polymorphisms and OA susceptibility.
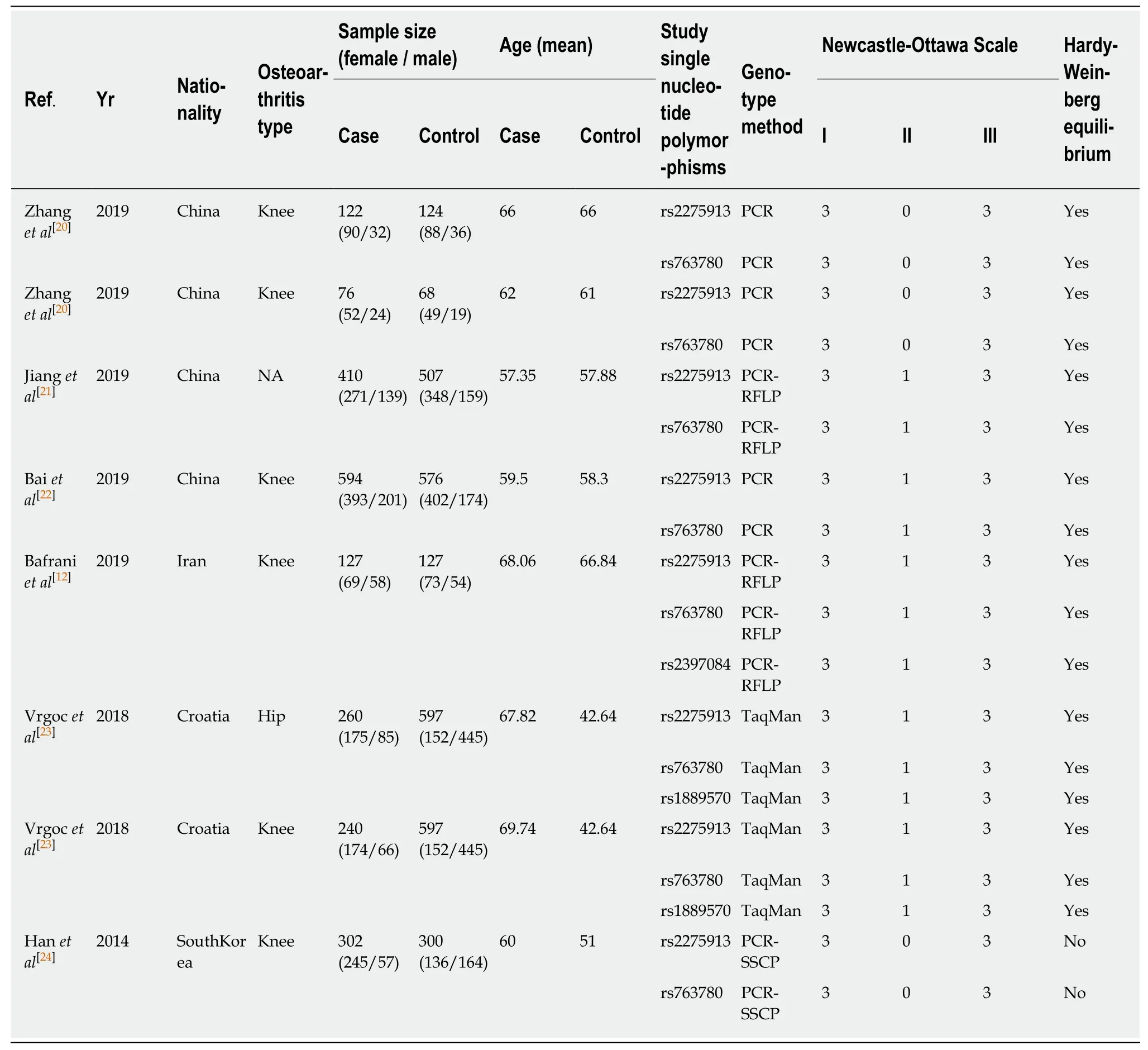
Table 1 Characteristics of included studies
Hanet al[24]first examined the alleles and genotypes ofIL-17Ars2275913 andIL-17Frs763780 in a Korean population, and found a significant association between rs2275913 and the susceptibility of knee OA. In addition, Vrgocet al[23]did not observe an association betweenIL-17Ars2275913 and the risk of hip or knee OA in a Croatian population. The C allele of theIL-17Fgene rs763780 polymorphism increased the risk of hip OA, but not of knee OA. The results of a study by Bafraniet al[12]indicated a significant association between rs2275913GA genotype and a decrease in the risk of knee OA. However, the rs763780TC genotype and rs763780C allele were related to an increased risk of knee OA. Zhanget al[20]suggested that the genotype AA frequency ofIL-17A(rs2275913) was significantly different between knee OA patients and the control group in a Chinese Han population, but not in a Tibetan population.Furthermore, Baiet al[22]indicated that theIL-17Ars2275913 polymorphism had a significant impact on the risk of knee OA. Additionally, the rs763780 C allele was found to be related to a greatly increased risk of developing knee OA. Jianget al[21]suggested a significant association between the increased risk of OA andIL-17Ars2275913, but not ofIL-17Frs763780. The discrepancy in the above-mentioned studies may be due to the following: First, the inclusion criteria differed among studies. For example, Baiet al[22]enrolled other types of arthritis or joint diseases, such as inflammatory arthritis, which were excluded by other citations. Moreover, Jianget al[21]used clinical symptoms and radiological evidence of joints, whereas in the Hanet al[24]study, OA cases who had undergone total knee arthroplasty were enrolled.Second, the allele frequencies of the rs2275913/rs763780 polymorphism in the cases were diverse. Third, the affected joint sites differed. Fourth, the genetic background of OA may vary among races. Finally, the difference in sample sizes may also account for this discrepancy.

Figure 1 Flowchart of the literature search and selection for this study.
Due to the limited sample sizes, previous single studies may have been underpowered and thereby may have presented conflicting findings, especially given the diverse inheritance of the heterogeneous and complex OA etiology, different ethnicities, clinical heterogeneity, and other causes. Therefore, we conducted this meta-analysis.
Our data showed that the rs2275913 and rs763780 polymorphisms increased the risk of OA. Stratification analyses by ethnicity and OA type showed that the rs2275913 polymorphism increased the risk of OA among Asians as well as in knee/hip OA,respectively. Stratification analyses also revealed that the rs763780 polymorphism increased OA risk among both Asians and Caucasians, as well as in knee/hip OA.There may be several possible reasons for the different findings regarding the rs2275913 polymorphism between Asians and Caucasians. First, genetic heterogeneity for OA exists in different populations. Second, these discrepancies may be explained by clinical heterogeneity. Third, the sample sizes of the Caucasian populations were not large enough to support a definitive conclusion. Additionally, different OA types and varying clinical parameters of different populations may also be potential reasons for the inconclusive findings. Furthermore, different characteristics of the OA groups(such as age and sex) and disease severity may also be possible reasons for the discrepancies observed. Finally, varying environmental factors may also have contributed, because the interaction between genetic factors and environmental factors can eventually lead to the development of OA. Gaoet al[33]and Leeet al[34]also conducted meta-analyses to study the association betweenIL-17gene rs2275913/rs763780 polymorphism and OA risk. We consider that our meta-analysis had several additional advantages. First, compared to the work by Leeet al[34], ourmeta-analysis of the rs3134069 polymorphism included one more case-controlled study[20]. Second, for rs2275913, Gaoet al[33]regarded the G allele as a minor allele and then analyzed it in 5 genetic models. In fact, according to the dbSNP database, A allele is the true minor allele. Gaoet al[33]misidentified the minor allele, which led to the wrong choice of genetic model. If the correct genetic model is selected, their results are consistent with our findings. This mistake was also found in the rs763780 polymorphism analysis. Third, FPRP was conducted in our meta-analysis to evaluate the significant findings and rule out any false associations due to multiple tests.
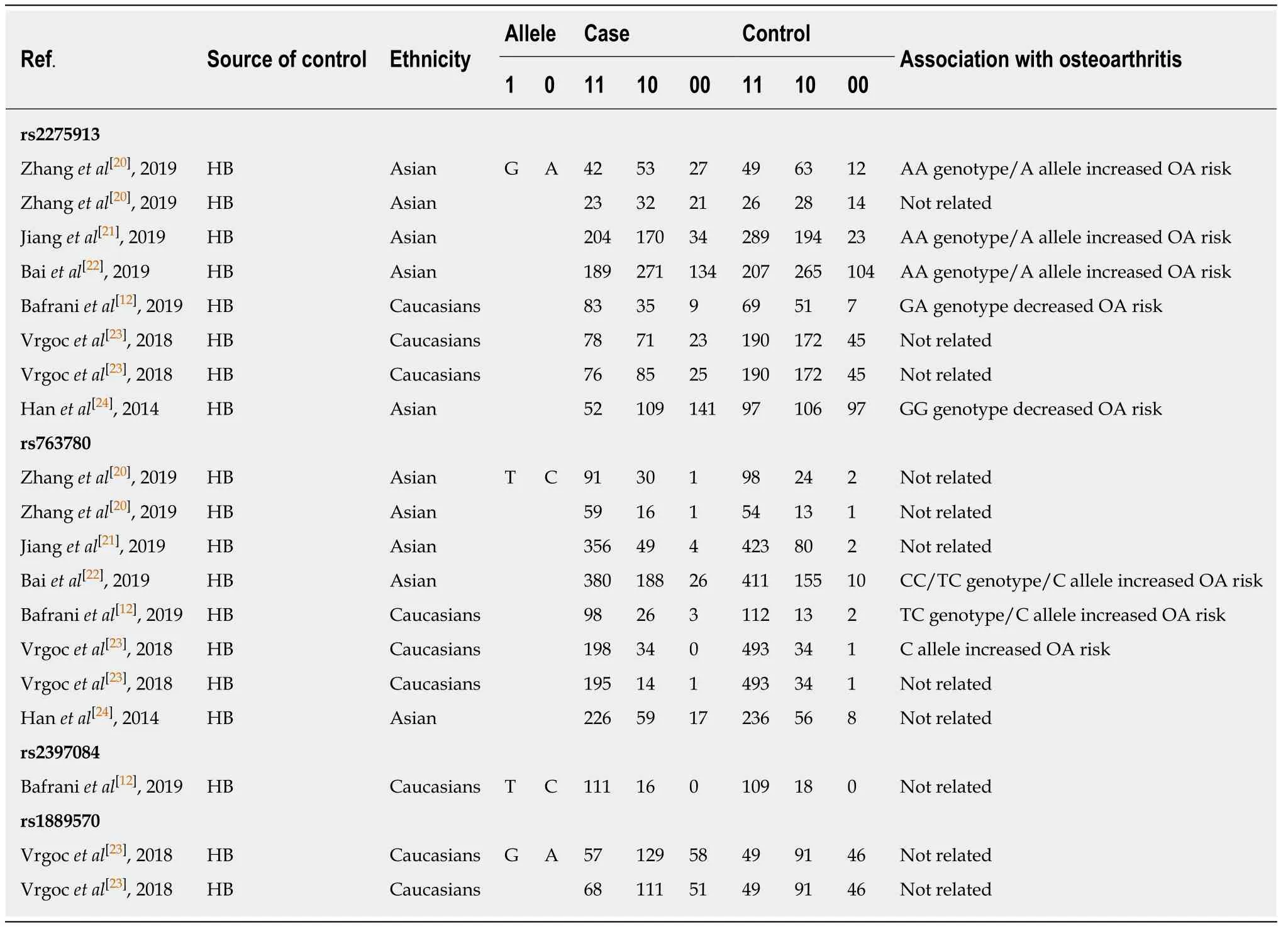
Table 2 Genotype distributions of IL-17 gene polymorphisms in the included studies
Our study has several limitations that should be considered. First, due to limited data, we were unable to conduct stratification analyses of other potential factors, such as age, sex, and age at OA onset. Second, our results were based on unadjusted estimates of confounding factors, which might have affected the final results. Third,although funnel plots and Egger’s tests revealed no publication bias, selection bias could not be fully prevented, because only studies published in the English language were searched. Fourth, we were unable to assess potential gene-gene or geneenvironment interactions due to the lack of relevant data. Fifth, in future studies,clinical cases should be investigated to support the analytical results observed in this study. Sixth, we can only infer but cannot conclude that theIL-17gene rs2275913/rs763780 polymorphism is a susceptibility locus for other types of OA.Thus, further investigation into more types of OA is warranted. Finally, five genetic models of inheritance were used, thus, type I error may have arisen through lack of correction for multiple testing.
In conclusion, the present meta-analysis demonstrated that the rs763780 polymorphism of theIL-17Fgene increased the risk of OA, whereas the rs2275913 polymorphism of theIL-17Agene only increased the risk of OA among Asians. Given the study limitations, further well-designed prospective studies with large sample sizes should be performed to validate these findings. In the future, it will become feasible to identify and diagnose OA in the early stage, as a result of genetic findings.Furthermore, the biological and functional relevance of these genetic findings is essential to help put the research into a clinical context to benefit people with OA.

Table 3 Meta-analysis of the association between IL-17 gene polymorphisms and osteoarthritis risk

OA: Osteoarthritis; SNP: Single nucleotide polymorphism.

Table 4 False-positive report probability values for associations between IL-17 gene polymorphisms and risk of osteoarthritis
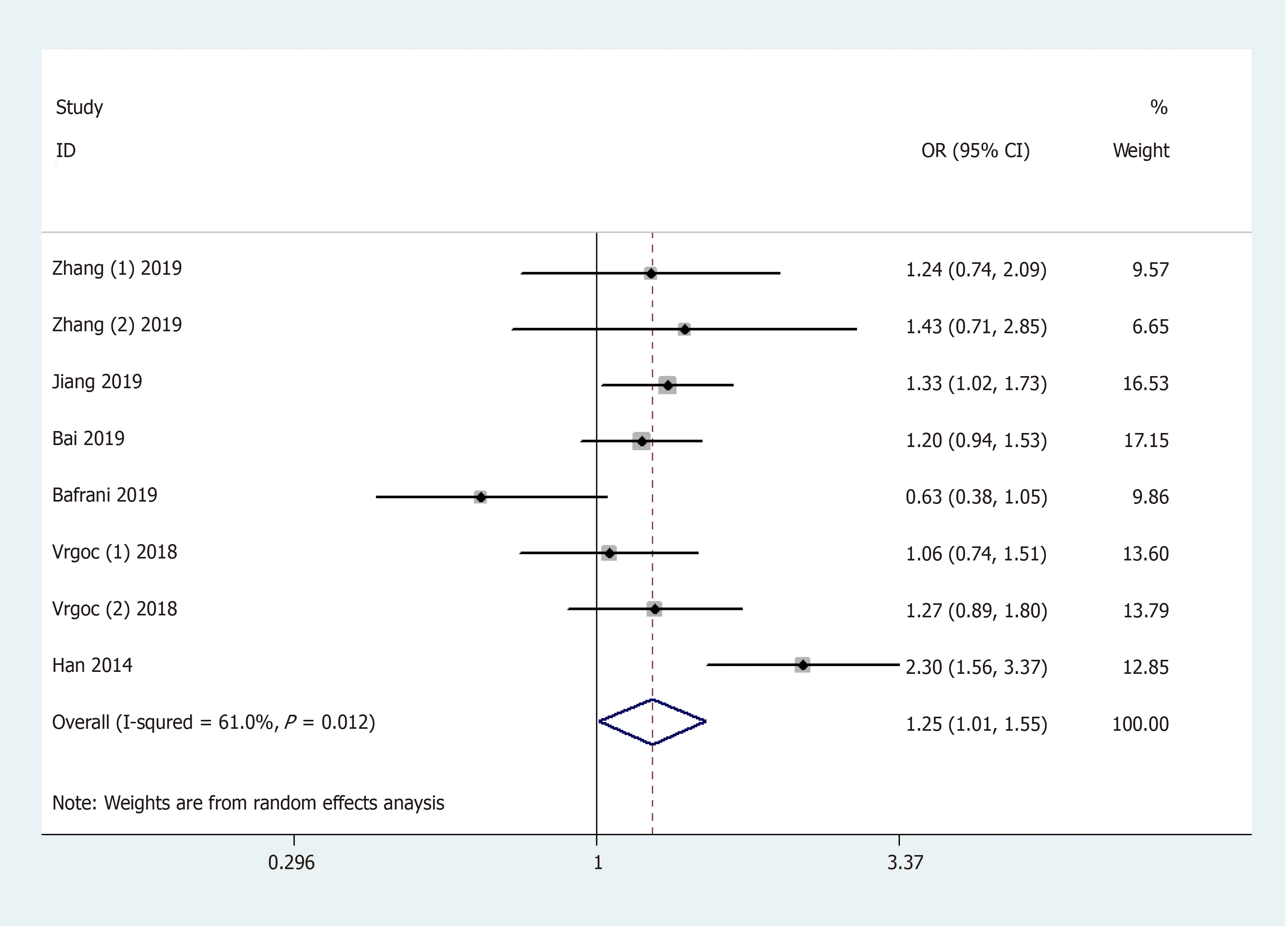
Figure 2 Forest plot shows odds ratios for the associations between rs2275913 polymorphism and osteoarthritis risk (AA + GA vs GG).

Figure 3 Stratification analysis by ethnicity shows odds ratio for the association between rs2275913 polymorphism and osteoarthritis risk (AA + GA vs GG).
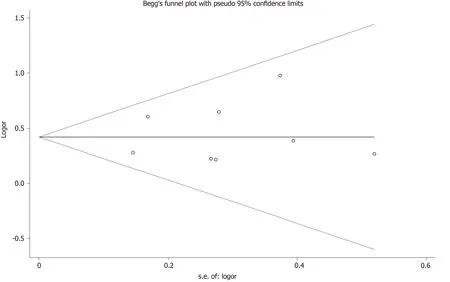
Figure 4 Begg's tests between rs2275913 polymorphism and osteoarthritis (AA vs GA + GG).

Figure 5 Forest plot shows odds ratios for the associations between rs763780 polymorphism and osteoarthritis risk (CC vs TC + TT).
ARTICLE HIGHLIGHTS
Research background
Osteoarthritis (OA) is the combined result of complex pathogenic factors, including mechanical,biochemical, environmental, endocrine, metabolic, and genetic factors, which account for nearly 50% of the risk of OA development. Although the pathogenesis and etiology of OA are not known, it is likely that interleukin-17 (IL-17) might play an important role in OA development.
Research motivation
To date, several studies have explored the relationship between polymorphisms of theIL-17gene and OA susceptibility. The association betweenIL-17gene single nucleotide polymorphisms and OA susceptibility may provide novel research directions for OA studies. However, the results of previous studies are inconclusive and conflicting due to clinical heterogeneity, different ethnic populations and small sample sizes.
Research objectives
We meta-analyzed relevant articles regarding the association between the polymorphisms ofIL-17gene and OA susceptibility.
Research methods
We systematically conducted the literature search using the following electronic databases:PubMed, EMBASE, MEDLINE, Cochrane Library, and Google Scholar to identify epidemiological studies published up to September 2019 to retrieve genetic association studies on OA. Pooled odds ratios with 95% confidence intervals were calculated. Subgroup analyses were carried based on ethnicity and type of OA. Furthermore, false-positive report probability was conducted to evaluate the significant findings and rule out any false associations due to multiple tests.
Research results
In a total of 6 citations involving 8 studies (2131 cases and 2299 controls), 4 single nucleotide polymorphisms were identified. Of these 4 polymorphisms, 2 (rs2275913, rs763780) were common in five case-control studies. Together, the pooled results revealed that the A allele and genotype AA/GA of the rs2275913 polymorphism, and the C allele and genotype CC of the rs763780 polymorphism in theIL-17gene increased the risk of OA. Furthermore, stratification analyses by ethnicity and OA type showed that the rs2275913 polymorphism increased the risk of OA among Asians and in knee/hip OA, respectively. In addition, stratification analyses also revealed that the rs763780 polymorphism increased OA risk among both Asians and Caucasians in knee/hip OA.
Research conclusions
The rs763780 polymorphism of theIL-17Fgene increased the risk of OA, whereas the rs2275913 polymorphism of theIL-17Agene increased the risk of OA only among Asians. Due to the limitations of this study, these findings should be validated in future studies.
 World Journal of Clinical Cases2020年11期
World Journal of Clinical Cases2020年11期
- World Journal of Clinical Cases的其它文章
- Macrophage activation syndrome as an initial presentation of systemic lupus erythematosus
- Optical coherence tomography guided treatment avoids stenting in an antiphospholipid syndrome patient: A case report
- Uterine incision dehiscence 3 mo after cesarean section causing massive bleeding: A case report
- Ataxia-telangiectasia complicated with Hodgkin's lymphoma: A case report
- Gastric pyloric gland adenoma resembling a submucosal tumor: A case report
- Reduced delay in diagnosis of odontogenic keratocysts with malignant transformation: A case report