Surgical closure of large splenorenal shunt may accelerate recovery from hepato-pulmonary syndrome in liver transplant patients
2020-12-09 05:41:00YanjunShiPatrickMckiernanKyleSoltysGeorgeMazariegosWeilinWang
Yan-jun Shi, Patrick Mckiernan, Kyle Soltys, George Mazariegos, Wei-lin Wang
1 Department of Hepatobiliary & Pancreas Surgery, the Second Affiliated Hospital of Zhejiang University School of Medicine, Hangzhou 310009, China
2 Thomas E. Starzl Transplantation Institute, Hillman Center for Pediatric Transplantation, Department of Transplant Surgery, Children's Hospital of Pittsburgh of the University of Pittsburgh Medical Center, Pittsburgh, PA, USA
Dear editor,
Hepatopulmonary syndrome (HPS) is not uncommon in the setting of liver disease, especially in liver cirrhosis patients. The prevalence of HPS in liver cirrhosis patients varies from 4% to 47%.[1-3]About the definition of HPS, it is a pulmonary vascular disorder with evidence of intrapulmonary arterial venous shunt.[4]Pulmonary dyspnea and polycythemia are common presentations of HPS. Dyspnea, cyanosis and clubbed fingers were present in most of all cases. Spider nevi is another common clinical feature of patients with HPS.[5]
The underline pathophysiology of HPS is not well understood. The possible mechanism is endogenous vasodilators like nitric oxide (NO).[6]NO causes abnormal vessel dilation of pulmonary capillary beds.[7]Eventually, it results in ventilation-perfusion mismatch.[8]Angiogenesis is also believed to play an important role in HPS patients.[9,10]There are two types of HPS. Type I is a more common type which is characterized by diffuse pulmonary vascular dilatations at the precapillary level.Type II is a more discrete and localized dilatations.Supplementary oxygen improves Type I HPS PaO2, but Type II HPS has a poor response to oxygen therapy.[11]
The diagnosis of HPS can be made if there is evidence of pulmonary vasodilatation with demonstrable functional shunting and hypoxia symptoms.[12,13]The diagnostic tests for HPS are Technetium-99 labelled macro aggregated albumin lung perfusion scan (99mTCMAA) and contrast echocardiogram. Bubble echo has been considered as gold standard to diagnose HPS.[13-15]
Oxygen supplementation is suggested in all hypoxemic HPS patients despite the lack of data to show improvements in survival. Liver transplantation is the only definitive treatment for HPS. Most patients with HPS undergoing liver transplantation experience either significant improvement or complete resolution in hypoxemia. This resolution however may take time and in some cases over a year.[16,17]
Spontaneous splenorenal shunts often develop in 20% of liver cirrhosis patients. It can result in significant blood steal from the transplanted liver. In most cases, it will eventually resolve after liver transplant. However,large shunts (> 1 cm) are less likely to collapse. It may influence the long-term graft survival of liver transplantation. Ligation of splenorenal shunt may reduce the vascular blood steal from the transplanted liver. It also reduces vasodilator in pulmonary capillary beds and eventually helps the resolve of HPS.[18]
CASE
A 21-year-old female was referred to us. She had been diagnosed with hepatoportal sclerosis and portal hypertension since she was two years old. Over the past few years, she complained of exertion dyspnea and was diagnosed with hepato-pulmonary syndrome. She was also noted to have a small (1.4 cm) focal adenoma in segment 6 and cirrhotic liver with significant varices including a native distal splenorenal shunt. She had ongoing shortness of breath with activity. She didn't use O2at home due to insurance issues. Her saturation ranged anywhere from 70% to 90%. She denied any recent illnesses, fevers, cough, chest pain, nausea, vomiting,abdominal pain and diarrhea.
She had mitral valve insufficiency and tricuspid valve regurgitation, without surgical history. Bubble study was performed within three beat of contrast visualization in the right heart. Bubbles were noted in the left atrium(LA) and left vebtricle (LV).
Pulmonary function test showed forced vital capacity(FVC) was normal, forced expiratory volume in one second(FEV1) normal, ratio normal, SpO2moderately reduced,PaO255. Large native distal splenorenal shunt was identified in CT scan (Figure 1). Hemoglobin (Hb) was 15 g/L,prothrombin time (PT) 14.1 s, international normalized ratio(INR) 1.1, partial thromboplastin time (PTT) 33 s, Bili 0.9 mg/dL, alanin aminotransferase (ALT) 56 U/L, aspartate aminotransferase (AST) 60 U/L, AKP 158 U/L, gamma glutamyl transferase (GGT) 50 U/L, creatinine (Cr) 0.6 μmol/L.
The donor was 25-year-old who succumbed to a head trauma. The donor was blood type A and all hepatitis and HIV serologies and nucleic acid testing (NAT) testing were negative, and cytomegalovirus (CMV) IgG and Epstein-Barr virus (EBV) IgG were both positive.
She underwent cadaveric orthotopic liver transplant with whole allograft on February 8, 2018. It was a piggyback liver transplant. We identified a native splenorenal shunt in the procedure. We decided to ligate the shunt to increase portal vein blood flow and help recovery from HPS (Figures 2 and 3). She recovered well immediately after operation. She was extubated 2 days after transplantation and liver enzyme trended down to be normal range. PaO2increased 80 at the day of discharge. SpO2was 100% on NC 1.5 liters. She was discharged home 15 days after operation. She was completely off O2one week after that.
DISCUSSION
As we known, liver cirrhosis patients develop collateral portocava shunt in several regions, like esophageal and gastric varices. It is important for portal vein blood flow diversion and for systemic hemodynamically compensation. Another way of decompression of the congested portal system is the formation of a spontaneous splenorenal shunt.Spontaneous splenorenal shunts often develop in 20%of liver cirrhosis patients. However, they are usually less accessible and surgeons usually do not examine it in the process of liver transplantation.[18,19]

Figure 1. CT image of large native distal splenorenal shunt.
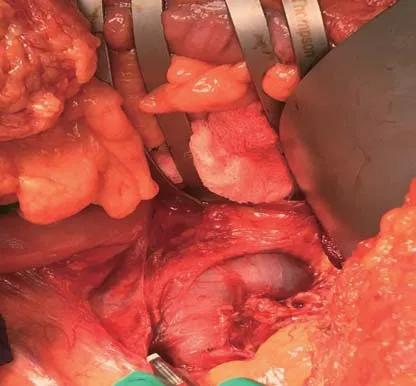
Figure 2. Intra-OP found large splenorenal shunt.
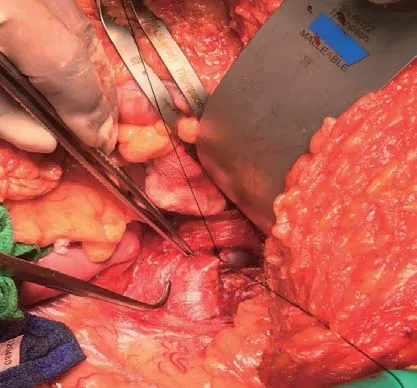
Figure 3. Surgical closure of spleno-renal shunt (ligation).
HPS is not completely understood. The possible mechanism is endogenous vasodilators like NO. NO causes abnormal vessel dilation at the level of pulmonary capillary beds. Eventually, it results in ventilationperfusion mismatch.[3-5,8]Natural prognosis of HPS is poor. The 5-year survival was only 23% without liver transplant. HPS is listed as model for end-stage liver disease (MELD) exception because HPS has a higher mortality and lower quality of life. Liver transplantation is the only definitive treatment for HPS. Most patients with HPS undergoing liver transplantation experience either significant improvement or complete resolution in hypoxemia. This resolution however may take time and in some cases over a year.[2-5,15]
In this unique case, patient had a large (>1 cm)native splenorenal shunt. It was identified by CT image before the operation. We decided to ligate the shunt to increase portal vein blood flow and help recovery from HPS. For this purpose, we explored it during the procedure and identified it. We surgically closed the shunt. Patient recovered well from liver transplant. In this case, patient was completely off O2about 4 weeks after transplantation. SaO2was about 90%. It was shorter than her natural history.
There is no direct evidence that closing the portosystemic shunt has impacted on the HPS in this case. However, there is evidence that closing the shunt does decrease pulmonary blood flow. Surgically closing the splenorenal shunt does increase portal vein blood flow and reduce liver ischemia. It also reduces vasodilators in pulmonary capillary bed and eventually accelerates recovery of HPS. However, the underlying mechanism still needs to be understood completely.[19]
We are not encouraging other teams to perform surgical maneuvers with the aim at stopping even small portosystemic collaterals. However, for large splenorenal shunt, especially larger than 1 cm shunt, it did increase portal blood flow and reduce blood steal. It did reduce pulmonary flow and accelerate the recovery from HPS for liver transplant patients.
We can also perform splenectomy intraoperatively,however as we know, it could increase the incidence of splenic vein thrombosis and even extends to portal vein.We had this type of complication during our practice.Postoperative splenic vein embolization is also an option, when blood f low steal is encountered. When the splenorenal shunt is difficult to expose, we can choose to ligate the left renal vein.[20,21]
CONCLUSIONS
In some cases, especially splenorenal shunt (>1 cm),surgical closure of the large native splenorenal shunt simultaneously with liver transplantation may accelerate recovery from hepato-pulmonary syndrome in liver transplant patients. However, it should be performed in selective case.
Funding:None.
Ethical approval:This study was approved by the Ethical Committee of Children's Hospital of Pittsburgh of the University of Pittsburgh Medical Center.
Conflicts of interests:The authors declare that there is no conflict of interest.
Contributors:YJS cared for the patient in question, reviewed the literature, and was primarily responsible for writing the manuscript. PM, KS, and GM contributed to the care of the patient and critically reviewed and edited the manuscript. WLW reviewed and edited the manuscript.
 World journal of emergency medicine2020年1期
World journal of emergency medicine2020年1期
- World journal of emergency medicine的其它文章
- Investigations for the assessment of adult patients presenting to the emergency department with supraventricular tachycardia
- Epidemiological characteristics and disease spectrum of emergency patients in two cities in China: Hong Kong and Shenzhen
- Role of penehyclidine in acute organophosphorus pesticide poisoning
- The first two cases of transcatheter mitral valve repair with ARTO system in Asia
- Admission delay is associated with worse surgical outcomes for elderly hip fracture patients: A retrospective observational study
- A pulmonary source of infection in patients with sepsis-associated acute kidney injury leads to a worse outcome and poor recovery of kidney function