Surgical therapy for hemangioma of the azygos vein arch under thoracoscopy: A case report
2021-04-14 07:18:02ZhenXingWangLiangLiangYangZheNanXuPeiYunLvYueWang
World Journal of Clinical Cases 2021年11期
Zhen-Xing Wang, Liang-Liang Yang, Zhe-Nan Xu, Pei-Yun Lv, Yue Wang
Zhen-Xing Wang, Liang-Liang Yang, Zhe-Nan Xu, Pei-Yun Lv, Yue Wang, Department of Thoracic Surgery, China-Japan Union Hospital of Jilin University, Changchun 130033, Jilin Province,China
Abstract BACKGROUND Azygos vein aneurysms are extremely rare, and their pathogenesis is not clear.The overwhelming majority of patients have no obvious clinical symptoms and are found to have the disease by physical examination or by chance. There are few reports on the diagnosis of and treatment strategy for this disease. Moreover, the choice of therapeutic schedule and the treatment window are controversial.CASE SUMMARY We report a case of azygos vein arch aneurysm in a 53-year-old woman. The patient had symptoms of back pain, chest tightness, and choking. Enhanced chest computed tomography showed a soft-tissue mass in the right posterior mediastinum, which was connected to the superior vena cava. The enhancement degree in the venous phase was the same as that of the superior vena cava. The patient received video-assisted thoracoscopic surgery. After the operation, her back pain disappeared, and her dysphagia and chest tightness were also significantly relieved. The postoperative pathology confirmed hemangioma. The patient was discharged on the seventh day after surgery without any complications.CONCLUSION Some patients with hemangioma of the azygos vein arch may experience dysphagia and chest tightness caused by the tumor compressing the esophagus and trachea. Enhanced computed tomography scanning is vital for the diagnosis of azygos vein aneurysms. In addition, despite the difficulty and risk of surgery,thoracoscopic surgery for azygos vein aneurysms is completely feasible.
Key Words: Azygos vein aneurysm; Hemangioma of the azygos vein arch; Mediastinal tumor; Thoracoscopic surgery; Case report
lNTRODUCTlON
Azygos vein aneurysms are extremely rare. There are few cases of the diagnosis and therapy of this disease in the medical literature. We report a case of hemangioma of the azygos vein arch in a 53-year-old woman. The patient had symptoms of back pain,chest tightness, and choking. To the best of our knowledge, this is the first case of a patient with choking symptoms due to compression of the esophagus by an azygos vein aneurysm. The enhanced chest computed tomography (CT) showed a soft-tissue mass in the right posterior mediastinum, which was connected to the superior vena cava. The enhancement degree in the venous phase was the same as that of the superior vena cava. The patient received video-assisted thoracoscopic surgery. After the operation, her back pain disappeared, and her dysphagia and chest tightness were also significantly relieved. The postoperative pathology confirmed hemangioma. The patient was discharged on the seventh day after surgery without any complications.Despite the difficulty and risk of surgery, it is completely feasible for azygos venous arch aneurysms to be repaired by thoracoscopic surgery.
CASE PRESENTATlON
Chief complaints
A 53-year-old woman experienced choking, chest tightness, and back pain.
History of present illness
The patient had experienced choking and chest tightness 2 years prior without any causation and had experienced back pain 1 year ago. Recently, the above symptoms had gradually been aggravated. The patient underwent gastroscopy that showed normal findings.
History of past illness
The patient had no other past illness except choking, chest tightness, and back pain.
Personal and family history
The patient had no remarkable personal and family history.
Physical examination
The physical examination was unremarkable.
Laboratory examinations
The patient was previously healthy and showed no abnormalities in the laboratory examinations.
Imaging examinations
CT revealed a soft-tissue mass approximately 4.2 cm × 3.7 cm × 2.6 cm in the right posterior mediastinum, for which the boundary between some areas and the esophagus was unclear, and the trachea was also compressed (Figure 1A). In the enhanced CT scan, a contrast agent was injected into the right upper limb. In the early arterial stage, the superior vena cava and the azygos vein arch were filled with the contrast agent, and the azygos vein arch was nodular. The density did not decrease in the venous phase, and there seemed to be a blood shadow during coronary reconstruction. The posterior mediastinal tumor showed delayed enhancement, and its internal density was not homogeneous. No definite filling defect was found. The tumor was connected to the superior vena cava, whose degree of enhancement was the same as that of the superior vena cava, and the boundary between the tumor and the esophagus was clear. The azygos vein valve was observed. The esophagus was compressed by an azygos vein aneurysm (Figure 1B). These findings indicated that there was a giant hemangioma originating from the azygos vein arch.
Pathological findings
The tumor was dissected, which revealed enlarged and dilated thin-walled blood vessels with intact endothelial cells on the wall, in which the medial muscle layer was thinned; a large number of red blood cells were found outside the lumen. Multiple red blood cells were observed in the expanded blood vessel wall, composing the mural thrombus. Postoperative pathology confirmed hemangiomas (Figure 2).
MULTIDISCIPLINARY EXPERT CONSULTATION
A multidisciplinary consultation recommended surgical resection.
FINAL DIAGNOSIS
These results led us to a definitive diagnosis of hemangioma (Figure 2).
TREATMENT
The patient received thoracoscopic surgery. During the operation, it was found that the azygos vein arch was enlarged abnormally, showing dark purple cystic changes,and the mass was slightly adherent to the surrounding tissues. The azygos vein arch was ligated with silk thread near the superior vena cava (Figure 3A), and then the distal vessel of the tumor was ligated (Figure 3B). Finally, the tumor was resected completely (Figure 3C and D).
OUTCOME AND FOLLOW-UP
After the operation, the patient's back pain disappeared immediately, and her symptoms of dysphagia and chest tightness were also evidently relieved. The patient recovered well and was discharged on the seventh postoperative day. After careful follow-up for 10 mo, the patient was doing well without any discomfort.
DISCUSSION
Azygos vein aneurysms are rare clinical problems. They can be divided into primary and secondary azygos vein aneurysms. Hitherto, the pathogenesis of primary azygos vein aneurysms has not been clarified. Watanabeet al[1]speculated that the venous wall is congenitally weak or degenerative due to abnormal connective tissue at the anastomotic site between the proximal segment of the posterior main vein and the right superior main vein in the embryonic stage and then progresses to abnormally form azygos vein aneurysms. There are many secondary causes, including pseudoaneurysms caused by traumatic disruption, infection, portal hypertension, inferior vena cava occlusion, venous valve insufficiency, and local thrombosis[2-4]. Guoet al[5]reported a case of a giant azygos vein aneurysm caused by resection and embolization of a cavernous hemangioma of the chest wall and back. They believed that the pressure and volume load of the azygos vein were increased by surgery, which led to the expansion of the azygos vein.
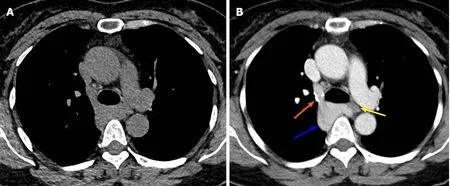
Figure 1 Tumor imaging by chest computed tomography. A: Chest computed tomography showed a soft-tissue mass in the right posterior mediastinum;the mass was approximately 4.2 cm × 3.7 cm × 2.6 cm in size and showed unclear boundaries with the esophagus and compression of the trachea; B: Enhanced scanning showed that the azygos vein arch widened, the contrast agent remained in the azygos vein arch, the tumor exhibited delayed enhancement, and the internal density was uneven (blue arrow). In the venous phase, the tumor was connected to the superior vena cava, and the degree of enhancement was the same as that of the superior vena cava. The boundary between the tumor and the esophagus was clear. Note the azygos vein valve (orange arrow). The esophagus was compressed by the azygos vein aneurysm (yellow arrow).
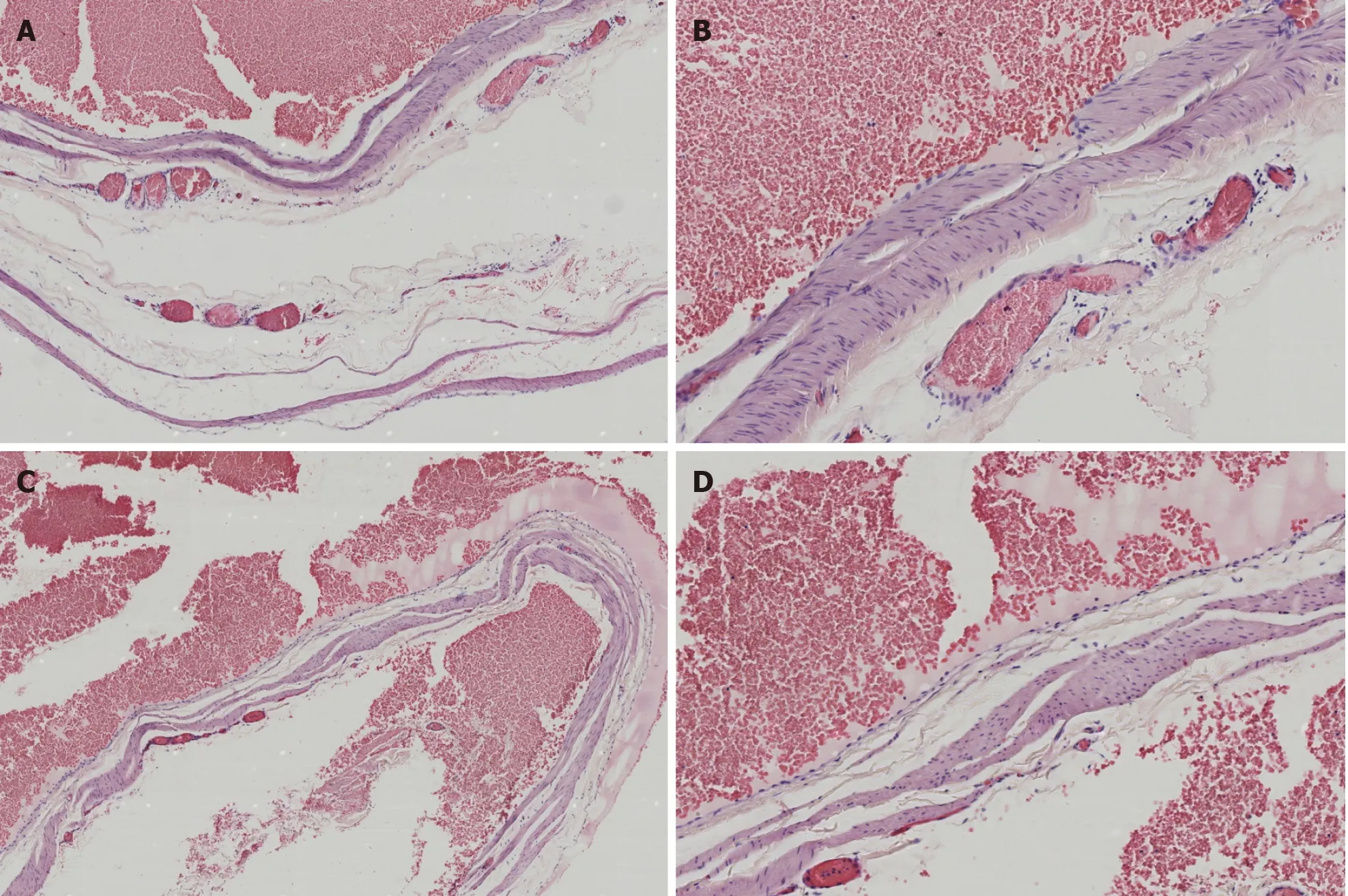
Figure 2 Hematoxylin and eosin staining. A and B: There were enlarged and dilated thin-walled blood vessels with intact endothelial cells on the wall, in which the medial muscle layer was thinned, and a large number of red blood cells were found outside the lumen (A: 40 ×; B: 100 ×); C and D: Multiple red blood cells were observed in the expanded blood vessel wall, composing the mural thrombus (C: 40 ×; D: 100 ×).
The overwhelming majority of patients with azygos vein aneurysms have no obvious clinical symptoms and are found to have the disease by physical examination or by chance[4,6-8]. A few patients have symptoms such as chest pain, choking, and cough[2,9]. However, our patient developed symptoms of back pain, chest tightness,and choking, probably because the esophagus and trachea were compressed by the azygos vein aneurysm, as shown by chest CT. After surgical resection, the abovementioned symptoms were evidently relieved, which forcefully confirmed our point of view. To the best of our knowledge, no such cases have been described in the literature; we report the first case of a patient with choking symptoms due to esophageal compression by an azygos vein aneurysm.
Azygos vein aneurysms should be differentiated from other mediastinal tumors,such as lymphomas, bronchial cysts, fibromas, and paragangliomas. Valuable examinations include chest CT scanning, enhanced CT scanning, angiography, nuclear magnetic resonance, nuclear magnetic resonance enhancement,etc.Some scholars believe that endobronchial ultrasound can show the blood flow of tumors more clearly, which is helpful for a definite diagnosis[10]. Interestingly, enhanced CT scanning of our patient showed nodular filling of contrast medium into the mediastinum of the azygos vein arch area. First, this was mistaken for lymph node calcification or old thrombus calcification in the azygos vein. After the analysis of CT scanning images by three-dimensional reconstruction, we found that the nodularity was due to the contrast agent flowing back into the azygos vein arch through the superior vena cava, but the contrast agent density did not decrease in the venous phase. This was considered to indicate the residual contrast agent in the azygos vein valve area. Ichikawaet al[11]reported that when a contrast agent was injected at high speed during enhanced CT scanning, the phenomenon of reflux of contrast medium from the superior vena cava to the azygos vein arch may sometimes be observed,resulting in residual contrast agent in the azygos vein arch valve. This phenomenon can also occur in the normal population, and it is more likely to occur when the contrast agent is injected into the right upper limb. In summary, the right posterior mediastinal tumor should be identified carefully before the operation, and the possibility of an azygos vein aneurysm should be considered to avoid the risk of bleeding caused by puncture biopsy.
It is generally believed that azygos vein aneurysms do not require special treatment[2,6], but some scholars believe that tumor rupture with the progression of the disease[12]and thrombosis may lead to pulmonary embolism[2,7]. In addition, tumors in this area also pose potential malignant risks. Dasikaet al[13]and De Palmaet al[14]reported cases of leiomyosarcoma of the azygos vein and epithelioid hemangioendothelioma, respectively, and they advocated aggressive surgical therapy. Savuet al[15]reported that in cases of azygos venous aneurysm with complete thrombosis,surgery was recommended and must be performed with extreme care in order to prevent intraoperative embolism. Our patient had symptoms of back pain, chest tightness, and choking. It was believed that the tumor was caused by compression of the esophagus and trachea, so we actively adopted surgical therapy. After the operation, we observed that the blood vessel wall of the tumor became thinner, and mural thrombosis was found inside. We speculate that this may have been due to the formation of vortices in the blood flow through the hemangioma, where the blood flow slowed down, leading to thrombosis, which also confirms Nakamuraet al[2]'s point of view. Therefore, we believe that it is necessary for azygos vein aneurysms to be treated by surgical resection.
The wall of the azygos vein aneurysm is weak, and there is a risk of rupture and bleeding during the operation. Traditional thoracotomy or endoscopic-assisted small incisions were adopted previously[16]. With the progress of endoscopic technology,totally thoracoscopic surgery has also been reported in recent years[4,6]. Ma and his colleagues[4]described the performance of thoracoscopic surgery, including avoiding unnecessary manipulation (pinching or pressing) of the masses to prevent bleeding complications. The proximal end of the hemangioma should be treated first to prevent the thrombus from entering the superior vena cava and right atrium and forming pulmonary embolism. We learned from their experience during the operation and achieved good therapeutic effects.
CONCLUSION
In conclusion, a right posterior mediastinal mass should be considered for the possibility of an azygos vein aneurysm. Some patients may experience dysphagia and chest tightness due to esophageal and tracheal compression caused by the tumors.Enhanced CT scanning is vital for the diagnosis of azygos vein aneurysms. In addition,despite the difficulty and risk of the operation, thoracoscopic surgery for azygos vein aneurysms is completely feasible.
ACKNOWLEDGEMENTS
We thank Professor Liu YX and Dr. Zhang LC for their help during the research process.
 World Journal of Clinical Cases2021年11期
World Journal of Clinical Cases2021年11期
- World Journal of Clinical Cases的其它文章
- Endoscopic diagnosis of early-stage primary esophageal small cell carcinoma: Report of two cases
- Melatonin for an obese child with MC4R gene variant showing epilepsy and disordered sleep: A case report
- Contrast-enhanced ultrasound using SonoVue mixed with oral gastrointestinal contrast agent to evaluate esophageal hiatal hernia:Report of three cases and a literature review
- Rare histological subtype of invasive micropapillary carcinoma in the ampulla of Vater: A case report
- Calcium pyrophosphate deposition disease of the temporomandibular joint invading the middle cranial fossa: Two case reports
- Cholangiojejunostomy for multiple biliary ducts in living donor liver transplantation: A case report