Study on the quality of life and its related factors for older adults in communities in Beijing, China?
2021-06-24 03:10:38YuLiuRoinWhittemoreHongGuoYnChenWeiZhngQioHe
Frontiers of Nursing 2021年2期
Yu Liu, Roin Whittemore, Hong Guo, Yn Chen, Wei Zhng, Qio He
aSchool of Nursing, Beijing University of Chinese Medicine, Beijing 100029, China
bSchool of Nursing, Yale University, New Haven, CT 06520, USA
cRehabilitation Department, Zhejiang Provincial People’s Hospital, Hangzhou, Zhejiang 310014, China
Abstract: Objectives: To describe the quality of life (QOL) of adults ≥60 years of age in communities in Beijing and explore demographic, clinical,and psychological factors associated with QOL.
Keywords: community ? depressive symptoms ? older adults ? quality of life
1. Introduction
With the improvement of socioeconomic status and the significant increase in life expectancy in China (from 67.77 years old in 1981 to 74.83 years old in 2010),1the number and proportion of the older adult population are increasing rapidly. By the end of 2014, the population of older adults (≥60 years) in China had reached 212 million, which was 15.5% of the total population.2According to the United Nations standards, a society in which >10% of people are over age 60 is regarded as an aging society; thus, China is an aging society. By 2050, the older adult population of China is projected to be 32.8% of the total population.3The rapidly aging population has caused challenges to the Chinese social security system, including changes in family and social structures, an increased burden of illness, and the risk of disability.4
In 2002, the World Health Organization put forward the concept of “active aging,” which is defined as the process of optimizing opportunities for health, participation, and security to enhance the quality of life (QOL) as people grow older.5QOL is a multi-dimensional, subjective, and dynamic phenomenon. In the context of the likely physical decline of the older adult, understanding and maintaining their QOL has been the pursuit of research in the past decade. For example, in a crosssectional survey in Brazil, the QOL of older men had the highest score in the social relations domain and the lowest score in the physical domain; functional disability had the strongest influence on their QOL.6Research on the QOL of the older adult may inform health care practice and policies for an aging population.
Understanding the factors that influence QOL in older adults is also important to identify those at risk.In Korean older adults, regular assessments of physical, cognitive, and other functions of older adults, with early detection and intervention, enhanced their QOL.7In a large study of older adults of Li ethnic regions in the southeast province of China, factors influencing better QOL in older adults included urban living, less chronic disease, regular exercise, the good living status of their children, being younger, and high income.8Increased depressive symptoms are common among older adults9and can negatively influence QOL.10Other factors, such as marital status and educational background, have been shown to influence the QOL of older adults.11However, most of the research on QOL of older adults focuses on those with chronic diseases12or a component of QOL, such as social relations or psychosocial aspects,13whereas less number of researches addresses overall QOL of community-dwelling older adults.
Synthesizing the research on the QOL of older adults in China is challenging because numerous self-report instruments are used to evaluate QOL. The 36-item short form (SF-36) is widely used for measuring healthrelated QOL in various settings internationally and it has been translated and validated in many languages. The Chinese version of the SF-36 has demonstrated good psychometric properties.14Despite the widespread use of the SF-36 worldwide, there has been little research evaluating the QOL for the Chinese older adult population. As a consequence, there has been limited understanding of the current status of the QOL in older adults and little understanding of how the QOL in Chinese older adults is similar or different to those in other countries. The purpose of this study was to describe the QOL of the older adults >60 years of age in communities in Beijing, the capital city of China, and compare the QOL between men and women as well as oldervs.younger adults. We also determined whether demographic and clinical characteristics and depressive symptoms were associated with QOL in older adults in China.
2. Methods
2.1. Sampling
This was a cross-sectional study. Older adults in two communities of Beijing were recruited through convenience sampling. In August 2014, we obtained Inspection Review Board (IRB) approval from a university in Beijing and the Residents’ Committee (RC)of two communities of Chaoyang District, Beijing,for poster recruitment inviting older residents to participate in the study. The RC is an autonomous and special non-governmental organization at the grassroots level with the characteristics of an autonomous administration, self-discipline, and self-service.RC is responsible for public affairs and public welfare issues of the community residents and is made up of 5–9 persons selected by the residents in the community. Inclusion criteria of this study were ≥60 years old,resident in a community of Beijing for >1 year, no history of a psychiatric disorder, and no prescription for psychotropic drugs in the past month. Exclusion criteria were hospitalization at the time of the investigation.
From August 2014 to July 2015, 363 older adults came to the community health service station and completed the study questionnaires. We removed invalid questionnaires of 50 (13.77%) older adults due to missing data, and we obtained the completed questionnaires of 313 (86.23%) older adults.
2.2. Data collection
Before data collection, trained research assistants verbally explained the study and participants signed a consent form in Chinese. All participants were asked to complete the questionnaire after obtaining their informed consent. For participants with low education or poor vision, investigators explained and read the questionnaire items one by one and recorded the participant’s responses. The participants were offered a free blood pressure check-up in appreciation for their participation.
2.3. Measurements
Data were collected on demographic and clinical characteristics, depressive symptoms, and QOL.
2.3.1. Demographic and clinical questionnaire
Demographic data included age, gender, marriage status, vocation, and salary. Clinical data on self-reported chronic diseases, such as diabetes, cardiac disease,hypertension, stroke, and rheumatoid arthritis, were also collected.
2.3.2. Self-Rating Depression Scale (SDS)
Depressive symptoms were assessed using the SDS,a 20-item self-administered questionnaire evaluating depressive symptoms,15developed in China. There are ten positively worded and ten negatively worded sentences. Items, such as “I feel downhearted and blue” and “I have trouble sleeping at night”, are scored from 1 (where symptoms are very seldom) to 4 (where symptoms are most of the time). The score of individual items is summed as a total score, then multiplied by 1.25 to get the standard score. According to the Chinese norm of SDS, depression is defined as a score of 53 or higher on the SDS.16The split-half reliability coefficient of SDS (Chinese version) was 0.73 and Cronbach’s alpha was 0.80.17The Cronbach’s alpha was 0.82 in our sample.
2.3.3. Medical outcomes study SF-36
The SF-36 is a self-reported survey of a person’s health and QOL. The SF-36 consists of eight subscales that include physical functioning, physical role functioning, vitality, bodily pain, general health perceptions,emotional role functioning, social role functioning,and mental health. Each subscale is transformed into a 0–100 scale on the assumption that each question carries equal weight and scored with weighted sums of the questions in its section. Higher scores on the SF-36 reflect better QOL. There are two subscales of the SF-36: a physical health dimension, represented by the physical component summary (PCS), and a mental health dimension, represented by the mental component summary (MCS). All the subscales contribute in different proportions to the scoring of both PCS and MCS.18Cronbach’s alpha of all the subscales in this study was between 0.77 and 0.81.
2.4. Statistical analyses
Descriptive statistical analysis included frequencies,means, and standard deviations. Thet-test and ranksum test (Mann–WhitneyUtest) were used to compare the QOL by gender and age group. To identify factors associated with QOL, bivariate analyses were initially assessed using Spearman’s Correlation coefficient. The variables significantly associated with QOL (p< 0.05)were included in a multiple linear regression model using the stepwise method. The PCS and MCS of the SF-36 were used as dependent variables, respectively.All the data were analyzed using SPSS 17.0 and using a statistical significance ofp< 0.05. A sample of 144 participants was needed to detect a populationR2of 0.10 using 8 predictors, with a 0.80 power.
Missing values of SF-36 or SDS in a questionnaire>10% were regarded as invalid. Among 363 participants, 50 were removed for this reason. In 313 valid participants, 21 had missing values in SF-36 or SDS<10%, and mean substitution was used for the missing values.
3. Results
3.1. Sample
Participants’ age ranged from 60 to 96 years, with a mean age of 72.96 ± 9.36 years, 56.5% of the participants had chronic diseases, 85.3% had an education background less than a high school level, and 47.6%were workers. The demographic characteristics of the sample are presented in Table 1.
The mean SDS score of 313 participants was 43.23 ± 10.34 and the prevalence of self-reported depressive symptoms (score >criterion score of 53)was 16.6%.
3.2. QOL for 313 older adults
The mean scores and standard deviations of the 8 subscales, PCS, and MCS of the SF-36 for 313 older adults are provided in Table 2 along with the U.S. normative data.19Chinese older adults had higher QOL in the domains of social role functioning and emotional role functioning, whereas they had lower QOL in the domains of physical functioning and general health perceptions. Chinese older adults also demonstrated higher QOL compared with the U.S. older adults across most subscales.
There were no significant differences in QOL between Chinese women and men. However, there were significant differences between different age groups of older adults (Table 3). The older the participants, the lower the PCS score (lower physical QOL)and the higher the MCS score (better mental QOL).Figure 1 illustrates the differences in the PCS and MCS of the SF-36 by age group.
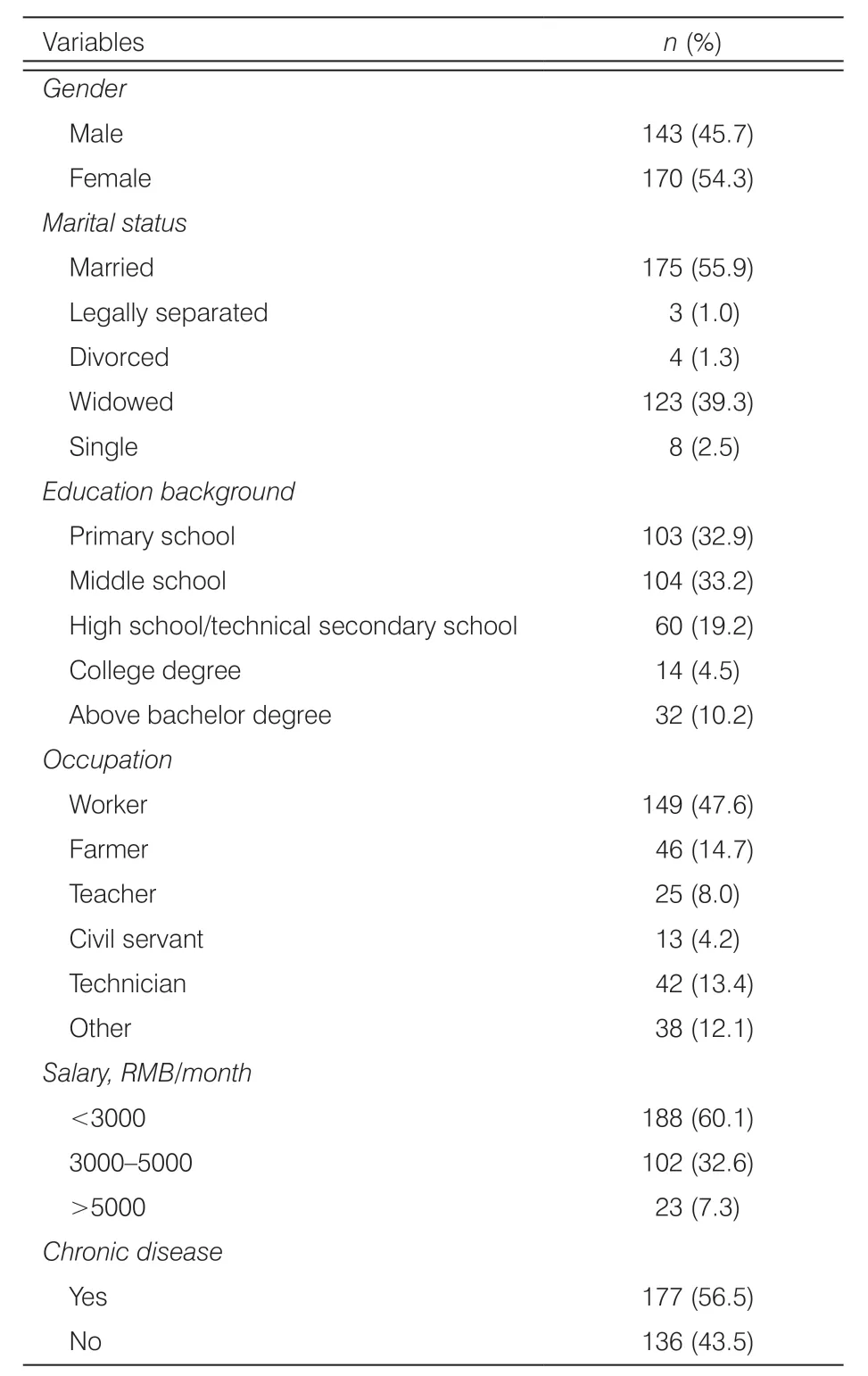
Table 1. Demographic characteristics of 313 older adults.
3.3. Factors related to QOL for 313 older adults
A correlation analysis was performed to evaluate variables associated with the PCS and MCS subscales of the SF-36. The PCS was associated with age, marital status, chronic disease, and SDS scores (r= -0.318,-0.325, -0.138, and -0.425). The MCS was associated with age, chronic disease, and SDS scores (r= 0.136,-0.325, and -0.416).
The variables significantly correlated with PCS in the bivariate analysis were included in a multiple linear regression model as independent variables. In the multivariate analysis, depressive symptoms, marital status, and age were associated with PCS (Table 4). Better physical QOL was associated with less depressive symptoms, having a partner, and younger age, explaining 28.7% of the variance. In the multivariate analysis for MCS, depressive symptoms, chronic disease, and age were associated with MCS (Table 4). Better mental health in QOL was associated with less depressive symptoms, no chronic disease, and older age, explaining 34.7% of the variance.
4. Discussion
We surveyed 313 older adults in two communities in Beijing and found that there was no significant difference in QOL between men and women. However, there were differences in both physical and mental QOL concerning age. With aging, physical QOL was lower and mental QOL was better. The decline of physical health in older adults is accordant with the decline of physiologicalfunction associated with age. In contrast, mental QOL may be influenced by less anxiety and more life satisfaction with age, despite declining physical health. In a survey of older adults in 7 cities in China, increased age was associated with feelings of calmness and satisfaction, and this status seemed to have a linear trend over time. As adults age, their satisfaction with families’ material life may increase and they understand more about the Chinese proverb “happiness consists in contentment.”20It is noteworthy that Beijing is the capital city of China and people experience a competitive life here,especially for young and middle-aged adults.21Many young and middle-aged adults have role strain balancing work, family, and children, so often they seek support from their parents, which may make their parents,most of them being in the younger older age group,feeling stress. In a large survey of adults in 7 provinces in China, age was associated with a lower risk of older adults being responsible for helping their young adult children. Older adults >75 years old were significantly less likely to be caring for their young adult families than those aged 60–64 years (odds ratio: 0.522).22This may help to explain why younger old adults have lower mental QOL than older old adults in our study.
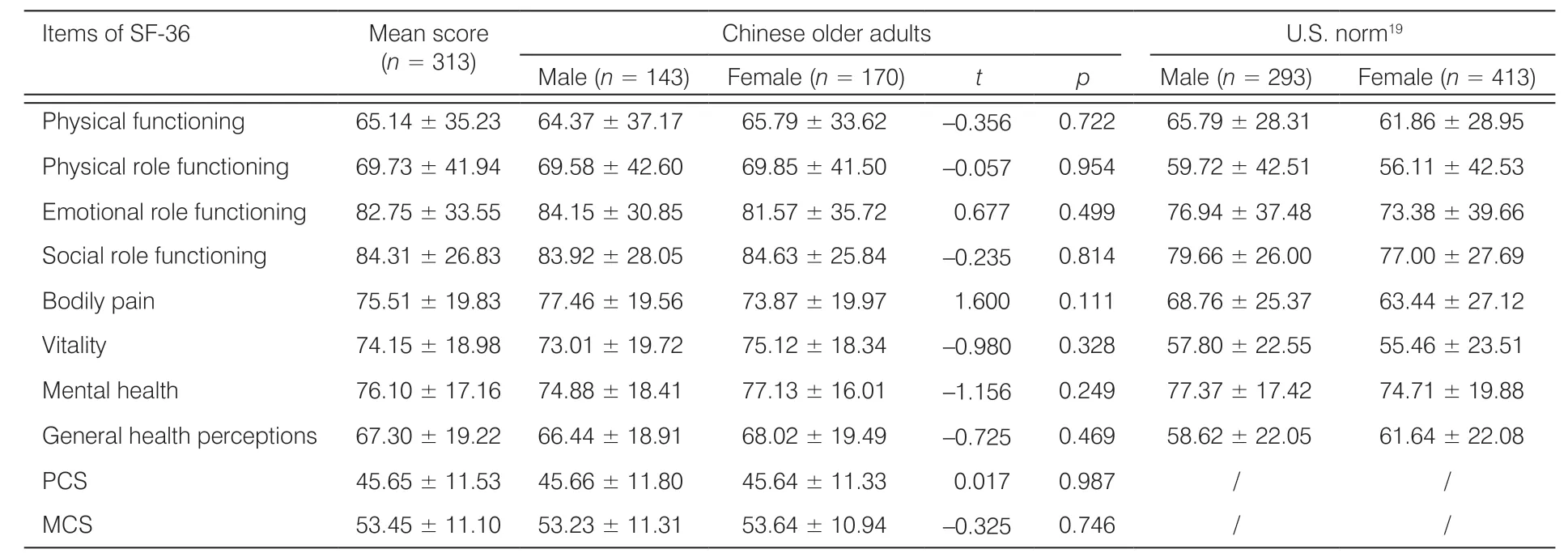
Table 2. Mean SF-36 scales score by gender.
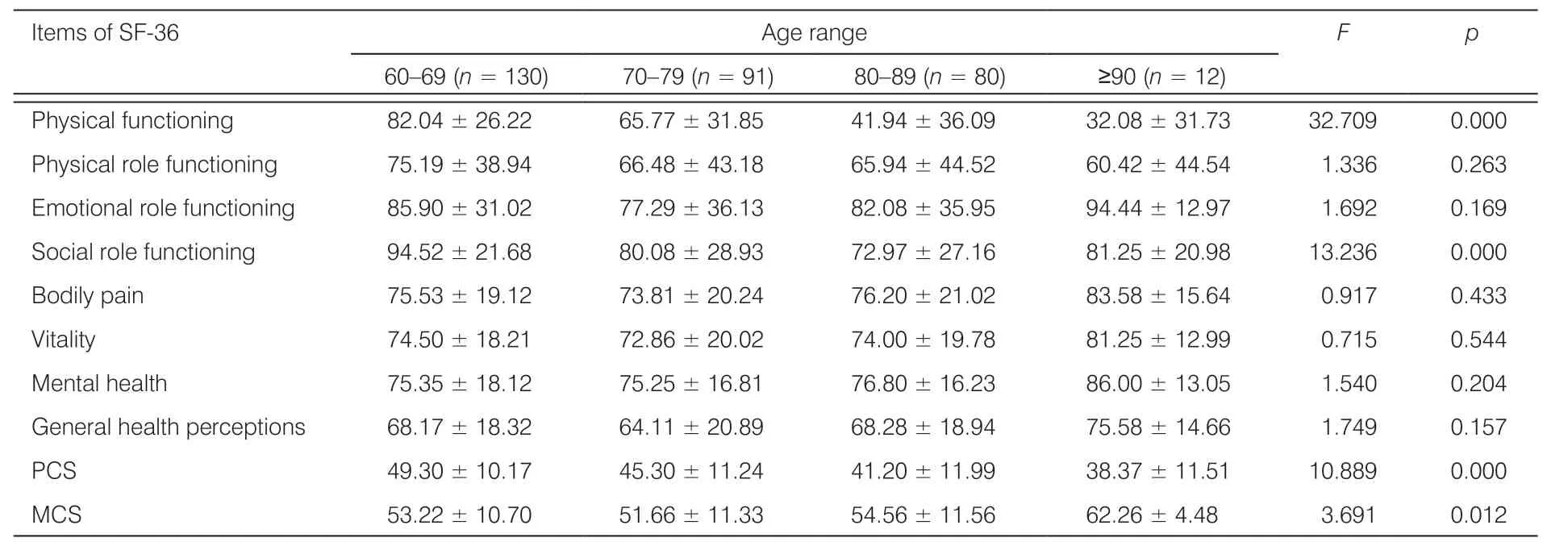
Table 3. Mean SF-36 scales score by age.
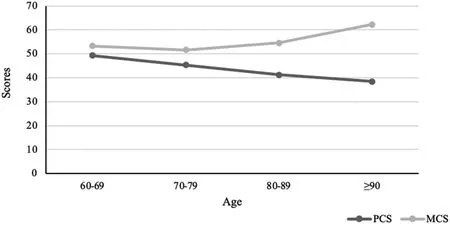
Figure 1. The difference in PCS and MCS of SF-36 in 313 older adults by age group.
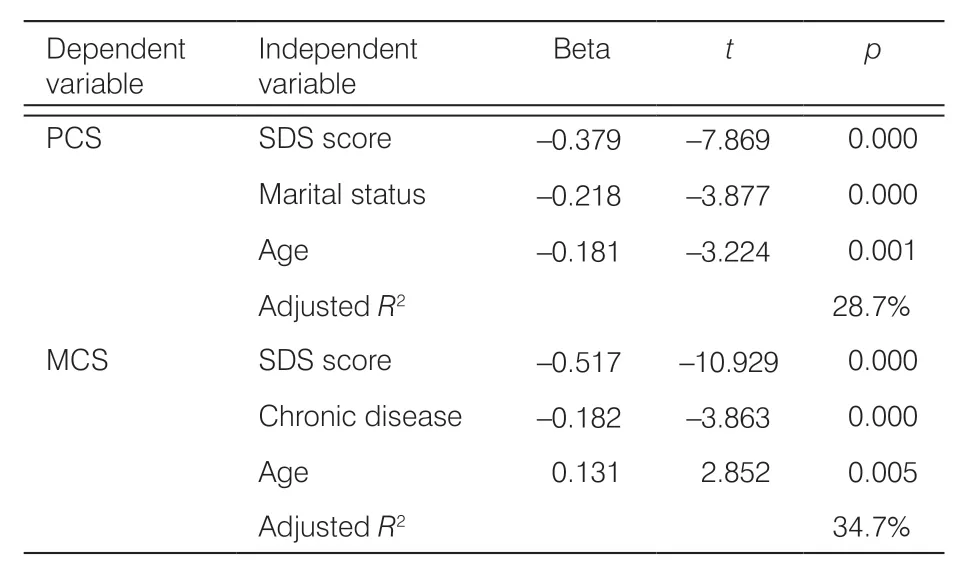
Table 4. Multiple linear regression analyses predicting PCS and MCS of SF-36 in 313 older adults.
Overall QOL in Chinese older adults was better than older adults in the U.S., which may be caused by a cultural difference with the elderly more respected in the Chinese society. In addition, the Chinese sample lived in Beijing where most older adults live with their families,23which may contribute to less isolation and better QOL.
Factors that influence QOL in older adults were also identified in this study. Depressive symptoms exerted a negative impact on both physical and mental QOL in the older adult in Beijing. With more depressive symptoms, older adults had lower physical and mental QOL. This finding was following a study in Brazil that used the WHOQOL-100 to survey older adults’ QOL.24While it has been reported that older adults have a higher risk for increased depressive symptoms,25the prevalence of self-reported depressive symptoms in older adults in this study was 16.61%, which is lower than previously reported in China about 40%.26The mean of the SDS scores in this sample was 43.23,similar to 41.88 in the Chinese norm,27which indicates that the severity of depression symptoms in this group was relatively low.
In this study, marital status had a positive impact on the physical QOL of the older adult, such that, older adults who had a spouse or partner experienced a higher level of physical QOL than those divorced or widowed or single, which has been supported in other research.28In old age, the frequency of interaction with friends reduces and the older adults’ life can become increasingly dependent on family members, especially their spouses. The older spouse may play a major role in the care of his wife/her husband in China and this caring and support may prevent their physical health and physical QOL from declining. Besides, elderly couples often play a role as a family authority according to Chinese tradition, thus, they can arrange family members to care for them and coordinate the factors that affect them.29
Previous studies on Chinese older adults have indicated that chronic diseases have an impact on overall QOL in the older adults,30but in our study, chronic disease was associated with lower mental QOL, but not physical QOL. A chronic disease may contribute to body pain or functional disability affecting activities of daily living, which may cause anxiety or depression.31If an older adult has a negative or pessimistic assessment about their health due to chronic diseases, it may have psychological consequences, thereby affecting their mental QOL. Thus, focusing on both the mental and physical QOL of older adults is important, particularly if they have a chronic disease.
5. Conclusions
In conclusion, the physical QOL of older adults in Beijing was lower and mental QOL was better with aging. Less depressive symptoms, having a spouse or partner, and young-old age were associated with better physical QOL of the older adult; and less depressive symptoms,no chronic disease, and older age were associated with better mental QOL. Assessment of QOL in older adults may be warranted and community-based strategies to encourage healthy lifestyles and social interaction, particularly older adults may improve physical and mental QOL. Since the SF-36 has been used widely in other countries, our result provides the feasibility to compare the data from different countries and populations with the same tool.
Several study limitations should be taken into account when interpreting these results. First, since there are regional differences in the development of the social economy in China, the relatively small sample size covering only the capital city of China and the convenience sampling may limit the generalization of findings in this study. Second, considering that there are many potential factors related to the older adults’ QOL, the factors included in this study were limited, and chronic diseases need classifying to recognize their different effects on the QOL. Finally, almost half of the participants had diabetes, which may influence evaluating the older adult’s QOL. Despite these limitations, this study provides important descriptive data on the QOL in older adults in China. Assessment and treatment of depressive symptoms, prevention of chronic disease,and healthy relationships appear necessary to enhance QOL in older adults.
Ethical approval
This article obtained Inspection Review Board (IRB)approval from a university in Beijing and the Residents’ Committee (RC) of two communities of Chaoyang District, Beijing, for poster recruitment inviting older residents to participate in the study.
Conflicts of interest
All contributing authors declare no conflicts of interest.
- Frontiers of Nursing的其它文章
- Frontiers of Nursing Call for Papers
- A conceptual analysis of the meaning of comfort at the end-of-life using the Walker and Avant (2014) Framework
- Research on teaching reform of rehabilitation nursing major based on modern apprenticeship system?
- Association between calcium supplementation and bone mineral density in children: a systematic review and meta-analysis
- Evaluation of undergraduate students’ nursing assessment and communication skills through an objective structured clinical examination within a high-fidelity simulation using a student-simulated patient?
- The effectiveness of dalethyne dressings for reducing bacteria in diabetic foot ulcers