Clinical observation on moxibustion therapy plus tuina in treating children with recurrent respiratory tract infections due to qi deficiency of spleen and lung
2021-10-27 08:27:32XiaYun夏云CaoZhiliang曹徵良LiuYinghan劉英含LouBidan婁必丹ZhangWei章薇
Xia Yun (夏云), Cao Zhi-liang (曹徵良), Liu Ying-han (劉英含), Lou Bi-dan (婁必丹), Zhang Wei (章薇)
The First Hospital of Hunan University of Chinese Medicine, Changsha 410007, China
Abstract
Keywords: Moxibustion Therapy; Tuina; Massage; Pediatric Massage (Tuina); Respiratory Tract Infections; Qi Deficiency of Spleen and Lung; Child, Preschool
Children’s recurrent respiratory infections (RRTI) refer to repeated respiratory infections in children within a year, and the incidence is significantly higher than that in normal children of the same age, and exceeds a certain range[1]. RRTI is a common pediatric disease, with an increasing incidence in recent years. According to statistics, about 60.0% of pediatric outpatients in China have respiratory tract infections, and 30.0% of the cases are RRTI[2]. The disease is mainly manifested as recurrent respiratory tract infections, including cold,bronchitis and pneumonia, and the course of disease is long and easy to recur, which will affect the physical growth and development of the children, and even affect their physical and mental health[3]. Pediatric massage(tuina), as a characteristic therapy of traditional Chinese medicine (TCM), is increasingly used in the clinical treatment of children with RRTI. It has definite curative effect and can also avoid the suffering caused by acupuncture and medication. In this study, 60 children with RRTI were taken as the research objects, and the clinical efficacy of moxibustion therapy plus Liu’s pediatric massage for RRTI was observed.
1 Clinical Materials
1.1 Diagnostic criteria
1.1.1 Criteria for syndrome differentiation in TCM
According to thePediatrics in Chinese Medicine[4]andClinic Terminology of Traditional Chinese Medical Diagnosis and Treatment-Syndromes(GB/T 16751.2-1997)[5], the criteria for syndrome of qi deficiency of spleen and lung in this study were established. Primary manifestations: recurrent exogenous disease, or easily recurrent after recovery. Secondary manifestations:yellowish and lusterless complexion, easy to sweat,spontaneous or night sweating, flabby muscles, poor appetite, lassitude and weakness. Tongue and pulse/infantile venule of the index finger: a pale tongue,thready and weak pulse, and thin superficial veins on the index finger.
1.1.2 Diagnostic criteria in Western medicine
This study referred the diagnostic criteria for RRTI inZhu Futang Textbook of Pediatrics[6]: the interval between two consecutive upper respiratory tract infections is more than 7 d; if the number of times of the upper respiratory tract infections is not enough, the times of upper and lower respiratory tract infections can be added, otherwise it cannot be added; continuous observation for 1 year to determine the incidence; the diagnosis of pneumonia requires lung signs such as dry or moist rales in the lungs and imaging data such as chest X-ray or CT examination (Table 1).
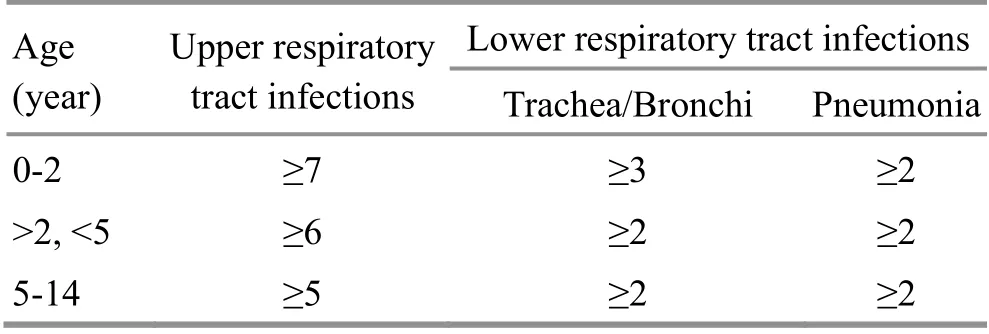
Table 1. Criteria for the number of times of respiratory tract infections in one year (time/year)
1.2 Inclusion criteria
Those who met the above diagnostic criteria for RRTI,during remission period; aged 1 to 6 years old in either gender; no history of Chinese or Western medicine treatment related to this disease in the past 1 month before enrollment; whose guardians agreed to accept the clinical study, and signed informed consent.
1.3 Exclusion criteria
Those who had acute respiratory tract infections; who had other severe diseases (such as heart, brain,respiratory system, liver, kidney and other systemic diseases); with local skin lesion, bleeding or infections;combined with hematological diseases and prone to bleeding; those who were unable to cooperate during moxibustion.
1.4 Elimination and dropout criteria
Those who or whose guardians did not cooperate to receive the prescribed treatment during the trial; who had severe adverse reactions such as burn that was improper to continue the trial; those who dropped out;those lost contact during follow-up.
1.5 Statistical methods
All data were statistically analyzed by the SPSS version 22.0 statistical software. Measurement data were all in normal distribution, and thus expressed as mean ±standard deviation (±s), with pairedt-test applied for the intra-group comparison, and independent samplettest applied for the comparisons between the groups.Counting data were processed by Chi-square test. Ranksum test was applied for the comparison of ranked data.P<0.05 was considered to indicate a statistically significant difference.
1.6 General data
Children diagnosed with RRTI were all enrolled from Pediatric Outpatient Department and Pediatric Massage Center of the First Hospital of Hunan University of Chinese Medicine, between December 2018 and June 2019. All patients were divided into an observation group and a control group according to the visiting sequence, with 30 cases in each group. There were no statistically significant differences in the general data between the two groups (allP>0.05), indicating that the two groups were comparable (Table 2).
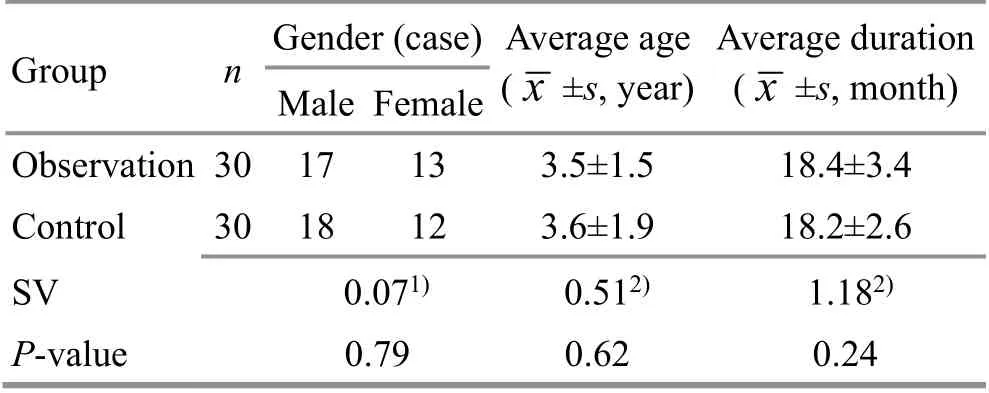
Table 2. Comparison of general data between the two groups
2 Treatment Methods
2.1 Observation group
Children in the observation group were treated with moxibustion therapy and Liu’s pediatric massage.2.1.1 Moxibustion therapy
Acupoints: Shenzhu (GV 12), Feishu (BL 13) and Pishu(BL 20) were the first group; Zhongfu (LU 1), Qihai (CV 6)and Zusanli (ST 36) were the second group.
Materials: Small moxa cones.
Methods:The child took a prone or supine position.After ignited, the moxa cone was placed on the acupoints to apply moxibustion. It was appropriate to have a warm and comfortable feeling in the local area until there slight flushed at local area (Figure 1).
Treatment course: The moxibustion took 1 moxa-cone at each acupoint, and was performed every other day.Thirty days constituted 1 treatment course, and a total of 3 courses were performed. Follow-up was conducted at 6 months after treatment.

Figure 1. Moxibustion therapy
2.1.2 Liu’s pediatric massage
Opening the orifices: Kai-opening Tianmen, Tuipushing Kangong, Tui-pushing Taiyang (EX-HN 5), Qiapinching Zongjin, Fen-parting Hand Yinyang, 24 times for each (Figure 2-Figure 6).
Tui-pushing Wujing: Bu-reinforcing Pijing 250 times,Bu-reinforcing Feijing 300 times, Qing-clearing Ganjing 150 times, Qing-clearing Xinjing 100 times, Bureinforcing Shenjing 150 times (Figure 7-Figure 11).

Figure 2. Kai-opening Tianmen

Figure 3. Tui-pushing Kangong

Figure 4. Tui-pushing Taiyang (EX-HN 5)

Figure 5. Qia-pinching Zongjin

Figure 6. Fen-parting Hand Yinyang

Figure 7. Bu-reinforcing Pijing

Figure 8. Bu-reinforcing Feijing

Figure 9. Qing-clearing Ganjing
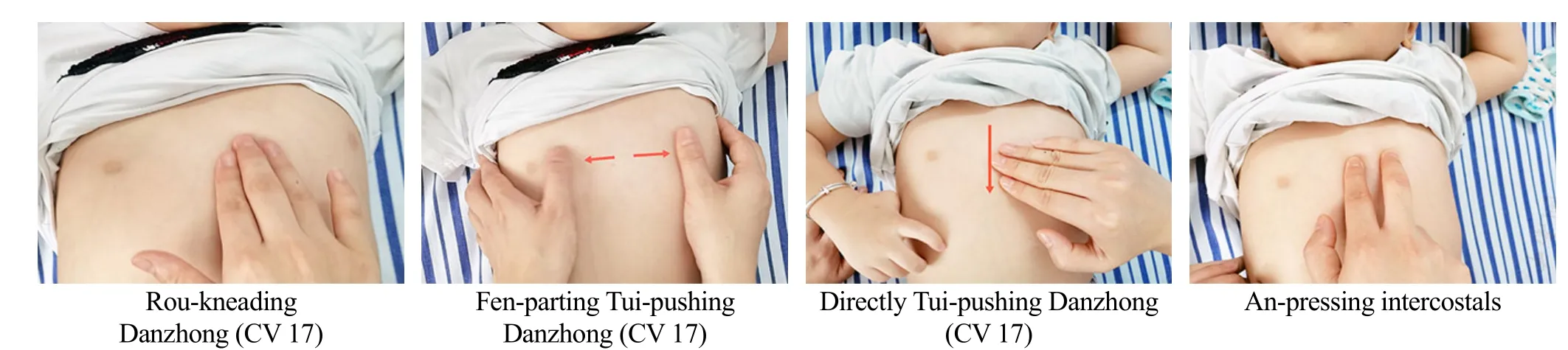
Figure 12. Tui-pushing chest manipulation

Figure 10. Qing-clearing Xinjing

Figure 11. Bu-reinforcing Shenjing
Points combination: Tui-pushing chest manipulation[Rou-kneading Danzhong (CV 17), Fen-parting Tuipushing Danzhong (CV 17), directly Tui-pushing Danzhong (CV 17), An-pressing intercostals, 60 times for each], Rou-kneading Zhongwan (CV 12) 120 times, Anpressing and Rou-kneading Zusanli (ST 36) 100 times, Tuipushing, Rou-kneading and Ca-scrubbing Feishu (BL 13)until the skin turned red (Figure 12-Figure 15).
Closing the orifices: Na-grasping Jianjing (GB 21)3-5 times (Figure 16).

Figure 13. Rou-kneading Zhongwan (CV 12)

Figure 14. An-pressing and Rou-kneading Zusanli (ST 36)

Figure 15. Tui-pushing, Rou-kneading and Ca-scrubbing Feishu (BL 13)

Figure 16. Na-grasping Jianjing (GB 21)
Treatment course: Massage was performed every other day, 3 times/week, and 4 weeks as a course, for a total of 3 courses.
2.2 Control group
The control group was treated with Liu’s pediatric massage same as that in the observation group,including the specific acupoints, manipulation methods and treatment course.
3 Observation of Curative Efficacy
3.1 Observation items
The frequencies of respiratory tract infections before treatment and at 6 months after treatment were counted, including the upper and lower respiratory tracts, and the TCM symptoms score of the children.
TCM symptoms score was evaluated by scoring method, including recurrence, complexion, body shape,sweating, fatigue, shortness of breath, and diet.According to the manifestations, it was divided into 4 grades: normal, mild, moderate and severe, scored 0, 2,4, and 6 points, respectively. The symptom score was recorded 6 months before and after treatment, and compared.
3.2 Criteria for curative efficacy
According to the diagnosis and treatment protocols of RRTI in theDiagnosis and Treatment Protocols of Traditional Chinese Medicine for 22 Professionals and 95 Diseases[7], the criteria for curative efficacy in this study were established.
Clinically cured: During the 6-month follow-up, the incidence of infections in children with RRTI was consistent with the standard for normal children of the same age.
Markedly effective: During the 6-month follow-up, the total times of infections in children with RRTI decreased by more than 2/3.
Effective: During the 6-month follow-up, the total times of infections in children with RRTI decreased by 1/3-2/3 on average.
Invalid: During the 6-month follow-up, the total times of infections in children with RRTI decreased by less than 1/3 on average.
3.3 Treatment results
3.3.1 Comparison of clinical efficacy
At the 6-month follow-up, the difference in clinical efficacy between the two groups was statistically significant (P<0.05), indicating that moxibustion therapy plus Liu’s pediatric massage had better efficacy in treating children with RRTI than Liu’s pediatric massage alone (Table 3).

Table 3. Comparison of clinical efficacy between the two groups (case)
3.3.2 Comparison of TCM symptoms score
There was no statistical difference in the TCM symptoms score between the two groups before treatment (P>0.05). After treatment, the scores in both groups decreased, and were statistically different from those in the same group before treatment (bothP<0.05),indicating that the treatment protocol of both groups could improve the TCM symptoms in children with RRTI.The difference in TCM symptoms score before and after treatment in the observation group was statistically different from that in the control group (P<0.05),indicating that moxibustion therapy plus Liu’s pediatric massage had a better effect in improving clinical symptoms in children with RRTI (Table 4).3.3.3 Comparison of the incidence
There was no statistical difference in the incidence between the two groups before treatment (P>0.05).After treatment, the incidences in both groups reduced,and were statistically different from that in the same group before treatment (bothP<0.01), indicating that the treatment protocol of both groups could reduce the incidence in the children. The difference in the incidence before and after treatment in the observation group was statistically different from that in the control group(P<0.05), indicating that moxibustion therapy plus pediatric massage could better reduce the incidence of RRTI in children (Table 5).
Table 4. Comparison of TCM symptoms score between the two groups ( ±s, point)

Table 4. Comparison of TCM symptoms score between the two groups ( ±s, point)
Note: Compared with the same group before treatment, 1) P<0.01,2) P<0.05; compared with the control group, 3) P<0.05
Group n Before treatment After treatment Difference Observation 30 11.67±3.44 6.00±1.791) 3.45±0.673)Control 30 11.00±2.10 8.67±1.632) 2.33±1.51
Table 5. Comparison of the incidence between the two groups( ±s, number)
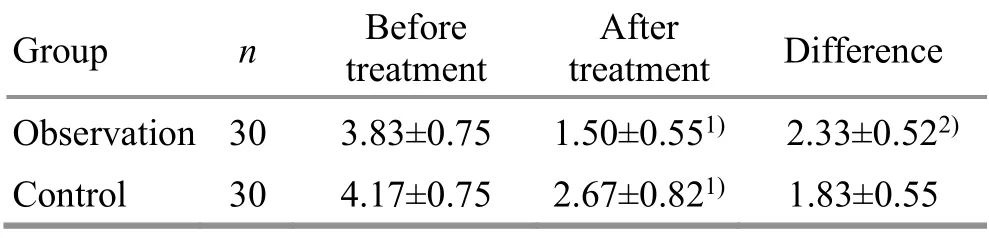
Table 5. Comparison of the incidence between the two groups( ±s, number)
Note: Compared with the same group before treatment, 1) P<0.01;compared with the control group, 2) P<0.05
Group n Before treatment After treatment Difference Observation 30 3.83±0.75 1.50±0.551) 2.33±0.522)Control 30 4.17±0.75 2.67±0.821) 1.83±0.55
4 Discussion
The development of RRTI is related to deficiency, low autoimmunity or environmental factors[8-9]. The prevention methods in Western medicine are limited.For children with RRTI during remission period, the prevention is mainly based on immunomodulators or trace elements[10].
TCM has advantages in the prevention and treatment of RRTI. RRTI belongs to exogenous disease in TCM. It is believed that its causes are congenital deficiency of lung and spleen and inappropriate diet and nursing. The treatment is mainly based on invigorating Yuan-Primordial qi and consolidating the constitution, focusing on regulating and reinforcing qi of Zang-fu organs,through benefiting qi for protecting exterior, or harmonizing the Ying-nutrient and Wei-defensive qi, or invigorating kidney and strengthening the body[11].
In this study, we used pediatric moxibustion combined with Liu’s pediatric massage to treat RRTI. Pediatric moxibustion can be directly attached to the skin for moxibustion. It is convenient, safe and effective. Modern studies have also confirmed that moxibustion can improve the immune function by regulating the immune organs[12-13], immune cells[14-15], immune regulatory factors[16], and immunoglobulins[17]. In this study,Shenzhu (GV 12), Feishu (BL 13), Pishu (BL 20), Zhongfu(LU 1), Qihai (CV 6) and Zusanli (ST 36) were selected.Feishu (BL 13) is the Back-Shu point of the lung. It can disperse the lung qi to calm panting, regulate qi to supress cough and dissipate phlegm. Zhongfu (LU 1) is the Front-Mu point of the lung, and it can suppress cough to calm panting, clear the lung and dissipate phlegm.Zhongfu (LU 1) combined with Feishu (BL 13) is the combination of Back-Shu and Front-Mu points, mainly for lung diseases such as cough, expectoration, and dyspnea. Moxibustion at Shenzhu (GV 12) can activate yang to promote qi-flow, regulate constitution, and improve physical function, so as to prevent and treat disease[18]. Pishu (BL 20) is the Back-Shu point of the spleen, which can invigorate spleen for benefiting qi.Zusanli (ST 36) is the He-Sea point of the Stomach Meridian and the Lower He-Sea point of stomach.Combined with Pishu (BL 20), it has the effect of regulating spleen and stomach function, promoting qi and blood transformation, and disease prevention and health care. Modern study has also suggested that acupuncture at Zusanli (ST 36) can improve the body's immune function[19]. Qihai (CV 6) is where body qi gathers, and treats qi-related diseases. These acupoints can reinforce lung-qi, harmonize the Ying-nutrient and Wei-defensive qi, invigorate the spleen and stomach,and strengthen constitution.
As an important part of TCM, pediatric massage is used to treat various diseases as it is safe and effective. It can not only reduce the toxic and side effects of drugs,but also avoid the pain of acupuncture. Therefore, it is welcomed by more and more children. Liu’s pediatric massage is one pediatric massage school in China.Wujing-concerted application is the characteristic of Liu’s pediatric massage, which is mainly based on the theory of five elements’ generation and restriction in TCM.According to the principles of the generation and restriction relationships among Wujing, the Wujingconcerted application for massage is formed. According to TCM syndrome differentiation and treatment, by Tuipushing Wujing to regulate the five Zang organs, it can harmonize yin and yang, treating both manifestations and root cause of disease[20-23]. Children with RRTI mainly are insufficient in the lung, spleen and kidney. Therefore,Tui-pushing Wujing is mainly based on reinforcing the spleen, lung and kidney. Qing-clearing Ganjing is to prevent excess liver qi over-restricting the spleen.Modern studies suggested that pediatric massage could improve the immunoglobulin (Ig) A and IgG levels, and enhance the immunity[24-25]. Also, massage could improve the serum CD3+and CD4+levels[26].
The results suggested that pediatric moxibustion plus Liu’s pediatric massage had combined the mild-warm stimulation, medication stimulation, meridians and acupoints together with the effects of manipulation,which could harmonize qi and blood, regulate Zang-fu organs, thereby enhancing the constitution of children with RRTI, reducing the incidence of respiratory tract infections. Moreover, it had positive significance for improving clinical symptoms in children with RRTI,indicating that the comprehensive therapy had a good clinical effect on RRTI. The treatment is safe and effective,easy to be accepted by children and their family, and thus is worthy of clinical promotion.
Conflict of Interest
There is no potential conflict of interest in this article.
Acknowledgments
This work was supported by the Inheritance Studio Construction Project for Academic School of Huxiang Fivemeridian Combined with Acupuncture-moxibustion and Tuina of the State Administration of Traditional Chinese Medicine (國(guó)家中醫(yī)藥管理局“湖湘五經(jīng)配伍針推學(xué)術(shù)流派”傳承工作室建設(shè)項(xiàng)目, No. LP0118041).
Statement of Informed Consent
Informed consent was obtained from the guardians of the recruited children in this study.
Received: 29 May 2020/Accepted: 19 November 2020
 Journal of Acupuncture and Tuina Science2021年5期
Journal of Acupuncture and Tuina Science2021年5期
- Journal of Acupuncture and Tuina Science的其它文章
- Study on the regulatory effect of herbal cakepartitioned moxibustion on colonic CD206, AMPK and TSC2 in rats with Crohn disease
- Acupuncture combined with medication for postherpetic neuralgia affecting the head and face:a randomized controlled trial
- Tendon-regulating and bone-setting manipulation plus endurance resistance exercises for female with chronic neck pain
- Efficacy and effect on related brain-gut peptides of acupoint sticking therapy for functional dyspepsia
- Effects of acupuncture plus language training on language function and cerebral blood flow in patients with motor aphasia after ischemic stroke
- Clinical efficacy observation of ‘Tong Du Yun Pi’manipulation for infantile diarrhea in autumn