Intervertebral bridging ossification after kyphoplasty in a Parkinson’s patient with Kummell’s disease:A case report
2022-01-24 09:24:50JieLiYunLiuLeiPengJianLiuZhiDongCaoMiaoHe
World Journal of Clinical Cases 2022年2期
INTRODUCTION
Kummell's disease is characterized by vertebral collapse,pseudarthrosis,and progressive pain caused by ischemic osteonecrosis of the vertebral body[1].Parkinson's disease (PD) is a pathological disorder associated with heterotopic ossification[2].However,there have been no reports of PD causing intervertebral bridge formation.Currently,kyphoplasty is an effective surgery for the treatment of Kummell's disease[3].However,occasional refracture of the vertebral body can seriously affect the prognosis of patients and is very difficult to treat[4].
In the present case,vertebral refracture and adjacent vertebral fracture after kyphoplasty resulted in persistent severe pain and dysfunction.These fractures were cured by extensive callus formation around the T12-L2 vertebrae,and intervertebral bridging ossification provided new stability.
CASE PRESENTATION
Chief complaints
A 78-year-old woman experienced severe low back recurrence pain 2 mo after kyphoplasty.
History of present illness
Two months before admission,the patient underwent kyphoplasty for Kummell's disease at L2,and the postoperative pain was significantly relieved.Two months after surgery,the patient experienced severe back pain recurrence in the same area.The radiographic findings indicated L2 refracture and new L1 fractures.
History of past illness
The patient had been suffering from PD of the rigidity type for more than 10 years.The stage of the patient was Hoehn and Yahr stage IV.She had been taking 600 mg levodopa and 150 mg benserazide hydrochloride orally daily to control the PD symptoms.The patient had significant standing instability when turning her body and could not maintain balance when her body was pushed.Functionally,the patient's mobility was significantly affected,and she could still walk and stand on her own,but she was unable to live independently.
Personal and family history
If you will only have patience I am just going out into the garden to gather some peas: we will shell them at our leisure, then I will light a fire and cook them, and when they are thoroughly35 done, we can enjoy them peaceably; there is no hurry
Physical examination
The patient's L1-2 spinous processes and pain on paravertebral muscle percussion were obvious,and lumbar movement was limited.No neurological injury was observed.
I am ... over Mamun now. Everytime I remember those days, looking at each other on the roof, talking, I feel really down. I wonder where he is now, if we will even meet again... I can never forget my first love.
Imaging examinations
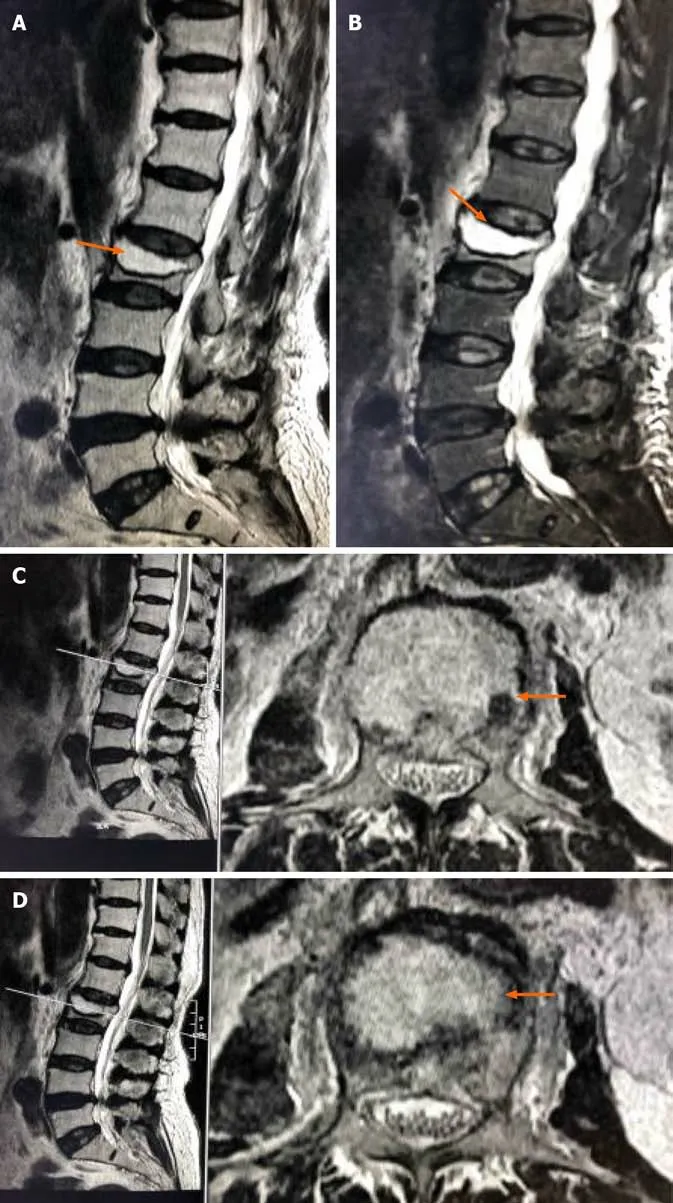
Preoperative magnetic resonance imaging (MRI) indicated collapse of the L2 MRI ertebral body and the formation of an intravertebral cavity-like structure indicated by the arrows (Figure 1A).T2WI with fat suppression (T2WI FS) showed a fluid-filled intravertebral vacuum,with little of the upper endplate structure remaining indicated by the arrows (Figure 1B).T2WI showed a low signal at the cavity edge,indicating vertebral bone necrosis and fibrous perichondrium formation,indicated by the arrows(Figure 1C and D).
The final diagnosis was Kummell's disease at L2,L2 vertebral refracture,and L1 vertebral compression fracture.
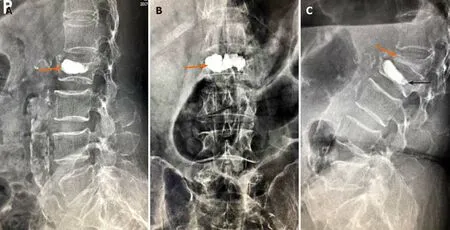
Postoperative X-ray images showed that bone cement filled the cystic cavity of the L2 vertebral body with smooth edges,and there was insufficient bone cement dispersion outside the cystic cavity (Figure 2A and B).Fifty days postoperatively,Xray images showed L2 vertebral body collapse,slight forward bone cement displacement (indicated by the black arrow),L1 vertebral compression fracture,and severe collapse (indicated by the orange arrow) (Figure 2C).
The patient's L1-2 spinous processes and pain on paravertebral muscle percussion were obvious,and lumbar movement was limited.No neurological injury was observed.
Physical examination
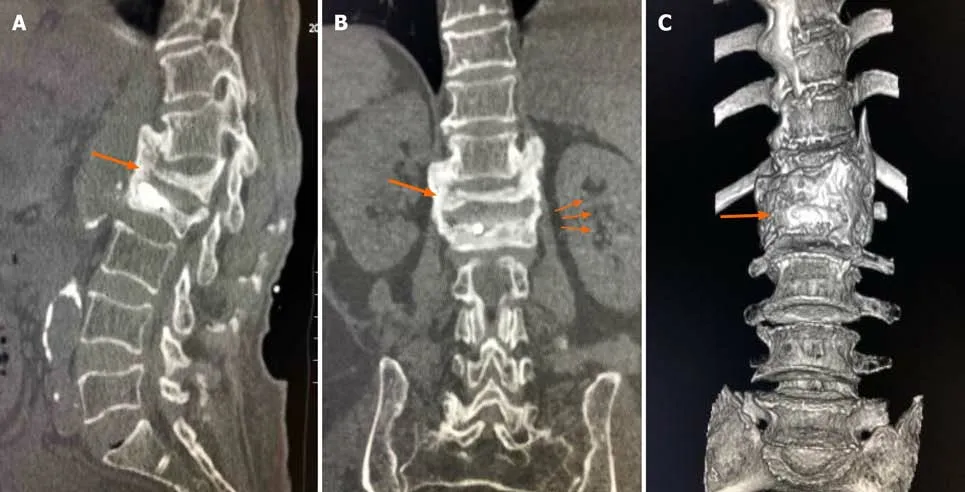
Seven-month follow-up CT indicated extensive callus formation around the T12-L2 vertebrae and intervertebral bridging ossification,providing new stability,as indicated by the arrow (Figure 3).
FINAL DIAGNOSIS
Then the Princess was compelled by her thirst to get down, and bending over the flowing water she cried and said: Oh! heaven, what am I to do? and the three drops of blood replied: If your mother only knew, Her heart would surely break in two
TREATMENT
The refracture of cemented vertebrae,displacement of bone cement and fracture of adjacent vertebrae are rare complications after percutaneous kyphoplasty for Kummell's disease and are relatively difficult to addres[5].PD is a pathological disorder associated with heterotopic ossification[6,7].There have been no reports in the literature on the occurrence or outcomes of postoperative complications in patients with both of these diseases at the same time.
Kyphoplasty was performed,and the severity of the intractable pain significantly decreased.Postoperative X-ray images showed that bone cement filled the cystic cavity of the L2 vertebral body with smooth edges,and there was insufficient bone cement dispersion outside the cystic cavity (Figure 2A and B).The patient’s VAS score for pain improved from 9 to 2.Fifty days postoperatively,the patient suddenly developed severe back pain,and the VAS pain score was 9 points.X-ray images showed L2 vertebral body collapse,slight forward bone cement displacement(Indicated by the black arrow),L1 vertebral compression fracture,and severe collapse(Indicated by the orange arrow) (Figure 2C).
The patient refused surgery,so she was given calcium acetate capsules (0.6 g po qd)and alfacalcidol (0.5 μg po qd),and bed rest and brace protection were ordered.
OUTCOME AND FOLLOW-UP
After conservative treatment for 2 mo,the patient's back pain was alleviated,and the VAS score improved from 9 to 2.CT at the 7-mo follow-up indicated extensive callus formation around the T12-L2 vertebrae and intervertebral bridging ossification,providing new stability,as indicated by the arrow (Figure 3).
DISCUSSION
Three months before admission,the patient developed lower back pain and discomfort and was hospitalized.The visual analog scale (VAS) score was 9 points.Preoperative MRI indicated collapse of the L2 vertebral body and the formation of an intravertebral cavity-like structure indicated by the arrows (Figure 1A).T2WI with fat suppression(T2WI FS) showed a fluid-filled intravertebral vacuum,with little of the upper endplate structure remaining indicated by the arrows (Figure 1B).T2WI showed a low signal at the cavity edge,indicating vertebral bone necrosis and fibrous perichondrium formation,indicated by the arrows (Figures 1C and D).
Cemented vertebral refracture
Mckiernan[8] reported that osteonecrosis and pseudarthrosis are the main risk factors for refracture.Due to the presence of fractures in the movable vertebrae,the bone cement tends to form a mass structure rather than spread throughout the trabecular bone[9].During polymethyl methacrylate (PMMA) injection,the bone cement follows the path of least resistance through the intravertebral space,resulting in insufficient filling and a lack of interlacing with nearby bone tissue[10].
After cementing the vertebral body,the protrusion of the endplate of the enhanced vertebral body increased as the height of the vertebral body was restored to a certain extent.At the same time,bone cement and residual endplates were fixed in the vertebral body adjacent to the endplate of the adjacent vertebral body.These factors lead to a lack of cushioning between adjacent vertebrae and bone cement,increasing the risk of refracture[14,15] (Figure 2C).
Adjacent vertebral body fracture
In addition,the formation of fibrous perichondrium at the internal edge of the vertebral cystic cavity prevented PMMA from forming an intersecting structure with the trabeculae[11] (Figure 1D).The stimulation of mechanical stress at the bone-cement interface may lead to microfractures of the vertebral body,highly progressive collapse of the vertebral body,failure at the bone-cement interface,and even fracture of the bone cement and collapse of the vertebral body[12].Therefore,Heo[13] proposed that vertebroplasty and kyphoplasty may be contraindicated by osteonecrosis or pseudoarthrosis of the fractured vertebral body.
According to Fahim DK[16],the normal intervertebral disc,the endplate and part of the trabecular bone of the treated vertebral body act as buffers between the bone cement and adjacent vertebral body.When bone cement reaches the level of the intervertebral disc,the tissue buffer decreases or completely disappears,leading to a high rate of adjacent fractures.Baroud[17] found that bulging of the enhanced endplate results in hardening of the intervertebral joint and the entire motion segment.A high intervertebral pressure and an inward-facing endplate bulge may be responsible for adjacent fractures[18,19].
The patient had no previous or family history of similar illnesses.
Intervertebral bridging ossification
Refractured vertebrae and adjacent fractured vertebrae are fused through intervertebral bridge formation at T12,L1 and L2 to achieve ultimate stability and significantly improve pain in patients within a short period (Figure 3).
PD has been described as a disease associated with HO incidence[6,7].Namazi proposed a pathway by which PD mediates heterotopic ossification development[20].In PD,peripheral blood mononuclear cells produce interleukin-1,interleukin-6,and tumor necrosis factor,which have been shown to play an important role in HO[21-24].In addition,levodopa mediates ectopic ossification,has been found to stimulate bone formation,callus formation,and healing through growth hormone (GH),and has been usedto promote bone growth after internal fixation of fractures[25-29].
Ali Baba and his son put a piece of gold into it, and Cogia Hassan, seeing that she was coming to him, pulled out his purse to make her a present, but while he was putting his hand into it Morgiana plunged40 the dagger into his heart
After looking at her he said, in a tone that might have struck terror into the boldest heart, though he did not seem to be angry: Good-evening, old man
The patient had PD for 10 years and was treated with oral levodopa and benserazide hydrochloride,so we hypothesized that the formation of her intervertebral bridge might be related to her disease and drug treatment.However,the existence of other interfering factors,such as the fracture itself,mechanical instability,blood leakage,and bone cement stimulation,which are all factors that stimulate the growth of fracture,cannot completely explain the formation of a large number of calli in a short period of time in patients with intervertebral bone bridges connecting three vertebrae[29].More case studies and further laboratory studies may be needed to confirm this phenomenon.
Then came yesterday. I heard a cry and a lot of things falling. The cry was from Harry and the things falling were a lot of dolls and other things which he had upset() while he was jumping over the counter. He ran across and grabbed12 a girl not ten feet from my window. She was small and dark and her eyebrows came to a little point in the middle.
The trunk, it is true, was cleft25 in themiddle from the root to the crown; the storms had bent it a little,but it still stood there, and out of every crevice26 and cleft, in whichwind and weather had carried mould, blades of grass and flowers sprang forth
CONCLUSION
Kyphoplasty is currently a common treatment for Kummell's disease,with definite short-term effects.However,complications still occur in the long term,and these complications are difficult to address;thus,the treatment needs to be selected carefully.To avoid refracture,an interlaced structure of bone cement with trabeculae should be created to the greatest extent possible during the injection of bone cement.Surgical intervention may not be urgently needed when a patient with PD experiences refracture and adjacent vertebral fracture,as a strong bridge may help stabilize the vertebrae and relieve pain.
 World Journal of Clinical Cases2022年2期
World Journal of Clinical Cases2022年2期
- World Journal of Clinical Cases的其它文章
- Successful management of delirium with dexmedetomidine in a patient with haloperidol-induced neuroleptic malignant syndrome:A case report
- Using a fretsaw in treating chronic penial incarceration:A case report
- Occupational fibrotic hypersensitivity pneumonia in a halogen dishes manufacturer:A case report
- Accelerated Infliximab Induction for Severe Lower Gastrointestinal Bleeding in a Young Patient with Crohn’s Disease:A Case Report
- Tension pneumocephalus following endoscopic resection of a mediastinal thoracic spinal tumor:A case report
- Primary adrenal diffuse large B-cell lymphoma with normal adrenal cortex function:A case report