Value of thyroglobulin combined with ultrasound-guided fine-needle aspiration cytology for diagnosis of lymph node metastasis of thyroid carcinoma
2022-01-24 09:24:34LiuYangZhangYongChenYaZhouAo
World Journal of Clinical Cases 2022年2期
INTRODUCTION
Common clinical diagnostic methods for cervical lymph node metastasis in thyroid carcinoma patients include ultrasound (US),computed tomography,magnetic resonance imaging,radionuclide scanning,and other imaging methods,as well as USguided fine-needle aspiration cytology (FNAC).However,all of these methods have limitations[1,2].US is the most commonly used imaging method;however,comorbid inflammatory lymphadenopathy can lead to misdiagnosis;accurate differentiation between benign and malignant nodules requires extensive experience[3].FNAC can offer further cytological diagnostic support for lymph nodes with suspicious US results.However,incorrect sampling sites,insufficient sample sizes,small metastases,and cystic alteration of the lesion can lead to false-negative results[4].Fine-needle aspiration of thyroglobulin (FNA-Tg) reportedly has a relatively high diagnostic value in lymph node metastasis and recurrence of differentiated thyroid carcinoma[5].In this study,we primarily aimed to explore and describe the value of FNA-Tg combined with US-guided FNAC to diagnose cervical lymph node metastasis in patients with thyroid carcinoma and explore factors influencing the diagnosis.
MATERIALS AND METHODS
Data
A total of 209 pathologically diagnosed thyroid carcinoma patients who visited the Thyroid Surgery Department of Affiliated Hospital of Chengde Medical University between Jan 2017 and Dec 2020 were selected.The inclusion criteria were as follows:(1) Patients who met the diagnostic criteria of thyroid cancer according to the National Comprehensive Cancer Network Guidelines for thyroid cancer criteria[6];(2) Patients with confirmed pathological diagnosis;(3) Patients aged 20 to 67 years;(4) Patients who presented with suspicious lymph node enlargement on preoperative cervical lymph node US and then underwent US-guided FNAC and FNA-Tg;and (5) Patients with complete data.The exclusion criteria were as follows:(1) Patients with a history of radiation and chemotherapy;and (2) Patients with lung infections and heart failure.
It had been a year since Susan, thirty-four, became blind. As the result of a medical accident she was sightless, suddenly thrown into a world of darkness, anger, frustration3 and self-pity. All she had to cling to was her husband Mark.
Before the implementation of this study,the research plan was submitted to the Medical Ethics Committee of our hospital for approval and then implemented after the decision and document of the Medical Ethics Committee.
Instrument check and FNAC method
For FNAC,the patients were placed supine with a soft pillow under their neck to fully expose the puncture site.After routine disinfection of the puncture site,1% lidocaine was applied under local anesthesia.A 22 G cell puncture needle (Yako,Japan) was selected,and the fine needle was inserted into the center of the lymph node under US guidance.The needle was rapidly retracted and inserted back and forth in different needle channels five times.Subsequently,the puncture needle was pulled out,the aspirated tissue was placed onto the slide,smeared,and fixed for pathological examination.Each lymph node was punctured at least three times.After HE staining,the smears were reviewed by two senior pathologists,and the cancer cells were either determined to be positive for lymph node metastases,or if no cancer cells were found,or if the number of cells was insufficient,the cells were determined to be negative.
FNA-Tg testing method
For FNA-Tg measurement,0.5 mL of 0.9% normal saline was absorbed with a 1-mL syringe,the needle was rinsed,and 1 mL of eluent was prepared.The supernatant was extracted after centrifugation at 3000 r/min for 5 min.Subsequently,the Tg content was detected using the COBAS E601 electrochemical analyzer (Roche,Basel,Switzerland) and an immunochemiluminescence method.
The judgment standards[7] were as follows:FNA-Tg>1.0 ng/mL was diagnosed as positive thyroid cancer lymph node metastasis,and FNA-Tg ≤ 1.0 ng/mL was diagnosed as negative thyroid cancer lymph node metastasis.
Statistical analyses
In this study,age and other measurement indexes were tested for normal distribution,and all were in line with approximate normal distribution or normal distribution,which was expressed by mean ± SD.A-test was performed using SPSS software (IBM Corp.,Armonk,NY,USA).The measured data were analyzed using antest.For multivariate analysis,a logistic regression model was used to draw the ROC curve and obtain the area under the curve (AUC).The test level was α=0.05.
Then he began to think that it was too absurd that he, the fascinating Featherhead, should fall in love with a portrait; and, to drive away the recollections of its haunting eyes, he rushed back to the town; but somehow everything seemed changed
RESULTS
Ultrasonographic findings of cervical lymph node metastases in positive and negative patients
Our study showed that patients with positive cervical lymph node metastasis had significantly higher rates of cortical centripetal thickening,hypoechogenicity of the cortex and medulla,long diameter/short diameter ratio<2,partial liquefaction or fusion of lymph nodes,abundant internal blood supply,and hilar absence than patients with negative lymph node metastasis (<0.05).These are the typical US characteristics of lymph node metastasis.The normal oval structure of the lymph nodes can be destroyed by the cancer cells;they have an irregular or round shape with a change in the vertical and horizontal diameter ratio.The internal structure can also be destroyed.In the case of lymph node metastasis,the lymphadenocortex involvement occurs first,leading to the loss of the cutaneous medulla structure.Moreover,the infiltration of cancer cells destroys the normal blood supply to the lymph nodes,and US usually reveals an uneven blood supply to the lymph nodes.

Comparison of FNA-Tg values in positive and negative patients with cervical lymph node metastasis
FNA-Tg values were significantly higher in patients with positive cervical lymph node metastasis than those with negative lymph node metastasis (<0.05) (Table 2).

Value of FNAC alone and FNA-Tg alone and their combination for the diagnosis of cervical lymph node metastasis in patients with thyroid carcinoma
Considering pathological results as the gold standard,a four-grid table was prepared(Table 3).The sensitivity and specificity of FNAC in the diagnosing cervical lymph node metastasis of thyroid carcinoma were 85.48% and 90.59%,respectively.The sensitivity and specificity of FNA-Tg for diagnosing cervical lymph node metastasis of thyroid carcinoma were 83.06% and 87.06%,respectively.The sensitivity and specificity of FNAC+FNA-Tg for diagnosing cervical lymph node metastasis of thyroid carcinoma were 96.77% and 91.76%,respectively (Table 4).


The Prince was deeply moved, and vowed37 that he would search the world for the Princess, and take no rest till he had found and restored her to her mother s arms
This time the King felt obliged to keep his promise, and calling his daughter to him, he said, My dear Grannonia, for that was the Princess s name, more as a joke than anything else, I demanded what seemed to me impossibilities from your bridegroom, but now that he has done all I required, I am bound to stick to my part of the bargain
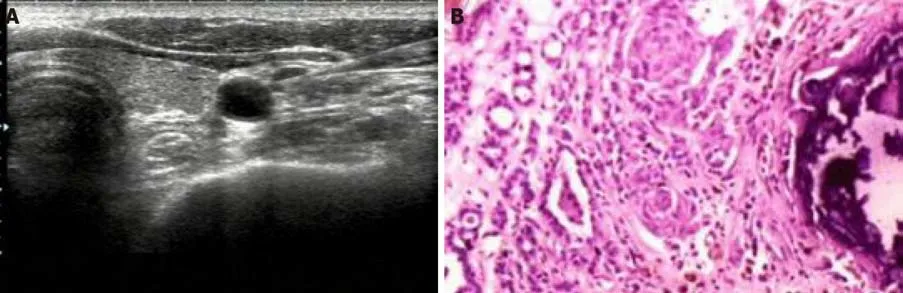
Figure 1 shows the results of US-guided FNA examination of cervical lymph nodes and postoperative pathological examination of lymph nodes in patients with papillary thyroid carcinoma with positive lymph node metastasis.
ROC curve analysis of FNAC and FNA-Tg alone and in combination for diagnosis of cervical lymph node metastasis in thyroid carcinoma patients
An ROC curve was drawn adopting the pathological results as the gold standard.Results showed that the AUC value for FNAC diagnosis of thyroid carcinoma with cervical lymph node metastasis was 0.880.The AUC value for FNA-Tg diagnosis of thyroid carcinoma with cervical lymph node metastasis was 0.851.The AUC value for FNAC+FNA-Tg for diagnosing thyroid carcinoma with cervical lymph node metastasis was 0.943 (Figure 2).

Univariate analysis of the influence of FNA-Tg alone on the diagnosis of cervical lymph node metastasis in patients with thyroid carcinoma
Patients were divided into groups based on FNA-Tg differential diagnosis.The univariate analysis showed that the differences between the two groups were statistically significant (<0.05),including the rate of long diameter,long diameter/short diameter lymph node ratio,the number of collected cells,serum thyroid stimulating hormone (TSH),serum Tg,and US characteristics (Table 5).
The Prince guessed easily that he had fallen on a witch s house, but as by this time it was quite dark and he could go no further, and as moreover he was not at all afraid, he stepped in
Multivariate analysis of the influence of FNA-Tg on the single diagnosis of cervical lymph node metastasis in patients with thyroid carcinoma
When the King heard that he had to thank him alone for the victory, he raised him higher than anyone else in rank, gave him great treasures and made him the first in the kingdom
The results of FNA-Tg differential diagnosis of cervical lymph node metastasis were adopted as dependent variables,and the statistically significant indexes,such as long diameter,long diameter/short diameter lymph node ratio,the number of collected cells,serum TSH,serum Tg,and characteristics of US signs,were adopted as independent variables to establish a logistic regression model.A long diameter/short diameter ratio<2,insufficient number of acquired cells,low level of serum Tg,and absence of typical US signs of lymph node metastasis were found to increase the risk of cervical lymph node metastasis in patients with thyroid carcinoma misdiagnosed using FNA-Tg (<0.05) (Table 6).


DISCUSSION
On US,patients with positive cervical lymph node metastasis showed significantly higher rates of cortical centripetal thickening,hypoechogenicity of the cortex and the medulla,long diameter/short diameter ratio<2,partial liquefaction or fusion of lymph nodes,abundant internal blood supply,and hilar absence than patients with negative lymph node metastasis (<0.05) (Table 1).
Tg is secreted by normal thyroid tissue and differentiated thyroid carcinoma and is a marker of tumor protein in peripheral blood[8,9].Tg expression is negligible in normal lymph nodes;d,it can be expressed in differentiated thyroid carcinoma,and lymph node metastasis and its concentration in tissue puncture fluid are much higher than that in serum[10].Detecting FNA-Tg levels in the eluent of needle biopsy samples can help reach the differential diagnosis of cervical lymph node metastasis in thyroid carcinoma.In this study,we adopted specific reference values for detecting positive
Affected by many factors,the positive threshold of FNA-Tg remains controversial[14,15].Although previous studies have reported that the diagnostic sensitivity of FNA-Tg was better than that of FNAC[16],our results showed no significant difference in sensitivity between the two methods.The small sample size in this study might have affected the sensitivity and specificity of the results.We found that the sensitivity and specificity of FNAC+FNA-Tg were superior for the diagnosis of cervical lymph node metastasis,thereby providing higher diagnostic accuracy.This may be because metastatic lymph nodes in thyroid carcinoma may be accompanied by significant cystic changes,which could be easily missed by FNAC examination alone.Lymph node eluting fluid has high Tg expression,which is of great help to the diagnosis.Cervical lymphoid node enlargement has many causes,and cytological examination alone is often insufficient for making a precise diagnosis.However,if combined with eluent FNA-Tg examination,the accuracy of diagnosis is improved.
Now go, he ended, and look after the pigs! So the next day she took out the pigs, and found them such good feeding grounds that they grew fatter every day
lymph node metastasis using FNA-Tg.The FNA-Tg value was significantly higher in patients with positive lymph node metastasis than patients with negative lymph node metastasis (<0.05).This suggests that because the thyroid tissue has a secretory function in the lymph node tissue,it may appear as lymph node metastasis due to the biological characteristics of the cell.Currently,FNAC is considered the most direct method to diagnose lymph node properties,as it can directly obtain the cells of the lesion and its tissue.However,its smear can be affected by factors such as blood,glia,and cell count,leading to a low sensitivity[10-12].When the lymph nodes are too small and the smear cells are insufficient,the sensitivity and specificity of FNAC diagnosis can be reduced,leading to an increase in false negatives,affecting the clinical diagnostic efficiency,and reducing the predictive accuracy[13].
In this study,a univariate analysis of the influence of FNA-Tg findings on the diagnosis of cervical lymph node metastasis revealed a significant difference between the two groups (<0.05) in terms of the rate of long diameter,the long diameter/short diameter ratio of the lymph nodes,the number of collected cells,serum TSH level,serum Tg level,and US characteristics.The multivariate analysis showed that a long diameter/short diameter ratio of<2,an insufficient amount of acquired cells,low level of serum Tg,and absence of typical US signs increased the risk of cervical lymph node metastasis in patients with thyroid carcinoma misdiagnosed by FNA-Tg (<0.05).
In conclusion,when diagnosing thyroid carcinoma patients with cervical lymph node metastasis,FNA-Tg can be affected by various factors,and its diagnostic value alone is not high;however,combined with FNAC,the sensitivity and specificity of diagnosis are significantly improved,providing a significant reference value to guide the treatment.
In this study,patients with suspicious cervical lymph node findings on US were studied.FNAC and FNA-Tg were performed to determine whether or not the diagnosis was thyroid lymph node metastatic carcinoma.Compared with previous studies[19,20],in our study,univariate and multivariate analyses of factors affecting FNA-Tg diagnosis were conducted for the first time,and the results were highly reliable.However,there were also some limitations to our study.The detection process and threshold setting lacked unified standards.Moreover,the factors affecting the test results were numerous and unclear.Thyroid inflammation,autoimmune diseases,and endocrine system diseases can all affect the serum Tg determination to some extent,especially in patients with false-positive and false-negative results.Therefore,underlying diseases should also be considered.
CONCLUSION
Some studies[17] have reported that the loss of thyroid tissue and inhibition of serum TSH after thyroidectomy may decrease serum Tg levels,and the levels of serum Tg can independently influence the diagnosis of FNA-Tg.Inhibition of serum TSH can reduce the serum Tg level,and a false negative FNA-Tg diagnosis is possible.In contrast,when serum Tg is not reduced,a false positive FNA-Tg diagnosis is possible[18].Therefore,it is suggested that FNA-Tg should be tested after TSH stimulation.The diagnostic performance of the FNA-Tg diagnostic threshold varies with thyroid status and serum Tg concentration,but there is no doubt that FNA-Tg detection as an auxiliary diagnostic method can bring about all of its unique advantages.
ARTICLE HIGHLIGHTS
Research background
Fine-needle aspiration cytology (FNAC) can offer further cytological diagnostic support for lymph nodes with suspicious ultrasound (US) results.
Research motivation
Fine-needle aspiration of thyroglobulin (FNA-Tg) reportedly has a relatively high diagnostic value in lymph node metastasis and recurrence of differentiated thyroid carcinoma.
Research objectives
We explore and describe the value of FNA-Tg combined with US-guided FNAC to diagnose cervical lymph node metastasis in patients with thyroid carcinoma.
Research methods
A total of 209 pathologically diagnosed thyroid carcinoma patients who visited the Thyroid Surgery Department of the Hospital were selected.
Research results
The sensitivity and specificity of US-guided FNAC,FNA-Tg,and US-guided FNAC+FNA-Tg were 85.48% and 90.59%,83.06% and 87.06%,and 96.77% and 91.76%,respectively.
Then she sat down to her work once more and span on, and as she did so an old saying which, she had often heard her godmother repeat whilst at work, came into her head, and she began to sing: Spindle, spindle, go and see, If my love will come to me
Research conclusions
Combined with US-guided FNAC,it is significantly improved.
Research perspectives
The detection process and threshold setting lacked unified standards.
 World Journal of Clinical Cases2022年2期
World Journal of Clinical Cases2022年2期
- World Journal of Clinical Cases的其它文章
- Successful management of delirium with dexmedetomidine in a patient with haloperidol-induced neuroleptic malignant syndrome:A case report
- Using a fretsaw in treating chronic penial incarceration:A case report
- Occupational fibrotic hypersensitivity pneumonia in a halogen dishes manufacturer:A case report
- Accelerated Infliximab Induction for Severe Lower Gastrointestinal Bleeding in a Young Patient with Crohn’s Disease:A Case Report
- Tension pneumocephalus following endoscopic resection of a mediastinal thoracic spinal tumor:A case report
- Primary adrenal diffuse large B-cell lymphoma with normal adrenal cortex function:A case report