
The status of caregiver burden and influencing factors among family caregivers in maintenance hemodialysis patients
2022-02-15 04:54:14FuHaiXiaGuoQingWangXueFenWang
Nursing Communications 2022年13期
Fu-Hai Xia,Guo-Qing Wang,Xue-Fen Wang*
1Health Science Center,Yangtze University,Jinzhou 434023,China. 2Nursing Department,Renmin Hospital of Wuhan University,Wuhan 430060,China.
Abstract Objective: To investigate the status of caregiver burden and influencing factors among family caregivers in maintenance hemodialysis (MHD) patients under the background of coronavirus disease 2019, and to provide references for nursing intervention. Methods:From May to August 2020, 237 convenient samples were recruited from the Hemodialysis Centers of The Renmin Hospital of Wuhan University and Zhongnan Hospital of Wuhan University. Questionnaires were conducted with the General Information Questionnaire,Zarit Burden Interview (ZBI), Sense of Coherence‐13 (SOC‐13) and Perceived Social Support Scale (PSSS). Multiple linear regression was used to analyze the influencing factors of caregiver burden. Results:The score of ZBI among the caregivers was(36.05± 14.09). The ZBI of family caregivers was negatively correlated with SOC‐13 and PSSS (P <0.01).Multiple regression results showed that professional status of MHD patients, activity of MHD patients, comprehensibility, manageability and other support were the main influencing factors of their caregiver burden (P <0.01), which explained 44.4% of the variance.Conclusion: The caregiver burden among family caregivers of MHD patients was above average under the background of COVID‐19, which indicated that they felt more burden in the process of caring. Medical staff could give targeted support and guidance in combination with their influencing factors to reduce their caregiver burden further.
Keywords: maintenance hemodialysis; family caregivers; caregiver burden; sense of coherence; social support
Introduction
Chronic kidney disease has become a serious public health problem facing the world [1], in which about 2% of patients progress to the end‐stage renal disease every year, with a growth rate much higher than that of China's population (1.1%) [2]. Maintenance hemodialysis(MHD) has been widely used in clinical practice as the main treatment for end‐stage renal disease. MHD patients are characterized by a long disease cycle, frequent and regular dialysis and many dialysis complications. It is reported that the number of patients receiving the MHD treatment in China has reached nearly 700,000 [1], and its care problem has gradually become the focus and hot spot of all sectors of society. Family caregivers refer to family members who are related to patients and undertake the main care tasks. They not only need to meet the needs of patients in daily life and medical rehabilitation, but also need to provide psychological and emotional support for patients[3]. Therefore, these family caregivers may experience significant levels of fatigue, stress, anxiety and depression related to both emotional disturbance and caregiver burden, which could, in turn,affect their lives and health [4, 5]. Especially during the prevention and control of coronavirus disease 2019 (COVID‐19), MHD patients generally have low immunity and need to travel to and from hospital frequently, which increases the risk of novel coronavirus infection for patients and their caregivers [6], which will undoubtedly increase the caregiver burden. The caregiver burden refers to a dynamic and multidimensional reaction that results from an imbalance of care demands and resources and induces overload in one or more of four components: physical, psychological, social, and financial issues [7].There is growing evidence that caring for a family member with end‐stage renal disease receiving MHD is one of the most burdensome experiences, as approximately 25% of caregivers self‐reported having depression, poor quality of life and low sleep quality [8, 9]. The sense of coherence, a psychological protection mechanism,can play a role in maintaining individual physical and mental health in various crises or adverse environments. The study has shown that sense of coherence can protect caregivers from high levels of psychological distress and caregiver burden [10]. The caregiver burden during the COVID‐19 pandemic is an important risk factor for depression in family caregivers, and providing psychological support is considered an important initiative to reduce the risk of depression in caregivers [11].In addition, the high level of social support also helps to reduce the caregiver burden. A Brazilian study found that caregivers reported lower levels of perceived social support compared with their care recipients, while caregivers who had more social support tended to provide more emotional support to their care recipients [12]. Studies on the caregiver burden among family caregivers in MHD patients during COVID‐19 have not been involved, and the status and influencing factors of the care burden have not been proved.Therefore, this study aims to investigate the status of care burden of family caregivers of MHD patients during COVID‐19 and analyze its influencing factors, in order to provide guidance for clinical targeted intervention and response to major outbreaks.
Methods
Ethical approval
All operations involving human volunteers were approved by the Renmin Hospital of Wuhan University ethics committee(2020YF0067), and the study followed the principles of Declaration of Helsinki.
Design and sample
This study was a descriptive cross‐sectional survey of family caregivers in MHD patients. From May to August 2020, we recruited participants from the Hemodialysis Centers of two hospitals in Wuhan,Hubei Province, China. Participants could have been considered if they matched the following criteria: (1) at least 18 years of age; (2)Those related to the MHD patient, have taken care of the patient for more than 1 month, and have undertaken most of the care tasks or spent the most time [6]; (3) clear awareness and effective communication; (4) informed consent and willingness to engage in the study. Participants may be excluded if they have (1) received payment, as for a nurse or babysitter; (2) an acute/critical illness involving the heart, brain, or lungs; (3) a history of mental illness. In this study, 245 questionnaires were gathered, of which 237 were valid, yielding an effective rate of 96.7%.
The sample size should be more than 10 times the number of covariate variables (These include comprehensibility, manageability,meaningfulness, friend support, other support and 13 general data variables with statistical difference) when using the multiple linear regression for analysis [13]. The final study identified 18 covariate variables. Given a 20% sample loss, the sample size should have been greater than 216, which means 237 samples match the criteria.
Measures
Demographic and clinical characteristics. We used a self‐made questionnaire to measure the demographic and clinical characteristics of participants. The contents of the questionnaire included: the gender, age, education, marital status etc. of MHD patients, and the gender, age, marital status, professional status, education etc. of family caregivers.
Zarit Caregiver Burden Interview (ZBI). The ZBI includes two subscales: personal burden and liability burden [14]. A five‐point Likert scale (0 = “no” to 4 = “always”) is used and the total score of 22 items varies from 0 to 88, with higher scores suggesting a higher level of care burden. The total score is divided into three levels: low(0 to 20), medium (21 to 39), and high (40 to 88). The instrument has been proven to be valid and reliable, and has been used among Chinese patients [15]. In this study, the Cronbach’s alpha coefficient was 0.880.
Sense of Coherence (SOC).The SOC includes three subscales:comprehensibility, manageability, and meaningfulness [16]. A five‐point Likert scale (1 = “often” to 7 = “never”) is used and the total score of 13 items varies from 13 to 91, with higher scores suggesting a higher level of Sense of Coherence. The instrument has been proven to be valid and reliable, and has been used among Chinese patients [17]. In this study, the Cronbach’s alpha coefficient was 0.763.
Perceived Social Support Scale (PSSS). The PSSS includes three subscales: family support, friends support and other support [18]. A five‐point Likert scale (1 = “Strongly disagree” to 7 = “Strongly agree”) is used and the total score of 12 items varies from 12 to 84,with higher scores suggesting a higher level of Social Support. The instrument has been proven to be valid and reliable, and has been used among Chinese patients [19]. In this study, the Cronbach’s alpha coefficient was 0.880.
Data collection procedure
The researchers collected questionnaires using an electronic questionnaire. We introduced the purpose, informed consent and filling methods of the study to participants, who completed the questionnaire independently or under the guidance of the researcher.If the answer time is less than 180 s or all the answers are consistent,the questionnaire is invalid. A total of 245 questionnaires were received, of which 237 were valid, with effective recovery of 96.7%.
Data analysis
SPSS version 26.0 (IBM Corporation, Armonk, New York, USA) were used to analyze data. Frequency and percentage were used to describe categorical variables. Mean and standard deviation (SD) were used to describe continuous variables. Two independent sample T‐tests or ANOVA were used to compare caregiver burden scores in MHD patients with different characteristics. Multiple linear regression was used to analyze the influencing factors of caregiver burden. All statistical tests were conducted by two‐sided tests, andPvalues of <0.05 indicated statistical significance.
Results
Caregiver burden, sense of coherence and social support scores
Table 1 shows the score of caregiver burden was(36.05±14.09), and the overall burden level was moderate. There were 44 cases with mild burden, 70 cases with moderate burden and 123 cases with severe burden.
Sample characteristics
Of the 237 MHD patients, the average age was 55.30 (SD =13.90;range from 18 to 76) years. Of the 237 family caregivers, 80 men and 157 women; 143 were married, 49 were unmarried, and 45 were divorced or widowed; 77 had no co‐caregivers and 160 had co‐caregivers (Number of family caregivers). More information about sample characteristics is reported in Table 2.
Comparison of caregiver burden scores among different characteristics
There was no statistical significance in caregiver burden scores among family caregivers of different gender, marital status, educational level and co‐caregivers (P >0.05), while other variables were statistically significant (Table 2).
Correlation of caregiver burden, sense of coherence, and social support among family caregivers
Table 3 shows that caregiver burden was negatively correlated with sense of coherence and social support, but the correlation for some subscales of these scales were not statistically different (P<0.05).
Multifactorial analysis of caregiver burden among family caregivers
In this study, the caregiver burden was taken as the dependent variable, and comprehensibility, manageability, meaningfulness,friend support, other support and 13 general data variables with statistical difference were taken as covariate variables, and then multiple linear regression analysis was conducted. Table 4 shows that covariate variables assignments.Table 5 shows that professional status of MHD patients, activity of MHD patient, comprehensibility,manageability and other support were the main influencing factors of their caregiver burden.
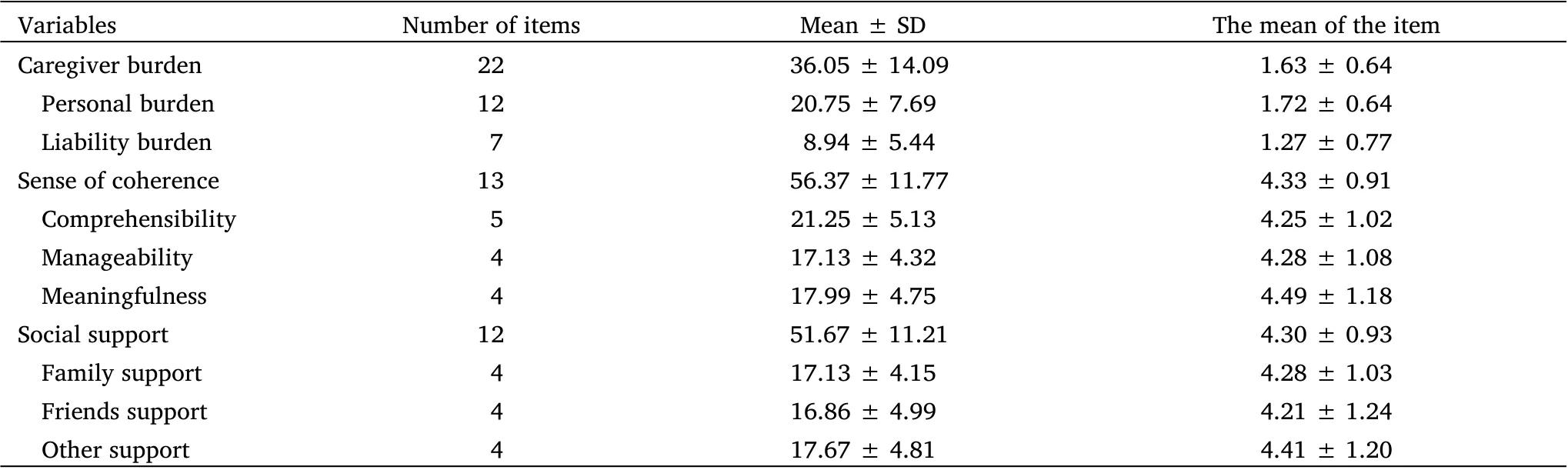
Table 1 Caregiver burden, sense of coherence and social support scores(N = 237)
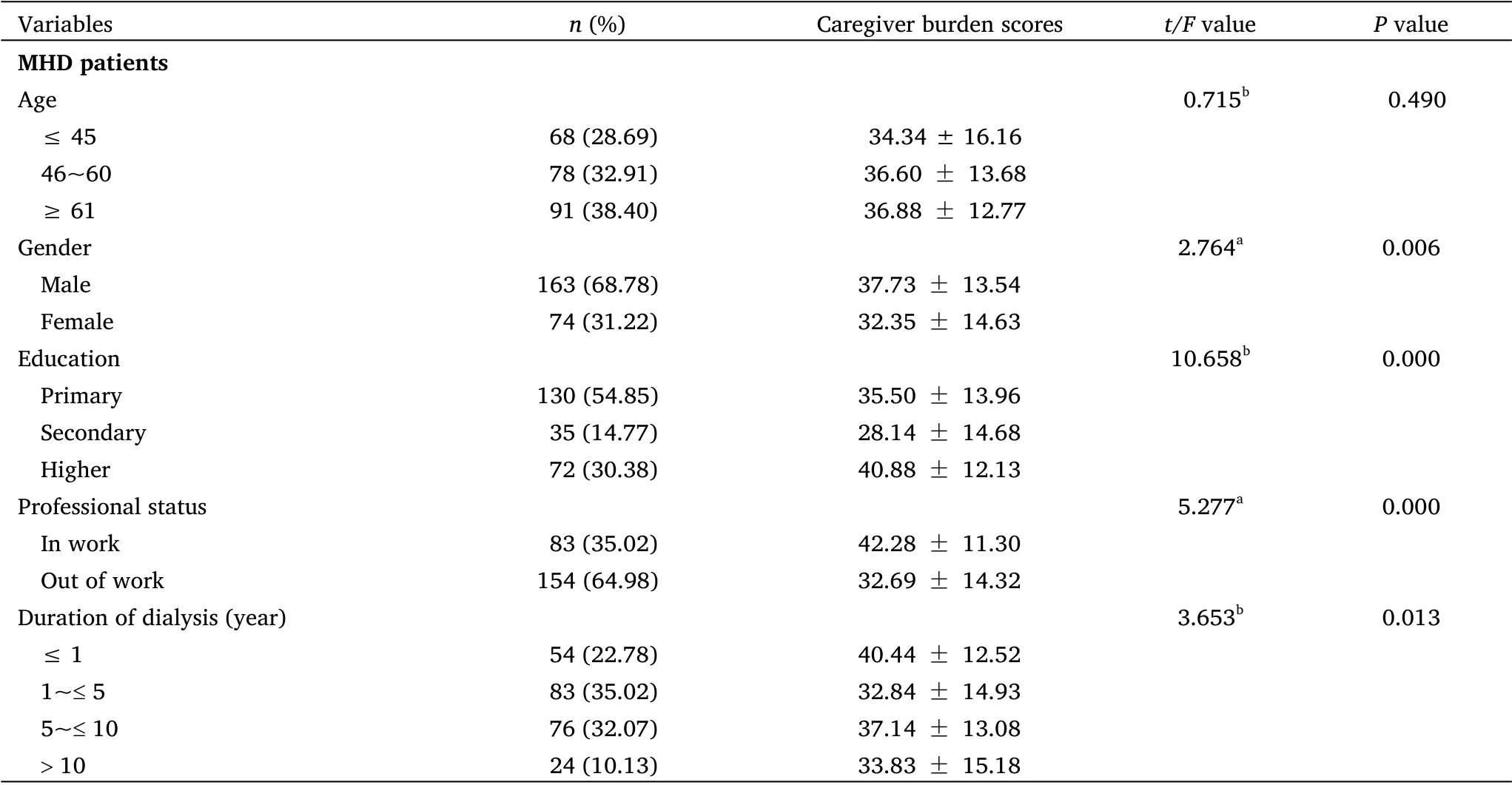
Table 2 Comparison of caregiver burden scores among different characteristics(N = 237)

Table 2 Comparison of caregiver burden scores among different characteristics (N = 237) (Continued)
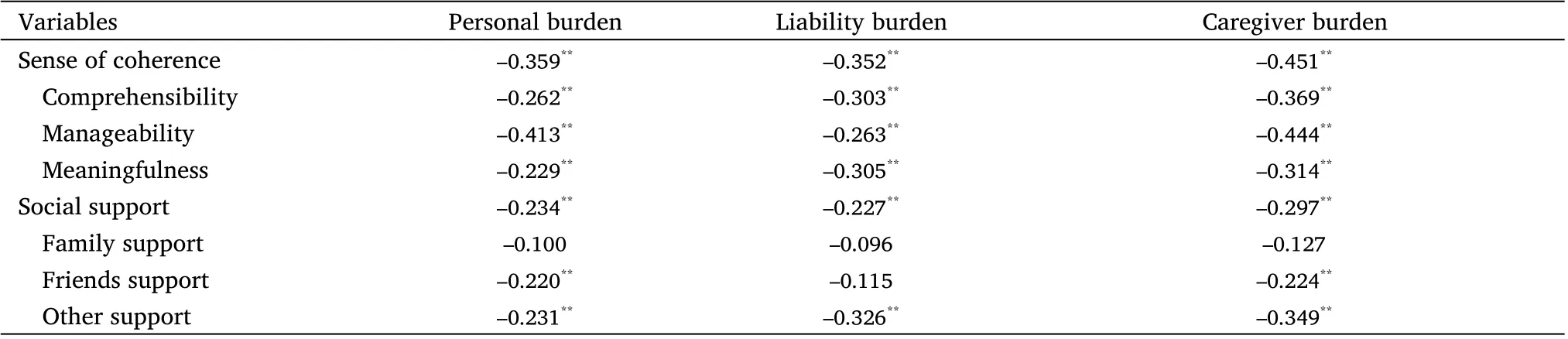
Table 3 Correlation of caregiver burden, sense of coherence, and social support among family caregivers (r)
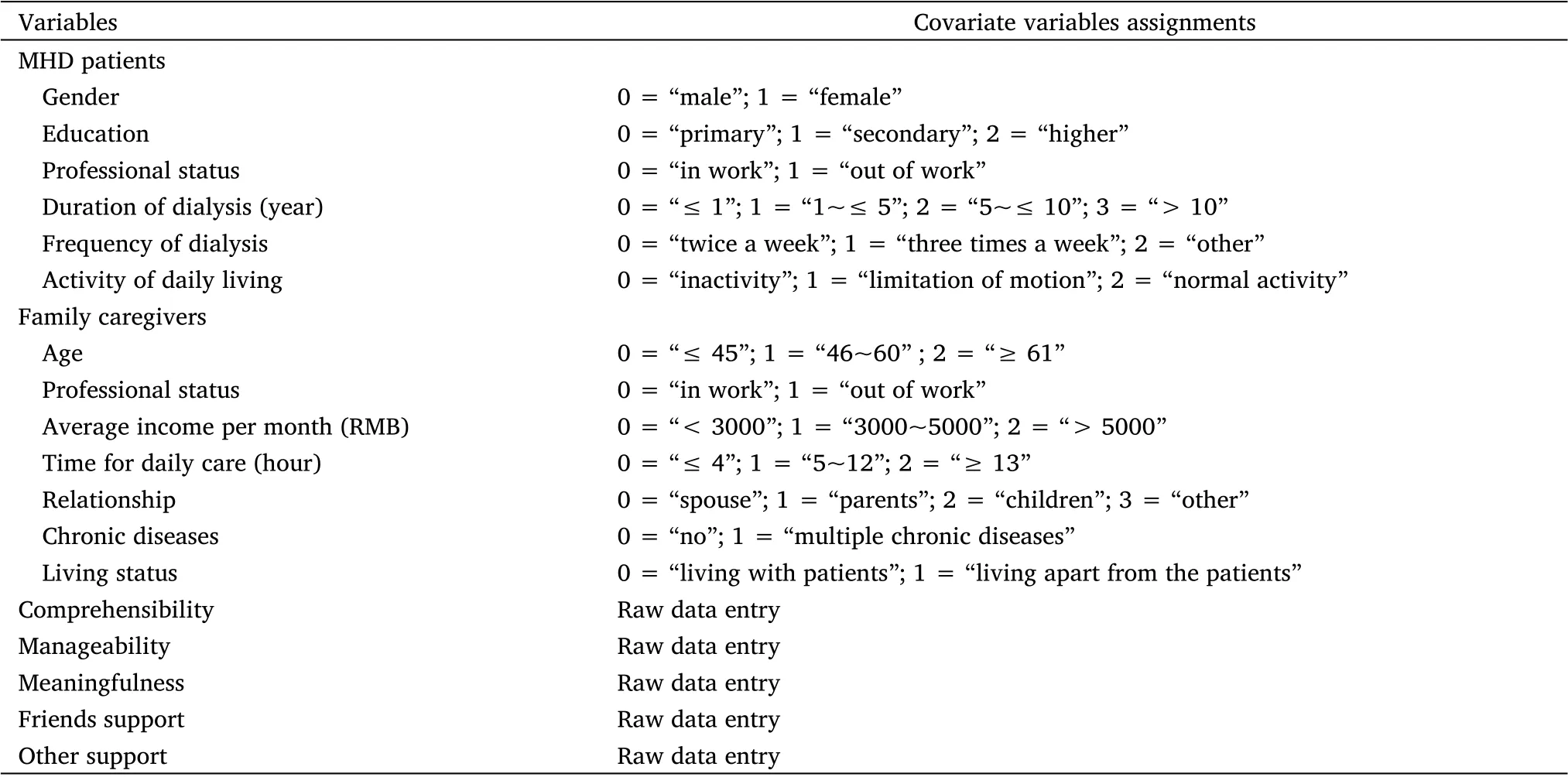
Table 4 Covariate variables assignments
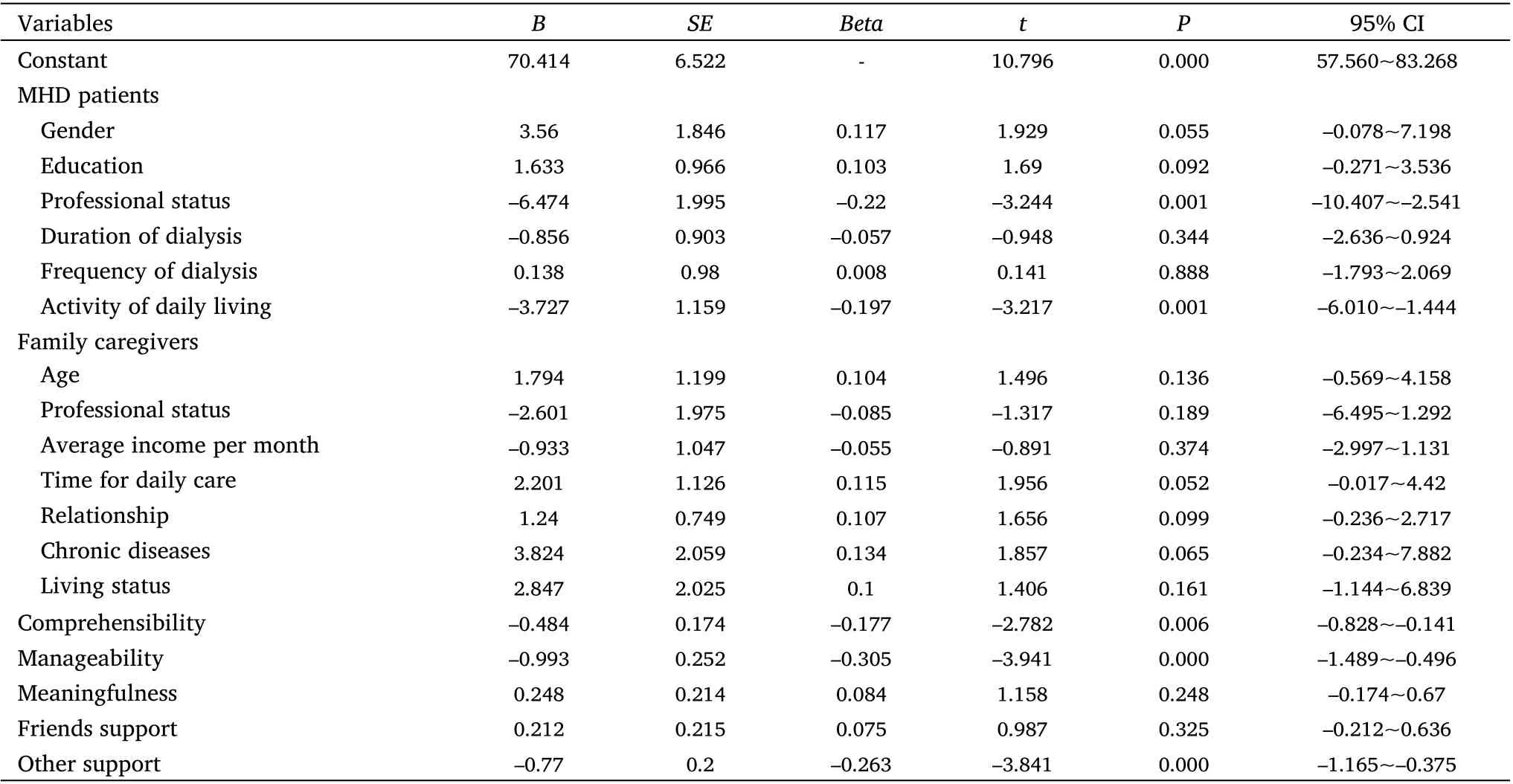
Table 5 Multifactorial analysis of caregiver burden among family caregivers (N = 237)
Discussion
The caregiver burden among family caregivers was found to be moderate in this study, which was higher than previous studies [20].The reasons may be as follows:First,MHD patients generally have low immunity and a high risk of novel coronavirus infection, which makes care for family caregivers more difficult, less able to cope and then increases the caregiver burden [6, 21]. Second, although novel coronavirus infection has been ruled out in some patients with fever,cough, lung inflammation and other symptoms during the COVID‐19 outbreak, these patients are required to be isolated in single rooms and sent to the buffer zone for continuous blood purification treatment [11, 22]. This undoubtedly increases the cost of health care and leads to the relative inadequacy of dialysis, which further increases the caregiver burden. Third, with the continuous improvement of the medical security system and zero addition of drugs and consumables, the National Health and Family Planning Commission of the People's Republic of China approved the establishment of an independent hemodialysis centers in 2016, which has greatly relieved the economic burden of dialysis patients and the shortage of dialysis resources. So that may be why the caregiver burden is moderate in this study. Studies showed that family caregivers had a decrease in both mental health and sleep quality during the lockdown [23]. In addition to the increased caregiving responsibilities, this result may be due to feelings of uncertainty about the future, fears related to contamination and decreased family support in the provision of care. These impacts have already been described as important psychosocial consequences of COVID‐19 for the general population [24]. It is suggested that medical staff should not only carry out routine health education for MHD patients and their caregivers, but also strengthen propaganda and education on COVID‐19 knowledge. On the other hand, medical staff should help them to obtain support resources from all sectors of society, such as community assistance to solve the problem of inconvenient transportation. The adequacy of dialysis for patients should be ensured as far as possible without additional medical costs.
The finding of this study showed that working MHD patients had a higher level of caregiver burden than non‐working MHD patients. The reason for this could be that working MHD patients are busy and have irregular eating patterns (high intake of convenience foods at meals).Too much social engagement or the influence of the surrounding living environment will increase the intake of phosphorus and easily cause hyperphosphatemia, thus increasing the caregiver burden [25].It is suggested that medical staff should educate family caregivers to strengthen the management of patients' treatment compliance and urge patients to consume food with low phosphorus content, so as to reduce the complications caused by hyperphosphatemia and reduce the caregiver burden.
The finding of this study showed that the activity of daily living of MHD patients was an influential factor for the caregiver burden of family caregivers, which was consistent with previous studies [26].The reason may be as follows: On the one hand, MHD patients with limitation of motion are more dependent on caregivers, which increases the care tasks and burden. On the other hand, patients with normal activity can go to hospitals for regular dialysis on their own or with community assistance, reducing the number of hospital visits by caregivers, which reduces their risk of contracting COVID‐19 and thus their caregiver burden.
The sense of coherence refers to the individual's overall feeling and cognition of life, which is a stable psychological tendency and psychological protection mechanism [10]. The finding of this study showed that the higher the comprehensibility and manageability, the lower the caregiver burden, which was consistent with previous studies [27]. The reason may be that family caregivers with high comprehensibility can better recognize various pressures and difficulties in the process of patient care. Family caregivers with high manageability can effectively use various support resources and explore their own potential resources to cope with the pressure, thus reducing their caregiver burden [28]. It is suggested that medical staff should pay attention to the sense of coherence of family caregivers,give corresponding psychological interventions, and improve their confidence in coping with pressure.
The finding of this study showed that the higher the level of other support in social support, the lower the caregiver burden. It is perhaps not surprising that family support and friend support were not significant predictors of caregiving burden in the present study. In the Chinese cultural context, caregivers are normally unwilling to bother other family members and close friends, tend to hide all of their difficulties without complaint to avoid giving “trouble to others” [29,30]. Sources of other support in this study could be caregivers'colleagues or leaders, community workers, medical staff, etc. The reasons may be as follows: First, 71.73% of caregivers took care of patients for more than 5 hours per day. For working caregivers, the support of leaders and colleagues was necessary for sufficient time to take care of patients. Second, community workers can help with transportation and medical care during COVID‐19, which can greatly reduce the burden and anxiety of caregivers. Third, dialysis quality control center established designated hospitals for treating MHD patients, and people from all walks of life gave more attention,support and help, which may be the reason why higher levels of other support can reduce the caregiver burden. It is suggested that medical administrators should reduce the caregiver burden by establishing a hospital‐family‐community integrated social support system [31, 32].
This study's main strength is that it is the first to explore the level of caregiver burden among family caregivers in MHD patients under COVID‐19. Our findings suggest that MHD patients' professional status, activity, comprehensibility, manageability and other support were the main factors affecting their caregiver burden. The limitation of this study is that the sample size is small due to the influence of COVID‐19, and only part of the influencing factors of caregiver burden were discussed. It is suggested to increase the sample size and carry out multi‐center studies in the future, so as to have a more comprehensive understanding of the caregiver burden among family caregivers under COVID‐19.
 Nursing Communications2022年13期
Nursing Communications2022年13期
- Nursing Communications的其它文章
- Nurses’ knowledge and skills concerning cardiopulmonary resuscitation: a descriptive study
- Surgical operation of a massive retroperitoneal tumor
- Progress in the application of Meleis transition theory in the nursing field
- Importance of teamwork communication in nursing practice
- From the perspective of traditional Chinese medicine nursing in the context of COVID-19
- Surgical first aid and nursing care of a parturient with massive hemorrhage in natural delivery