Tacrolimus treatment for relapsing-remitting chronic inflammatory demyelinating polyradiculoneuropathy:Two case reports
2022-03-15 11:59:54WenJiaZhuYuWeiDaHaiChenMinXuYanLuLiDiJianYingDuo
World Journal of Clinical Cases 2022年5期
lNTRODUCTlON
Chronic inflammatory demyelinating polyradiculoneuropathy(CIDP)is an immunemediated motor sensory neuropathy that is characterized by the demyelination of peripheral nerves and secondary axonal damage[1].and CIDP patients usually present with numbness and weakness of the extremities as well as a loss of reflexes[2].The exact pathogenesis of CIDP is not fully understood,but it involves an attack of the myelin sheath by components of both cellular and humoral immunity,ultimately leading to demyelination of nerve fibers[3].
There are several treatment options for CIDP including plasma exchange or the administration of corticosteroids(CS)and intravenous immunoglobulin(IVIg)[4,5].The failure of first-line treatment strategies to obtain satisfactory outcomes can lead to the consideration of immunosuppressive agents.Immunosuppressive agents include azathioprine,methotrexate,interferon alpha(IFN-α),cyclosporine(CyA),cyclophosphamide,mycophenolate mofetil,rituximab and stem cell transplantation[6-8].Accumulating evidence has demonstrated that CyA,a calcineurin inhibitor,can selectively inhibit cytokines produced by helper T cells with a quick onset of action[9-11].However,CyA has also been associated with side effects that may include nephrotoxicity[12].Tacrolimus,another calcineurin inhibitor,is more bioavailable with a faster onset of action and lower nephrotoxicity than CyA[13].Tacrolimus has been widely used in organ transplantation and for the treatment of autoimmune diseases[14].
In 1998,Ahlmén[15]reported the treatment of a patient with CIDP using a combination of glucocorticoids and tacrolimus.However,detailed information regarding the efficacy and safety of tacrolimus in CIDP remains unknown.In this study,the clinical response and follow up evaluation of two CIDP patients treated with tacrolimus were reported.
He soon arrived in the town where the mist-veiled queen reigned34 in her palace, but the whole city had changed, and he could scarcely find his way through the streets
CASE PRESENTATlON
Chief complaints
A 17-year-old female was hospitalized with recurrent episodes of numbness and weakness of limbs occurring over the previous 11 mo.
I own everything about me -- my body, including everything it does; my mind, including all my thoughts and ideas; my eyes, including the images of all they behold3; my feelings, whatever they might be -- anger, joy, frustration4, love, disappointment, excitement; my mouth and all the words that come out of it -- polite, sweet and rough, correct or incorrect; my voice, loud and soft; all my actions, whether they be to others or myself.
History of present illness
In December 2016,the patient presented with numbness in both hands,weakness in the upper extremities,difficulty combing her hair,and difficulty dressing.The patient’s symptoms presumably began after she suffered from a common cold.In April 2017,her weakness worsened,and the patient could no longer lift her upper extremities and had trouble sitting upright.The numbness in both hands gradually progressed toward the proximal extremities.Upon admission,the patient was diagnosed with CIDP at her local hospital,and she was administered methylprednisolone(1000 mg/d for 3 d)and IVIg(0.4/kg/d for 5 d;Table 1).Following treatment,her symptoms subsided and she was discharged with no follow-up treatment.In July 2017,the patient presented with another episode of finger numbness and extremity weakness.After three days,the patient could not walk,and she was admitted to her local hospital.The patient was treated with IVIg(0.4/kg/d for 5 d)and her condition improved.Then,in November 2017(11 mo after initial onset of symptoms),the patient presented with another CIDP episode and was admitted to our inpatient department one week after symptom onset.
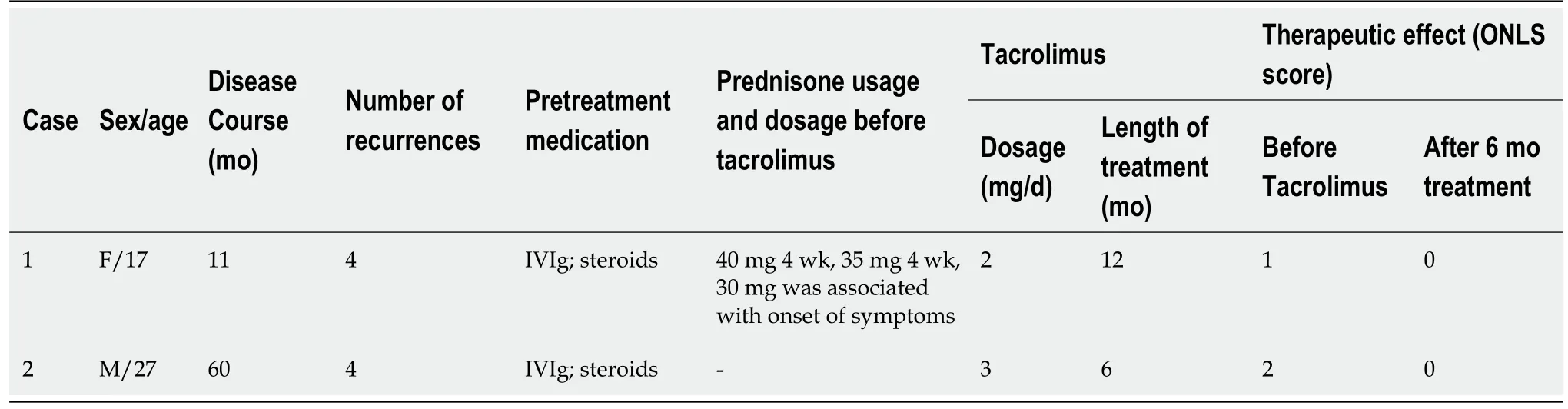
At the time of admission,both patients experienced CIDP symptoms that had recurred for the fourth time.The clinical features of case 1 were characterized by rapid progression after each recurrence.Following CS and IVIg treatment,her disability score improved by 4 points within five to seven days.However,the patient experienced weight gain following prednisone(40 mg/d)treatment and therefore she disliked the option of long-term CS use.Likewise,the second patient(case 2)developed obesity,diabetes,hypertension,and hyperlipidemia following long-term CS use.Their families could no longer afford the cost of IVIg and plasma exchange.Therefore,a quick-onset non-hormonal immunosuppressive agent was selected.
History of past illness
The patient used to be in a good health and had no previous medical history.
Personal and family history
The patient could not continue steroid pulse therapy or the expensive IVIg treatments.Therefore,oral tacrolimus(3 mg/d)was administered for six months,and his body weight was strictly controlled.
Physical examination
The patient showed proximal extremity muscle strength values of 2-3 out of 5,distal extremity strength values of 3-4 out of 5,and an absence of tendon reflexes.However,her superficial/deep sensation was normal.
The physical examination revealed obesity,an inability to walk on the toes,an inability to squat,a proximal/distal extremity muscle strength of 3 out of 5,and the absence of tendon reflexes as well as sensory anesthesia.
Laboratory examinations
The final diagnosis of both patients was relapsing-remitting CIDP.
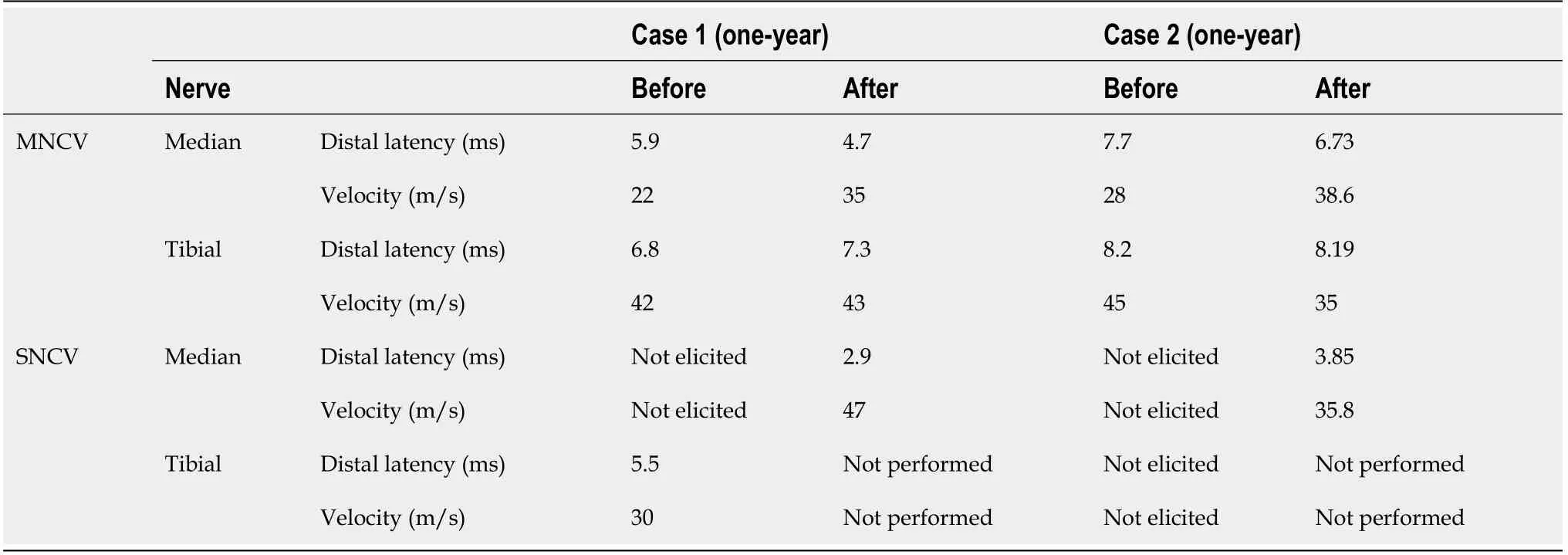
After two months,the patient's weight dropped to 83 kg,and the extremity weakness was markedly improved.His diabetes,hypertension,and hyperlipidemia were controlled with medication.Physical examination revealed symmetrical biceps muscle strength and a finger extension strength ratio of 4/5,a finger abduction/adduction muscle strength of 5/5,a hip flexion and toe dorsiflexion strength ratio of 4/5,muscle strength of 5/5 in the other extremities,and the absence of tendon reflexes.Prior to tacrolimus treatment,the ONLS scores were 2 points,which improved after six months of treatment(Table 1).During treatment,the serum concentration of tacrolimus fluctuated between 5.1 and 6.8 ng/μL.At the one-year follow-upappointment,the sensory and motor nerve conduction velocities had recovered but did not completely return to normal,supporting the suggestion that electrophysiological recovery is slower than clinical recovery(Table 2).
Imaging examinations
The brain and spinal MRI scan did not reveal any abnormalities.The chest and abdominal Computed tomography(CT)scans were normal.
The brain and spinal MRI scan did not reveal any abnormalities.The chest CT scan was normal.The abdominal CT scan showed fatty liver disease.
Sheesh! Give me a few points for self control! I snapped at my cranky() husband. I wanted to stop at a sporting goods store Going Out of Business sale we passed in the mall. There s nothing we need , his usual grumpy male comment. It s all overpriced junk. If they had anything good they wouldn t be going out of business.
A 27-year-old male was admitted to our department complaining of recurrent weakness and numbness in the limbs for 60 mo.
Thereupon the King travelled about for seven long years, and sought her in every cleft27 of the rocks and in every cave, but he found her not, and thought she had died of want. During the whole of this time he neither ate nor drank, but God supported him. At length he came into a great forest, and found therein the little house whose sign was, Here all dwell free. Then forth came the white maiden, took him by the hand, led him in, and said, Welcome, Lord King, and asked him from whence he came. He answered, Soon shall I have travelled about for the space of seven years, and I seek my wife and her child, but cannot find them. The angel offered him meat and drink,21 but he did not take anything, and only wished to rest a little. Then he lay down to sleep, and put a handkerchief over his face.
FlNAL DlAGNOSlS
Lumbar puncture was performed and the results showed an elevated protein level(59 mg/dL).Routine blood,urine,and stool examinations were normal.Thyroid function,infection,immune findings(ESR,anti-nuclear antibody spectrum,antineutrophil cytoplasmic antibody,and anti-cardiolipin antibodies)and tumor screening results were normal.Immunofixation electrophoresis and anti-ganglioside ester antibodies were absent.Nerve conduction velocities were recorded.
We sometimes reminisce on that concert of years ago when my teenage son and I made a lifetime memory. Aaron always laughs about the fact that his mom was the “only” person in the whole youth group to get an autograph from the performer.
TREATMENT
Case 1
Following admission,the patient’s weakness continued to progress and she was treated with IVIg(0.4/kg/d for 5 d)for the third time.Her extremity weakness and numbness quickly improved.However,her weakened left upper extremity and absence of right knee reflexes persisted.To prevent recurrence,oral prednisone(40 mg/d,reduced by 5 mg per month)was prescribed in November 2017.
Case 2
There were no negative personal habits or customs,and no special family history to note.
OUTCOME AND FOLLOW-UP
Case 1
In January 2018,the prednisone dose was reduced to 30 mg,but the patient had gained 12 kg(BMI of 26.67).Then,she developed bilateral fingertip numbness and weakness for the fourth time.Physical examination revealed bilateral digital opposition,an extensor strength of 4 out of 5,and extremity tendon reflex attenuation.Other physical examination findings were normal.The patient was treated with tacrolimus(2 mg/d)and prednisone(40 mg/d)was added to her treatment regimen.During treatment,the serum concentration of tacrolimus fluctuated between 1.6 and 2.9 ng/μL(Table 1).Following the initiation of treatment with tacrolimus,the numbness disappeared in the second week,and prednisone was reduced by 5 mg every two weeks.In April 2018,prednisone was decreased to 15 mg and then gradually reduced for discontinuation,but tacrolimus was maintained at 2 mg/d until the end of the 12-month treatment course(January 2019).Prior to treatment,the overall neuropathy limitation scale(ONLS)[9]score was 1 point and it improved to 0 points after six months of treatment(Table 1).In addition,nerve conduction studies were recorded before and after treatment(Table 2).At the one-year follow-up appointment in January 2019,the patient was asymptomatic and the sensory as well as motor nerve conduction velocities had recovered,but did not completely return to normal,suggesting that electrophysiological recovery can be slower than clinical recovery(Table 2).
Case 2
Lumbar puncture results showed an elevated protein level(82 mg/dL).Routine blood,urine,and stool examinations were normal.Thyroid function,infection,immune findings(ESR,anti-nuclear antibody spectrum,anti-neutrophil cytoplasmic antibody,and anti-cardiolipin antibodies)and tumor screening results were normal.Immunofixation electrophoresis and anti-ganglioside ester antibodies were absent.Nerve conduction velocities were recorded.
DlSCUSSlON
In this study,two patients were clinically diagnosed with relapsing-remitting CIDP characterized by extremity numbness and weakness,electrophysiological findings consistent with demyelinating peripheral neuropathy,and lumbar puncture findings indicative of cerebrospinal fluid protein-cell separation.Both patients were young and childless(17 and 27 years of age),and the disease courses were 11 and 60 mo in patients 1 and 2,respectively.All other related diseases were excluded.
The patient presented with gradually progressive numbness and weakness in his extremities and was diagnosed with relapsing-remitting CIDP in February 2014.The patient was treated with multiple courses of IVIg(0.4/kg/d for 5 d,= 12)and methylprednisolone(1000 mg/d for 3 d)therapy with subsequent dosage reductions.During the steroid treatment periods,the patient’s weight increased from 70 kg to 103 kg[body mass index(BMI)of 30.86]and he developed secondary diabetes,hypertension,and hyperlipidemia.In October 2018,he again developed weakness in his extremities that gradually worsened.
Ahlmén[15]used tacrolimus(also known as FK506)in 1998 to treat a 28-yearold woman with relapsing-remitting CIDP.In that particular patient,high-dose IVIg,cyclophosphamide,and azathioprine were ineffective.She had a favorable outcome with high-dose prednisone but she relapsed after discontinuation of the prednisone.Reduction therapy involving a combination of plasma exchange and a high dose of prednisone(80 mg/d)was effective,but the patient developed steroid myopathy.Therefore,she was administered a high dose of tacrolimus(0.42 mg/BMI/d)that was later reduced to 0.08 mg/BMI/d after 1.5 years,and prednisone(40 mg/d)was discontinued after the first six months.This treatment course had a favorable outcome,and the patient did not relapse within the one year of observation.Nevertheless,that patient developed side effects including diarrhea and hand tremors during the highdose tacrolimus treatment course,but those symptoms disappeared when the tacrolimus dose was reduced[15].
The combination of tacrolimus and FK506 binding protein(FKBP)forms the FK506-FKBP-12 complex,which can prevent T cell proliferation,decrease T-cell mediated tissue damage,and play an immunosuppressive role through the inhibition of various lymphocyte products,such as IL-2[16].Tacrolimus has been widely used in organ transplantation and may be an effective treatment strategy for CIDP patients.However,several organ transplant patients using tacrolimus developed reversible demyelinating peripheral neuropathy[17-19].Nevertheless,those symptoms were observed in only 3% of organ transplant patients,and may be attributed to the high doses of tacrolimus that were administered(5-10 mg/d)[20].
This request roused her to fury, since she had counted upon the Princess s fine robes to clothe her for the rest of her life, so that it was some time before the Prince could make himself heard to explain that he was willing to pay for them
21. Changed them into swans: Animal transformation and shapeshifting is a common motif in folklore and found in almost every culture around the world, often attributed to witches and other magical beings, but sometimes practiced by humans. The change can either be voluntary or imposed through enchantment, as it is here. Shapeshifting is often instigated by the rising or setting of the sun or moon. The most common types of shapeshifting for humans usually involves changing into a bear or wolf, especially for men. In tales of the AT 451: The Maiden Who Seeks Her Brothers classification, the brothers are usually turned into a type of bird, including ravens, ducks, and swans.Return to place in story.
In this study,both patients were young adults and childless.Due to possible reproductive toxicity,cyclophosphamide and azathioprine were not optimal treatment options in these younger patients[21,22].Therefore,the patients preferred treatment with tacrolimus due to its relatively mild side effects and quick onset of action.Among the nonhormonal immunosuppressive agents,tacrolimus has the fastest onset of action[11,13].In this study,case 2 used a single dose of tacrolimus(3 mg/d)for six months,and the severity of extremity weakness was significantly improved.On the other hand,case 1 used a slightly lower dose of tacrolimus(2 mg/d)for 12 mo.In case 1,although the serum concentration of tacrolimus was lower(fluctuating from 1.6 to 2.9 ng/μL),we were still able to reduce the concentration of prednisone and prevent side effects attributed to prolonged CS treatment.However,this suggests that the serum concentration of tacrolimus is not the only factor that determines the efficacy of treatment,but this point will be addressed in future studies.
CONCLUSlON
In conclusion,these results demonstrate the efficacy and safety of low-dose tacrolimus in the treatment of CIDP if first-line treatment options were ineffective or contraindicated.Nevertheless,future multi-center studies that enroll a greater number of patients will be necessary to fully evaluate the role of tacrolimus in the treatment of CIDP.
ACKNOWLEDGEMENTS
Thanks due to the two young patients’ support and the trust in our hospital.
 World Journal of Clinical Cases2022年5期
World Journal of Clinical Cases2022年5期
- World Journal of Clinical Cases的其它文章
- Subclavian artery stenting via ilateral radial artery access:Four case reports
- Neurothekeoma located in the hallux and axilla:Two case reports
- Diffuse invasive signet ring cell carcinoma in total colorectum caused by ulcerative colitis:A case report and review of literature
- Aseptic abscess in the abdominal wall accompanied by monoclonal gammopathy simulating the local recurrence of rectal cancer:A case report
- Unusual magnetic resonance imaging findings of brain and leptomeningeal metastasis in lung adenocarcinoma:A case report
- Vedolizumab-associated diffuse interstitial lung disease in patients with ulcerative colitis:A case report