Prostate sclerosing adenopathy: A clinicopathological and immunohistochemical study of twelve patients
2022-06-27 08:34:48RunLinFengYanPingTaoZhiYongTanShiFuHaiFengWang
World Journal of Clinical Cases 2022年18期
lNTRODUCTlON
Sclerosing adenopathy of the prostate is a rare pseudomalignant proliferative lesion with a distinct histomorphological and immunohistochemical phenotype that often resembles acinar adenocarcinoma but may also resemble sarcomatoid carcinoma[1]. It can manifest as single or multiple lesions, in which good small glands and scattered single-cell components can be seen, forming the impression of cell-like features. These lesions are benign pseudotumor hyperplasia lesions that are very similar to those of small alveolar prostate adenocarcinoma and are often misdiagnosed as prostate cancer by primary pathologists due to their characteristic interstitial spindle cell proliferation and small glandular architecture. They are observed in 2% of the transurethral prostatectomy or prostatectomy specimens and are rare in small samples derived from prostate needle biopsy[2-4]. The glandular components show nuclear atypia, including nuclear enlargement and prominent nucleoli. However, sclerosing adenopathy tends to be a more focal lesion than sarcomatoid carcinoma, which is thought to arise from the myoepithelial cells surrounding the prostate, high molecular weight cytokeratins. Moreover, the lesions are often positive for muscle-specific actin staining. Compared with that prostate adenocarcinoma, sclerosing adenopathy has a lower incidence and a higher misdiagnosis rate. Furthermore, since it is a rare lesion, to date, no large samples have been available for clinical pathology experiments. In clinical treatment, surgical resection is still the best treatment option for sclerosing adenopathy of the prostate. To further understand this condition, we aimed to investigate the histopathological morphology and immunohistochemical phenotype of this very rare prostate lesion and to further explore its associated biological significance and underlying mechanisms.
MATERlALS AND METHODS
Thirteen patients with prostate sclerosing adenopathy that visited the Second Affiliated Hospital of Kunming Medical University from January 2015 to November 2021 were enrolled and followed up.Their clinical history, imaging data, and disease were analyzed and further confirmedthe relevant immunohistochemical analysis. Twelve specimens were routinely fixed using 4% neutral formaldehyde,paraffin-embedded, and tissue-sectioned to a thickness of 4 μm, followed by HE staining and immunohistochemical analysis. The HE-stained slides were reviewed by three pathologists to confirm the diagnosis. We reviewed the gross specimen characteristics and read the immunohistochemical product instructions, the expiration dates of the antibodies, the localization of the positive antibodies, and the staining intensity interpretation criteria in detail. The required immunohistochemistry AR, CKH, P63,CD56, CK5/6, calponin, S100, P504S, prostate-specific antigen (PSA), PSAP, P53, and Ki-67 markers were obtained from the Fujian Meixin Company, China, and the procedures were carried out strictly according to the instructions, and positive and negative controls were routinely set up.
裝備在車內(nèi)的嵌入式系統(tǒng)可以安全、便捷地將人們送到目的地,裝備在玩具飛機(jī)中的嵌入式系統(tǒng),可以使傳統(tǒng)無線電控制的玩具飛機(jī)達(dá)到新的高度,引入嵌入式系統(tǒng)的GPS技術(shù)可以讓戶外運(yùn)動(dòng)者隨心所欲欣賞沿途風(fēng)光,而不用擔(dān)心迷路,這些都要?dú)w功于嵌入式系統(tǒng)的發(fā)展。
Prostatic sclerosing adenopathy is highly misdiagnosed as prostate adenocarcinoma or other tumor-like lesions. Therefore, it should attract the attention of clinicopathologic researchers.
None of the 12 patients in this study had received prior radiotherapy, chemotherapy, immunotherapy, or drug therapy. Complete clinical and pathological data were obtained for all 12 patients, and intraoperative histological specimens were obtained. The study was approved by the Ethics Committee of the Second Affiliated Hospital of Kunming Medical University (approval number: trial-PJ-2021-142).Since the study was performed using medical records and biological specimens obtained from previous clinical consultations, all conditions were met to exempt patients from informed consent.
1)Constraints on NP:if something such as articles and novels etc uoods,its meaning is realized or known.
In addition, there are no studies that show that the PSA value is related to the occurrence and development of prostate sclerosing adenopathy. In this study, the PSA value of the vast majority of patients with sclerosing adenopathy was within the reference range. Therefore, patients with sclerosing adenopathy should be informed that long-term follow-up and observation are required. If the PSA value increases significantly compared to the original value, and clinical symptoms such as frequent urination, urgency, dysuria, hematuria, and dysuria appear, patients should promptly consult their doctor, since they may have prostate cancer.
RESULTS
Clinical data
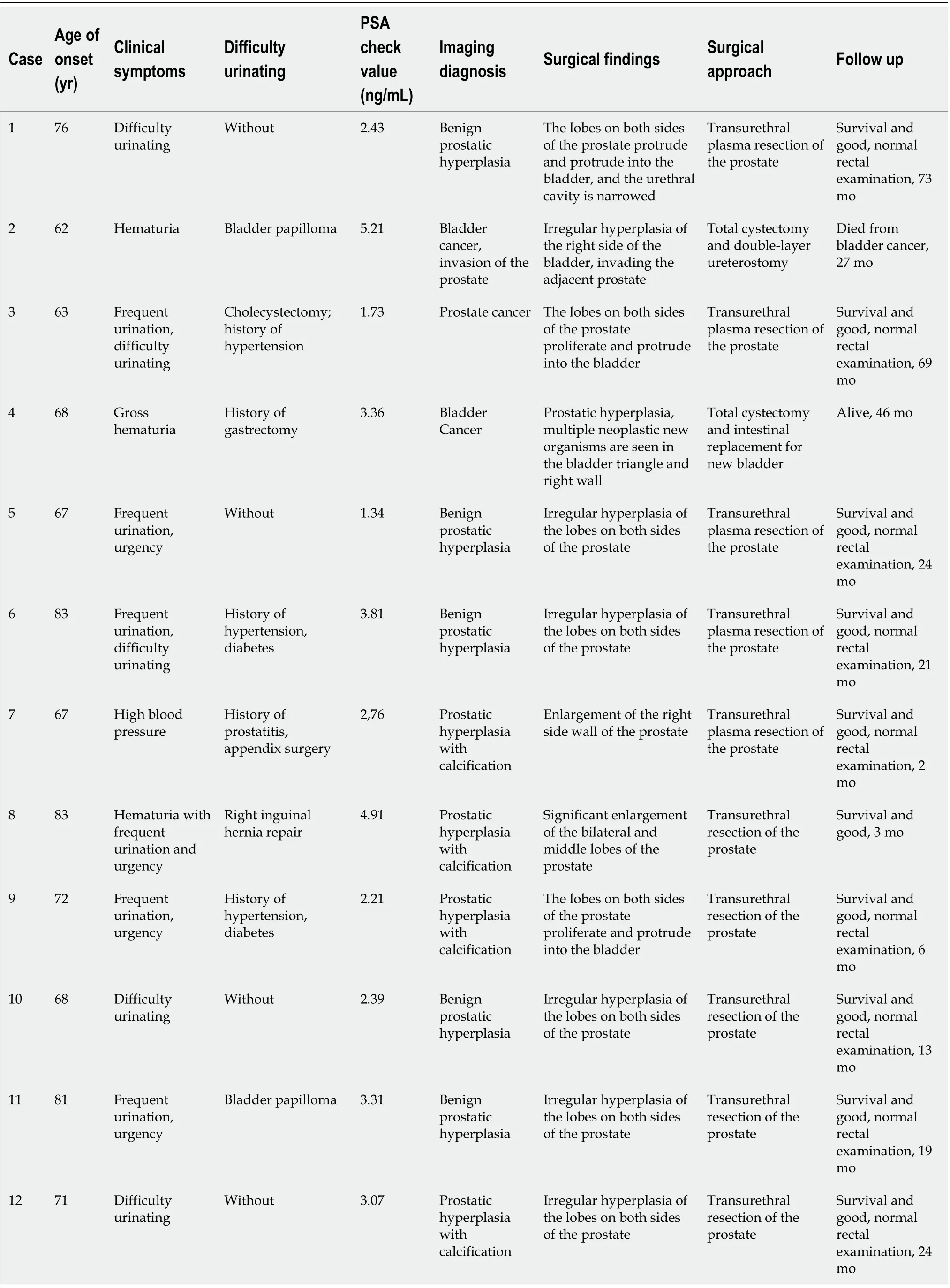
A total of 7674 surgically resected prostate specimens were collected between January 2015 and November 2021, including 625 radical prostatectomy specimens, 1155 prostate puncture specimens, and 5894 transurethral electrodesiccation prostate specimens. A re-read of the 7674 prostate specimens revealed 12 cases of sclerosing adenopathy (0.2%), 2 of which were found in radical prostatectomy specimens, and 10 were found in transurethral resection specimens, with no lesions found in the prostate puncture specimens. The clinical data, laboratory tests, pathological morphology, and immunohistochemical phenotype of these 12 cases of prostatic sclerosing adenopathy were analyzed and are summarized in Table 1.
All 12 patients were elderly men with an average age of 71.7 years (age range, 62-83 years). In terms of clinical symptoms, 11 patients presented varying degrees of hematuria, urinary frequency, urinary urgency, and difficulty in urination, and one patient had increased blood pressure. After admission to the hospital, the laboratory tests revealed that 11 of the 12 patients had serum total prostate-specific antigen (PSA) values within the normal reference range, and only one patient had a slightly higher than normal value. Rectal finger examination showed hyperplastic changes in all the prostate tissues, with varying degrees of prostatic hyperplasia visible intraoperatively, mainly in both lobes and on the right wall. Among the 12 cases, transurethral resection of the prostate was performed in 10 of them, and total cystectomy and bowel replacement with total cystectomy and double ureterostomy for bladder cancer was performed in two cases, respectively.
Imaging features
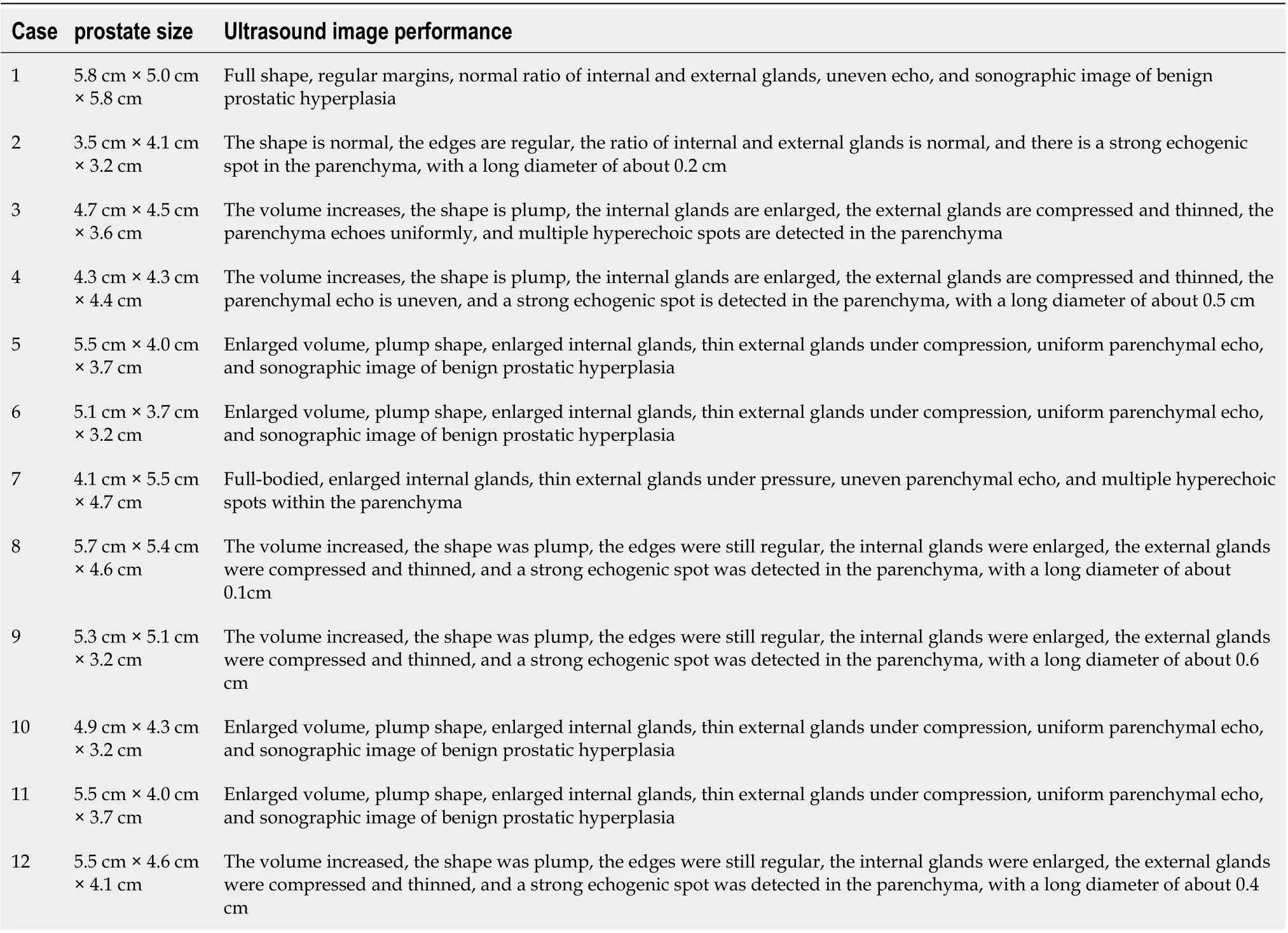
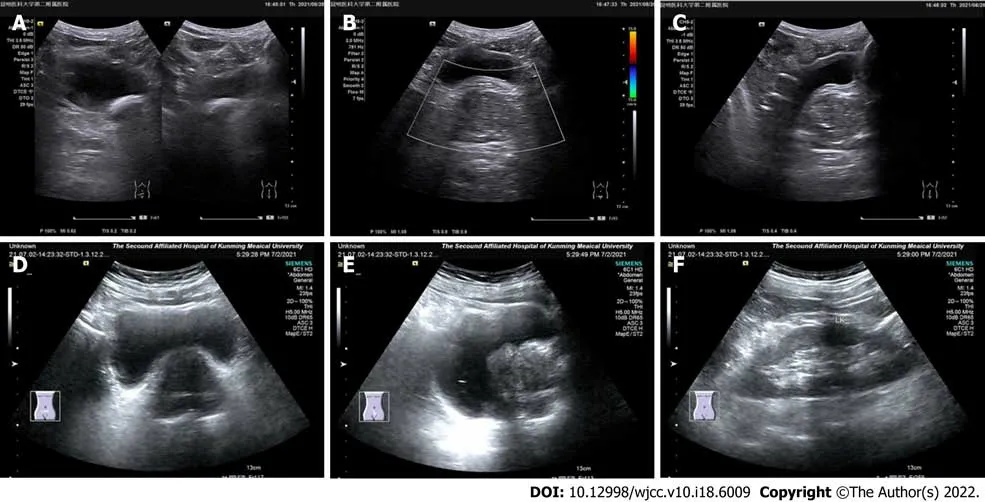
In the 12 patients, the computed tomography examination results showed an enlarged prostate with single to multiple calcified foci and, in three cases, localized protrusion into the bladder trigone with uneven enhancement (Figure 1). The preoperative ultrasonography results showed an enlarged prostate morphology, an enlarged inner gland, a thinning of the outer gland under pressure, and inhomogeneous parenchyma with one to multiple strong echogenic spots in all the 12 patients (Figure 2,Table 2).
共和縣處于藏區(qū),人們的飲食習(xí)慣主要是面食、青稞炒面以及肉類為主,對于蔬菜的需求量不是太大。2017年,共和縣蔬菜產(chǎn)量分布如下:
Histopathological findings
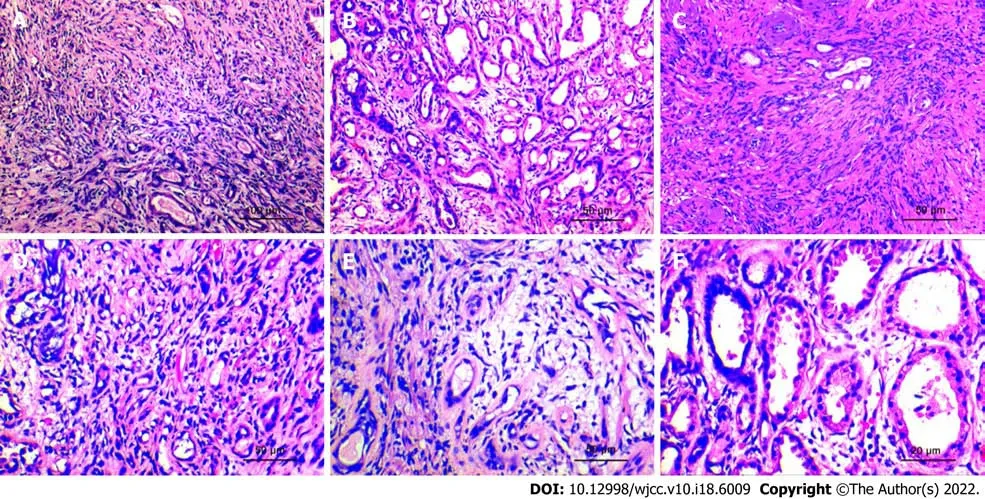
Specimen analysis showed that 10 cases presented a fragmented prostate tissue, two cases presented the complete cystoprostate tissue, which was grayish-red, along with a tissue multi-sectional cut that was tough. No obvious nodules or masses were seen. The microscopic observation results revealed that all 12 cases of prostate sclerosing adenopathy presented modularly distributed lesions indicative of benign prostatic hyperplasia. The lesions only had a few millimeters, had a nodular shape with varying degrees of small alveolar hyperplasia, without an obvious envelope, and with a growth pattern that mimicked the infiltration pattern of "prostate adenocarcinoma" (Figure 3A). The hyperplastic mesenchyme extruded the gland into ductal (Figure 3B), lacunar, and linear (Figure 3C) forms, and the glandular epithelium was covered with eosinophilic spike-like cells. Some of the glands were extruded to form vacuoles, and the increased number of vacuolated cells could form a structure similar to that of printed ring cells (Figure 3D). The interstitium was collagenous or mucinous and consisted of cells with a mildspindle-like morphology (Figure 3E). Observation at high magnification showed an eosinophilic cytoplasm with nuclei located at the base and small nucleoli but no nuclear division (Figure 3F).
媽媽印象最深刻的就是吃紅薯,她告訴我,早上吃的是“整豬整羊”,意思是光吃蒸紅薯,中午是“芝麻拌糖”,意思是在飯上蒸一點(diǎn)紅薯,晚上則是“吹吹打打”,吃的是煨紅薯,需要拍灰吹打……

Immunohistochemical phenotype
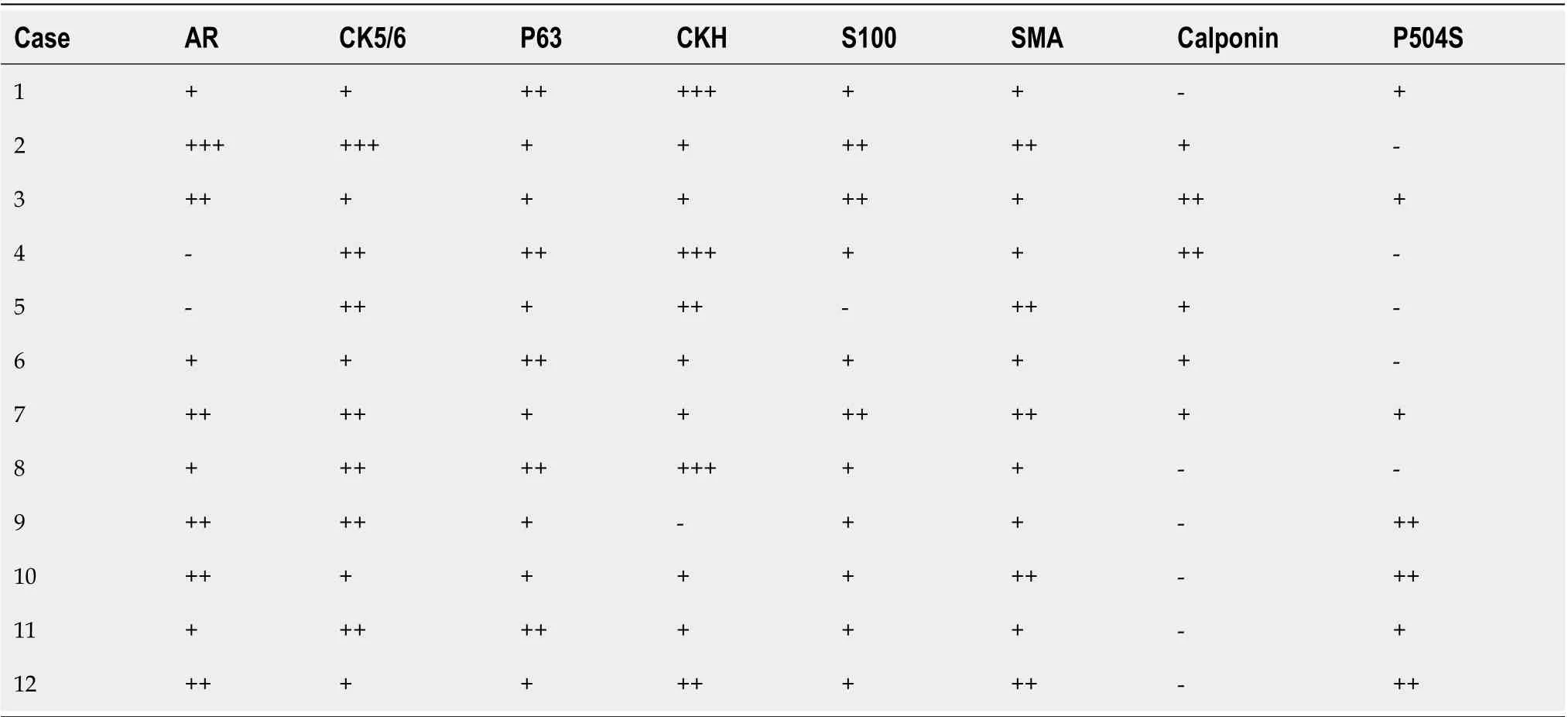
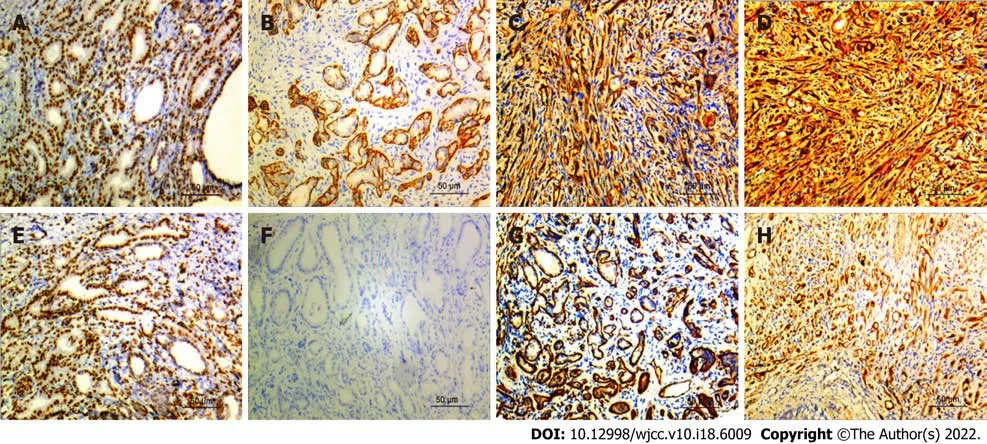
The basal cells of all the 12 cases of prostatic sclerosing adenopathy expressed molecules such as AR(Figure 4A), CKH (Figure 4D), P63 (Figure 4E), and CK5/6 (Figure 4C) to varying degrees, and also myoepithelial markers such as calponin (Figure 4B), S100 (Figure 4H), and smooth muscle actin (SMA)(Figure 4G). Nine of the 12 cases did not express P504S (Figure 4F), and the remaining three cases showed only a weakly positive expression of P504S. In addition, the prostate-specific markers PSA and PSAP were also expressed, P53 was not expressed, and the Ki67 proliferation index was in the 1%-3%range (Table 3).
Follow-up results
The mean follow-up time was 27.6 mo (3-73 mo), and 11 of the 12 patients survived well with normal rectal examinations and no recurrence or exacerbation of the disease. One patient died 26 mo after surgery due to bladder cancer.
DlSCUSSlON
Patients should be informed that long-term follow-up and observation are required. If the PSA value increases significantly compared to the original value, and clinical symptoms such as frequent urination,urgency, dysuria, hematuria, and dysuria appear, patients should promptly see their doctor, since they may have prostate cancer.
Sclerosing adenopathy is a rare benign proliferative lesion of the small alveoli without a markedly sclerotic stroma that occurs most occasionally after transurethral resection of the prostate, simple prostatectomy, or radical prostatectomy based on benign prostatic hyperplasia. It is detected by pathologists but occurs very rarely[17,18]. The histopathological pattern of sclerosing lymphadenopathy of the prostate is very similar to that of mammary sclerosing lymphadenopathy; however, unlike mammary sclerosing lymphadenopathy, prostatic sclerosing lymphadenopathy results in small lesions,usually with only a few millimeters[19]. It can result in single or multiple lesions, and it mostly occurs in the peripheral area of the prostate. It is difficult to detect the lesionrectal ultrasound, and it cannot be toucheddigital rectal examination. In addition, the serum PSA value is not high; thus, it is very difficult to measure it in clinical practice. In this group of 12 cases of prostate sclerosing lymphadenopathy, ultrasonography and rectal examination showed no abnormalities, and the serum PSA value did not increase. With the continuous improvement of ultrasound-guided technology, the probability of finding prostate sclerosing lymphadenopathy in biopsy tissue samples will increase; however, the possibility of it being misdiagnosed as prostate cancer will also increase. Research analysis found that 2% of the cases with this condition were diagnosed as prostate cancer. T1a stage prostate cancer wasconfirmed to be prostate sclerosing adenopathyreexamination[20]. Therefore, surgeon pathologists should consider prostate biopsy specimens as of great importance to avoid overdiagnosis of sclerosing adenopathy as prostate cancer.
Sclerosing adenopathy of the prostate has clear demarcation, is associated with small and concentrated lesions, nodular growth, no obvious capsule, and an infiltrative growth trend to the surrounding normal prostate tissue, similar to the growth pattern of prostate adenocarcinoma, but in the scope of growth-restricted lesions[21]. On the surface, it has a worrying appearance, with morphological distortions that can form stripes, threads, clusters, nests, and even single-cell arrangements. When the gland overproliferates, it may expand into a cyst, in which the amyloid material disappears and is replaced by a crystalline or myxoid material that is suggestive of prostate cancer[9,12]. In addition,several authors have described the lesion as presenting mild atypia and even small nucleoli, but generally no apparent large nucleoli. When individual cases are accompanied by moderate heterogeneity, heterogeneity, such as large and deep nuclear staining and prominent nucleoli, they are likely misdiagnosed as prostate adenocarcinoma. There is no evidence of the underlying malignancy of this lesion, although follow-up in our cases and others documented in the literature is admittedly limited.
碳酸鎳沉淀分離濃密池采用砼襯橡膠,再襯耐酸耐溫陶磚的復(fù)合襯里結(jié)構(gòu),橡膠內(nèi)襯為5 mm厚預(yù)硫化丁基橡膠(P- ⅡR- 18),呋喃樹脂膠泥砌筑2層耐酸耐溫陶磚(200 mm×200 mm×54 mm)。除鐵、除鈷帕丘卡空氣攪拌槽嘗試采用了新方法砼襯橡膠,再襯耐酸耐溫陶磚的復(fù)合襯里結(jié)構(gòu)[3];導(dǎo)流筒為乙烯基樹脂玻璃鋼制作;導(dǎo)流筒支架為TA2材質(zhì);槽蓋為鋼件內(nèi)外表面襯膠。
In conclusion, sclerosing adenopathy of the prostate is a morphological abnormality with characteristic histological features and immunohistochemical profiles. All the available evidence indicates that it is a benign condition that does not require treatment and is not a precancerous condition of prostate cancer.It is important to note, however, that many of the cases encountered to date have had a short follow-up period, and that it may often co-exist with other unrelated cancers in older men. The pathogenesis of this lesion is unclear, but its most striking feature seems to be the ability of cells to differentiate and proliferate. Studying and better understanding the features of sclerosing adenopathy should lead to its appropriate conservative management.
Sclerosing adenopathy of the prostate is considered a rare variant of adenopathy whose biological behavior remains uncertain, and the research on the risk of prostate cancer following a diagnosis of sclerosing adenopathy is very limited. Sclerosing adenopathy might be one of the precursors of prostate adenocarcinoma; however, this is unlikely because of its rarity and lack of other evidence linking its clinic features or pathology to cancer. When patients with sclerosing adenopathy present with cellular atypia, it is considered atypical sclerosing adenopathy; however, we should emphasize the use of the term "atypical sclerosing adenopathy" does not imply that these lesions are precancerous. Some scholars have found that DNA aneuploidy occurs in some atypical sclerosing adenopathy cases, but all typical sclerosing adenopathy cases are DNA diploid[28]. Whether sclerosing adenopathy can be used as an independent feature to predict the risk of prostate cancer in men is not yet clear, and a large multiinstitutional prospective study is needed for confirmation.
Sclerosing adenopathy has a similar histological pattern to that of the following lesions and is easily misdiagnosed as one of them. In this group of 12 patients with sclerosing adenopathy, two were misdiagnosed as having prostate adenocarcinoma and one was misdiagnosed as having nephrogenic adenoma by the primary pathologist. Therefore, prostate adenocarcinoma sclerosing adenopathy should be distinguished from the following lesions[1]. Prostate adenocarcinoma, which is the most likely misdiagnose. The identification points include: (1) Sclerosing adenopathy is mainly located in the peripheral area, with small and concentrated lesions, unlike cancer, that spreads and whose growth is invasive; (2) Sclerosing adenopathy is glandular hyperplasia with interstitial hyperplasia that is mucoid or fibrous; (3) An eosinophilic basement membrane material is seen around the ducts of patients with sclerosing adenopathy; (4) Mild-to-moderate dysplasia of the glandular epithelium may lead to subnucleation without significantly enlarged nucleoli; (5) There is no amyloid but a myxoid in the glandular follicular lumen. Furthermore, prostate cancer acini are lined with a layer of cuboidal or columnar cells without a distinctly flattened basal cell layer, as evidenced by the negative immunoreactivity for keratin 903[29,30]; and (6) Nephrogenic adenomas differentiate from sclerosing adenomas when they are tubular or solid. Nephrogenic adenomas are usually confined to the lamina propria, covering a single layer of short columnar or subcubical epithelial cells, among which some are shoe-stud-like cells, with round or oval nuclei, visible nucleoli, and most express markers such as CK7, CKH, CKL, and CEA,whereas they do not express the markers P63, PSA, PSAP, GATA3, and CK5/6. Atypical adenomatous hyperplasia is also nodular hyperplasia with clear borders; however, the lesions are often interspersed with a small number of large acinar with a normal structure in the proliferating small glands[31].
沿河地區(qū)民居建筑平面形式豐富,正房面闊三間、五間或七間,有相當(dāng)多采用帶檐廊和甩袖的平面形式,部分民居以窯洞為正房;廂房多采用三開間不帶甩袖的平面;臨時(shí)性或附屬建筑多為兩開間平面。山區(qū)民居院內(nèi)建筑等級差別不大,多為不帶甩袖的三開間平面。多開間及帶甩袖民居建筑平面的產(chǎn)生與當(dāng)?shù)夭煌H共同生活的居住模式息息相關(guān)。以五開間南北向建筑為例,“長輩一般住東邊三間,中間會有一個(gè)小廳,晚輩住西邊兩間(圖10)。”1)甩袖的做法可以增加室內(nèi)空間,前后墻一般都會砌筑小土炕,兩炕之間用土灶或火爐聯(lián)系,或者可將土灶砌筑在室外檐廊盡端。
CONCLUSlON
In daily clinical practice, immunohistochemical markers are relied upon to help determine when lesions are morphologically atypical or when cellular heterogeneity occurs. Moreover, prostate basal cells are not considered myoepithelial cells[22], contrary to the notion of the myoepithelial origin of salivary gland myoepithelial cells, since they do not have actin filaments. S100 protein and smooth muscle actin are not expressed in normal prostate basal cells[23,24]; in contrast, the presence of the S100 protein and SMA immunoreactivity in basal cells of sclerosing adenopathy suggests that they present myoepithelial differentiation, a characteristic feature based on which sclerosing adenopathy is diagnosed. In addition, some scholars have confirmed the existence of microfilaments in the cytoplasm of basal cells of sclerosing adenopathy using electron microscopy, which is consistent with the presence of actin filaments[25]. In rare cases, S100 protein immunoreactivity can be seen in prostate basal cell hyperplasias, such as adenoid basal cell carcinoma, adenoid cystic carcinoma, and atypical basal cell hyperplasia[26]. In addition, we have recently found that D2-40 is a sensitive marker of prostate basal cells[27]; therefore, D2-40 and the combination of P63 and cytokeratin can be used to differentiate sclerosing adenopathy from prostate cancer. However, in practice, due to the severe extrusion of basal cells and myoepithelial cells, the immunohistochemical expression results are not ideal, and some sclerosing adenopathy cases will express P504S to varying degrees, overlapping with the immunohistochemistry results of patients with prostate cancer, posing great challenges during pathological diagnosis.
Sclerosing adenopathy of the prostate is a morphological abnormality with characteristic histological features and immunohistochemical profiles. All the available evidence indicates that it is a benign condition that does not require treatment and is not a precancerous condition of prostate cancer. It is important to note, however, that many of the cases encountered to date have had a short follow-up period, and that it may often co-exist with other unrelated cancers in older men. The pathogenesis of this lesion is unclear, but its most striking feature seems to be the ability of cells to differentiate and proliferate. Studying and better understanding the features of sclerosing adenopathy should lead to its appropriate conservative management.
ARTlCLE HlGHLlGHTS

Research motivation
Sclerosing adenopathy of the prostate is a morphological abnormality with characteristic histological features and immunohistochemical profiles. All the available evidence indicates that it is a benign condition that does not require treatment and is not a precancerous condition of prostate cancer. It is important to note, however, that many of the cases encountered to date have had a short follow-up period, and that it may often co-exist with other unrelated cancers in older men. The pathogenesis of this lesion is unclear, but its most striking feature seems to be the ability of cells to differentiate and proliferate. Studying and better understanding the features of sclerosing adenopathy should lead to its appropriate conservative management.
Research objectives
This study explores the clinicopathological features, diagnosis, and immunohistochemical phenotypes that distinguish prostate sclerosing adenopathy from other conditions. We believe that our study makes a significant contribution to the literature because we show that this condition is benign, does not require treatment, and is not a precancerous condition of prostate cancer. However, notably, many of the cases encountered to date have had a short follow-up period, and this condition may often co-exist with other unrelated cancers in older men.
Research methods
The clinical data, laboratory tests, pathological morphology, and immunohistochemical phenotypes of 12 cases of prostatic sclerosing adenopathy were retrospectively analyzed, and the relevant literature was reviewed.
Research results
The authors summarized the age, clinical symptoms, medical history, serum total prostate-specific antigen (PSA) value, surgical findings, surgical methods, follow-up time, and follow-up results of 12 patients with prostate sclerosing adenopathy in detail (Table 1). The results of the study showed that the patients were all elderly men, with an average age of 71.7 years. The patients had symptoms of hematuria, frequent urination, urgency, and dysuria to varying degrees. Different degrees of prostate hyperplasia was seen during digital rectal examination and surgery, and the bladder was the most common. Lateral lobe hyperplasia is predominant. The mean postoperative follow-up time was 27.6 mo,and only 1 patient died of bladder cancer. In addition, 11 of the 12 patients had PSA values within the normal reference range. From the above description, it is not difficult to find that the clinical features of sclerosing adenopathy of the prostate are similar to those of benign prostatic hyperplasia and prostate cancer, and most of the patients' PSA values are Within the normal range, suggesting that sclerosing adenopathy may be a benign lesion. Pathologically, the lesions are very complex, with single or mixed glandular tubular, cord-like and linear structures, and focal distribution in benign prostate glands.Unlike prostate adenocarcinoma, immunohistochemical Expression of the basal cell (such as P63,CK5/6) and myoepithelial (Calponin, S100, SMA) markers, provides a very meaningful value for the identification of the two. In practice, when it is difficult to identify prostate sclerosing adenopathy and prostate cancer, we can use immunohistochemical markers to distinguish them. In addition, we can also use immunohistochemical PSA, and PSAP to identify sclerosing adenopathy and other neoplastic lesions such as nephrogenic adenoma. The above pathological characteristics can provide effective help for the follow-up in-depth study of the prostate. However, even though we performed a comprehensive systematic analysis of sclerosing adenopathy of the prostate, this study has some limitations. First,although we predicted a certain relationship between sclerosing adenopathy of the prostate and PSA values, there is still a lack of direct evidence for the two relevance of the person. Secondly, the sample size of this study is too small, and it is necessary to further supplement the sample size and explore it in depth. Finally, whether sclerosing adenopathy is a precancerous lesion of prostate cancer also lacks direct evidence to further prove. These issues need to be further explored in future work.
陳頤磊駐足,脫下帽子,交與副官,先是給孔圣人三鞠躬,又給孔守真鞠了一躬。嘴里喃喃念到:孔圣人,國難當(dāng)頭,玉石俱焚,借寶地辦幾件大事,失敬失敬。
Research conclusions
The objective is to investigate the clinicopathological features, diagnosis, and immunohistochemical phenotypes that distinguish prostate sclerosing adenopathy from other conditions.
Research perspectives
In 1983, Chen and Schiff reported a prostate lesion that they considered most notably similar to an adenomatous tumor[5]. Therefore, it was named sclerosing adenopathy[6]. Sclerosing adenopathy of the prostate, first reported in 1987 by Young[7], was previously known as an adenomatous prostate tumor, prostatic pseudoadenoma, and fibroepithelial nodules[8-10]. It was originally used to express the similarity of the lesions to testicular adenomatous tumors but was abandoned due to the recognition that the lesions were of prostatic origin based on the immunoreactivity of PSA in acinar cells. It was subsequently found that sclerosing adenopathy is superficially similar to the breast lesion of the same name, is composed of prostate epithelial cells rather than mesothelial cells, and is characterized by glandular hyperplasia of varying sizes in the intercellular substance[11-14]. Sclerosing adenopathy is well characterized both immunohistochemically and ultrastructurally, and there are currently several case reports and small series of this lesion[15,16].
FOOTNOTES
Feng RL and Tan ZY contributed equally to this work; Feng RL, Tao YP, Fu S, and Wang HF designed the study; Tan ZY and Tao YP contributed new reagents and analytical tools; Tao YP, Fu S and Wang HF analyzed data; Feng RL and Tan ZY wrote the manuscript. All authors have read and approved the final manuscript.
The study was authorized by the Ethics Committee at The Second Affiliated Hospital of Kunming Medical University.
The authors declared that no competing interests exist.
結(jié)合恩格斯為《政治經(jīng)濟(jì)學(xué)批判》所作的書評以及馬克思自己在《資本論》第一卷第二版跋中的說法,“我公開承認(rèn)我是這位大思想家的門人,而在關(guān)于價(jià)值學(xué)說的那一章,我在這里那里用黑格爾特有的表現(xiàn)方法來顯示一番”(馬克思,1963:第二版的跋XXIII)。必須承認(rèn):馬克思對于黑格爾辯證法的批判性改造,最直接的表現(xiàn)就是“政治經(jīng)濟(jì)學(xué)批判”的第一章“商品”。然而,從《政治經(jīng)濟(jì)學(xué)批判》的“商品”章到《資本論》的“商品”章,雖然在主題與內(nèi)容上存在連續(xù)性,都是敘述從商品向貨幣再到資本的辯證過渡這一最為抽象的內(nèi)容,但是二者之間卻存在細(xì)微的本質(zhì)的差別。
On reasonable request, the corresponding author will provide the analyzed datasets generated during the study.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed by the Creative Commons Attribution-NonCommercial (CC BY-NC 4.0) license,which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See:https://creativecommons.org/Licenses/by-nc/4.0/
運(yùn)動(dòng)訓(xùn)練對中老年冠心病患者PCI術(shù)后運(yùn)動(dòng)能力、心肺功能和認(rèn)知功能的作用······················趙夢飛 毛立偉 季 鵬 胡樹罡 高 苗 王 磊 (2,198)
China
Run-Lin Feng 0000-0002-3532-9450; Yan-Ping Tao 0000-0001-8868-7166; Zhi-Yong Tan 0000-0002-7771-0962; Shi Fu 0000-0003-4023-7195; Hai-Feng Wang 0000-0002-0891-5120.
Ma YJ
A
Ma YJ
猜你喜歡
北方建筑(2021年6期)2021-12-31 03:03:54
文苑(2020年10期)2020-11-07 03:15:36
現(xiàn)代裝飾(2020年6期)2020-06-22 08:43:12
現(xiàn)代裝飾(2020年4期)2020-05-20 08:55:08
電子制作(2019年7期)2019-04-25 13:17:14
電子制作(2018年18期)2018-11-14 01:48:16
鐵道通信信號(2018年2期)2018-04-18 12:18:23
電鍍與環(huán)保(2016年3期)2017-01-20 08:15:32
福建農(nóng)業(yè)科技(2016年10期)2016-03-07 09:46:49
少兒科學(xué)周刊·兒童版(2015年6期)2015-11-24 03:49:38
 World Journal of Clinical Cases2022年18期
World Journal of Clinical Cases2022年18期
- World Journal of Clinical Cases的其它文章
- Stem cells as an option for the treatment of COVID-19
- Development of clustered regularly interspaced short palindromic repeats/CRISPR-associated technology for potential clinical applications
- Effectiveness and postoperative rehabilitation of one-stage combined anterior-posterior surgery for severe thoracolumbar fractures with spinal cord injury
- Construction and validation of a novel prediction system for detection of overall survival in lung cancer patients
- Identification of potential key molecules and signaling pathways for psoriasis based on weighted gene coexpression network analysis
- Coinfection of Streptococcus suis and Nocardia asiatica in the human central nervous system: A case report