Rare case of hepatocellular carcinoma metastasis to urinary bladder: A case report
2022-06-28 03:53:18YohanKimYoungSeokKimJeongJuYooSangGyuneKimSusieChinAhrimMoon
World Journal of Clinical Cases 2022年16期
INTRODUCTION
HCC is the sixth most common cancer worldwide and the third leading cause of cancer-related mortality[1]. In addition, because its symptoms are not severe until the disease has progressed, most HCCs at the time of diagnosis are in an advanced stage.
隨著經濟社會的發展、科技的進步,居民對文化生活的需求不斷增長,“非遺”傳承與發展獲得了新的機遇。江蘇對“非遺”項目的傳承、保護和發展能夠應時而動,許多“非遺”傳承人也能夠因地制宜,不斷反思與變革,以適應時代發展的新需求。但是,由于社會“非遺”項目傳承、保護和發展的宏觀戰略與具體措施存在一些偏誤,以及一些“非遺”項目未能及時自我調整以適應社會的變化,江蘇“非遺”項目生態化傳承、保護和發展還存在令人擔憂的問題。
In HCC, not only intrahepatic metastasis, but also extrahepatic metastases to other sites such as lung, abdominal lymph nodes, bone, and adrenal glands are common [2-4]. The main routes of metastasis are vascular and lymphatic spread. Other routes such as spread through the bile duct and direct invasion are also possible[2,4-6]. However, metastasis of HCC into the urinary bladder is very rare. Here, we report a case of a solitary metastasis in the bladder found during transcatheter arterial chemoembolization (TACE) in a 60-year-old Korean woman previously diagnosed with chronic hepatitis B and HCC.
CASE PRESENTATION
Chief complaints
A 60-year-old female who underwent TACE twice for HCC visited our clinic after a bladder mass was found in a follow-up computed tomography (CT) scan.
History of present illness
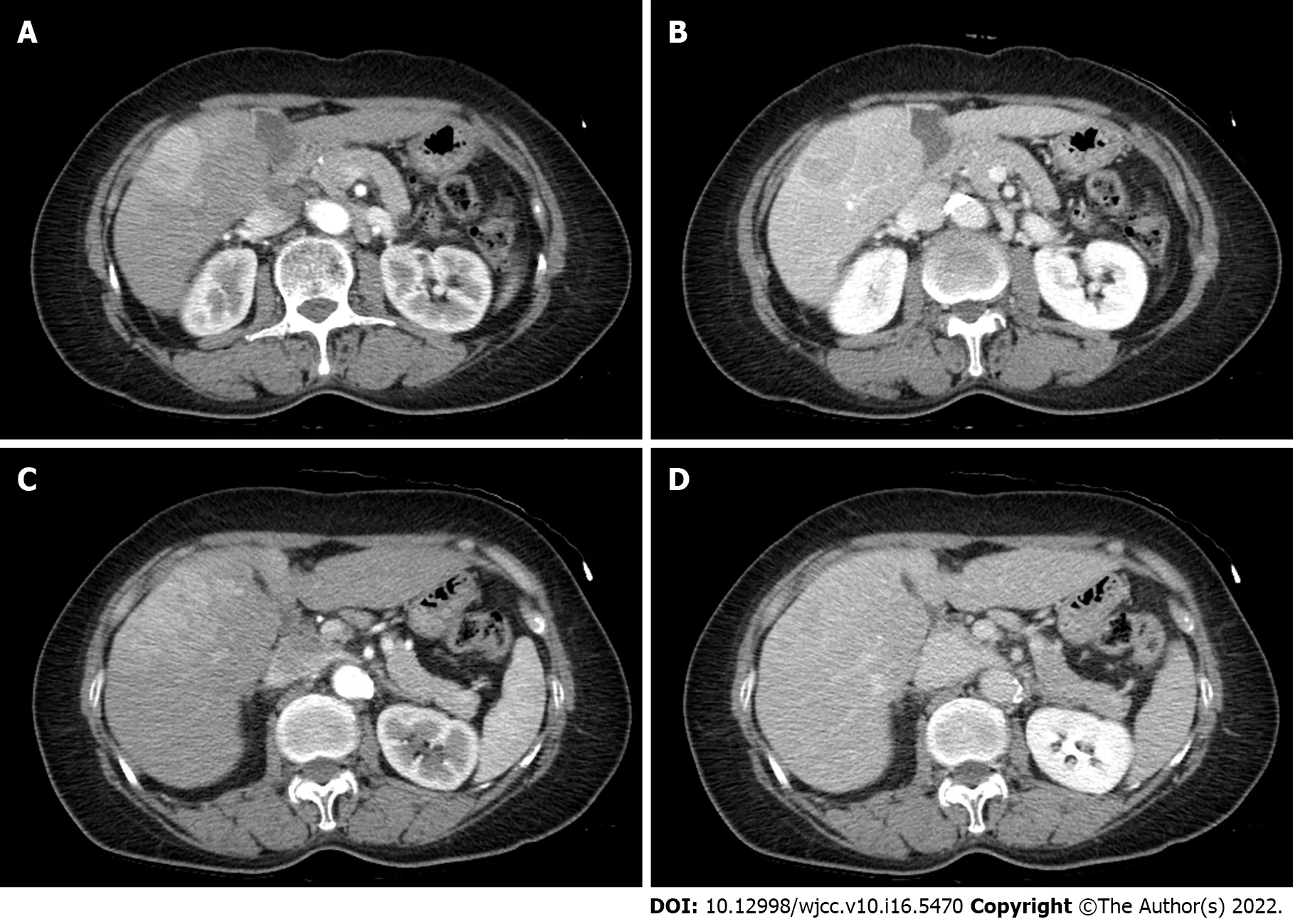
A 60-year-old female was found to be positive for hepatitis B surface antigen in a laboratory test. However, the patient denied both a history of hepatitis B and a family history. Therefore, HBV DNA test and abdominal ultrasonography were performed to work up the first diagnosis of hepatitis B. The HBV DNA test was confirmed to be positive. Liver cirrhosis and 3.6 cm sized HCC in segment 5 with infiltrative HCC in segment 8 were founded on abdominal ultrasound and liver dynamic CT (Figure 1).
In the liver function test performed during hospitalization, her aspartate aminotransferase and alanine aminotransferase levels were 24 U/L and 15 U/L, respectively, and her total bilirubin level was 0.78 mg/dL, all of which were normal. Her prothrombin time international normalized ratio was 1.05, which was within the normal range. Her albumin level was at 4.0 g/dL, which was also within the normal range.
For accurate diagnosis of the hepatic mass lesion suspected of HCC, we carried out enhanced liver dynamic magnetic resonance imaging (MRI) and liver biopsy on the S5 mass. As a result, HCC was diagnosed without evidence of portal vein invasion, lymph node metastasis, or distant metastasis (Figure 2). For multiple intrahepatic masses, we performed TACE immediately after diagnosis and at 5 mo after the 1
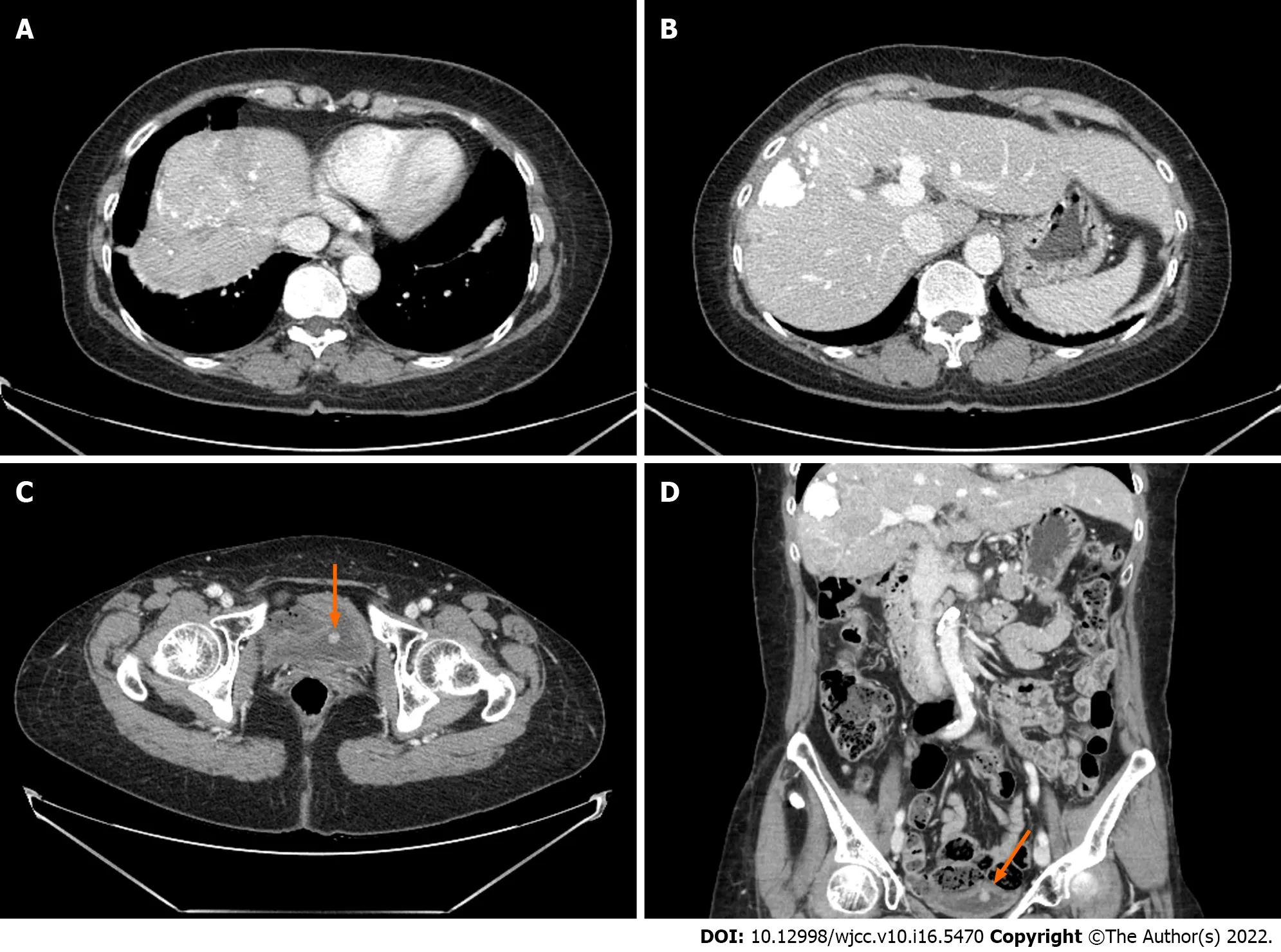
TACE on the main mass. TACE was performed by infusion of Adriamycin (50 mg) and lipiodol (10 mL) mixture, followed by embolization with gelfoam. After the second TACE, a urinary bladder tumor was newly discovered on liver dynamic CT performed to confirm treatment response (Figure 3).
History of past illness
The patient had a history of hysterectomy for uterine myoma 20 years ago. She was taking amlodipine 10 mg and olmesartan 40 mg as antihypertensive drugs.
Personal and family history
No special notes.
Physical examination
At the time of admission, the patient was 152.0 cm tall with a weight of 61.8 kg. Regarding her blood pressure, her systolic blood pressure was 124 mmHg and her diastolic blood pressure was 83 mmHg. Her heart rate (65 bpm) and body temperature (36.4°C) were normal. Her respiratory rate was also normal at 20 breaths per minute. Her mental status was alert. At the time of admission, the patient did not complain of any symptoms including abdominal pain. Abnormal findings such as ascites were not observed on abdominal examination.
在開始基西米河生態修復的基礎上,組織人員成立了專門的研究機構,制定和提出了奧基喬比湖生態修復、大沼澤地恢復及建設、佛州灣生態修復、入海河口治理等一系列計劃、方案,并在每個項目上投入了大量經費。
Laboratory examinations
通過兩種焊條的工藝評定對比試驗,選擇出符合圖紙技術要求的焊接材料,并制定相應的焊接工藝;該勵磁機風扇已在電廠平穩運行兩年多,表明焊材的選擇及焊接工藝的制定是正確的。
There were multinodular intrahepatic masses of S5 and S8. Because her Eastern Cooperative Oncology Group performance status was 0-1 and her Child-Pugh score was A, local treatment through TACE was first attempted on the main mass. Systemic chemotherapy was then planned. TACE was performed twice. Her AFP level was 3.5 ng/mL and her PIVKA-II level was 23.4 mAU/mL, which did not rise during the treatment period. A new urinary bladder tumor was found during regular follow-up with a contrast-enhanced liver CT. Transurethral resection of bladder tumor (TUR-BT) was performed for the diagnosis and treatment.
Imaging examinations
“‘赤城號’‘西京丸號’在外側躲避炮火,其余艦船呈一字陣型。‘吉野’四艦前隊游擊,旗艦‘松島號’為后隊核心,側舷對敵!”荷塘東岸,十二艘懸掛著太陽旗的航模艦艇同時啟動,在荷塘中激起一道自東向西的水波,用側舷那黑洞洞的炮口對準了北岸駛出的艦隊。
1.6 色譜條件 色譜柱:ACE C18-PFP(4.6 mm×150 mm,3 μm);流動相:A 相為乙腈,B 相為0.2% 甲酸水;梯度洗脫,洗脫程序如下:0~2.5 min A∶B=20∶80,2.5~4 min A∶B=60∶40;流速為 0.4 mL/min;平衡時間為 2 min;柱溫為25 ℃;進樣量為 2 μL。
FINAL DIAGNOSIS
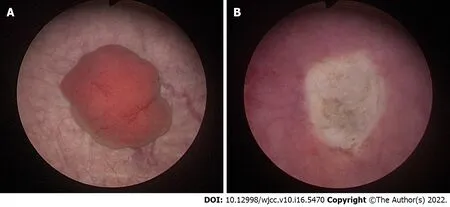
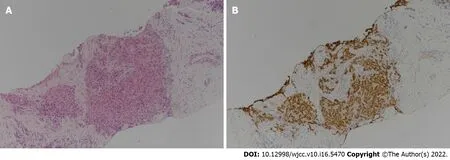
Transurethral resection of the bladder tumor was performed for the newly discovered bladder mass in the Urology Department. Cystoscopic findings revealed a 2 cm-sized well-defined reddish polypoid tumor on the posterior area of the bladder (Figure 4). The mass was removed using a hot loop. The pathology department confirmed that this tissue was metastatic HCC. In the case of HCC, it can be confirmed only by imaging study. She additionally underwent liver biopsy. Result was comparable to tissue of metastatic HCC. For the bladder tumor tissue, GATA binding protein 3 (GATA3) immunohistochemical staining that shows positive expression in the urothelium was negative, while arginase-1, which is significant in HCC, was positive. Thus, it was diagnosed as metastatic HCC (Figure 5).
TREATMENT
Her HBV DNA test was negative (< 10 IU/mL) from 46.0 IU/mL after entecavir administration. No other coinfections including HCV were identified. Levels of alpha-fetoprotein (AFP) and protein induced by vitamin K absence or antagonist-II (PIVKA-II) as tumor markers were found to be 3.9 ng/mL and 24.0 mAU/mL, respectively.
OUTCOME AND FOLLOW-UP
After TUR-BT, TACE, to which the mass had previously responded well, was performed again. Lenvatinib was then added as a systemic chemotherapy. Since then, she has been followed up with regular close monitoring in an outpatient clinic without any special problems.
DISCUSSION
In the present case, HCC was suspected as a liver mass with an early enhancing and delayed washout pattern on contrast-enhanced liver CT and MRI. HCC was confirmed by liver biopsy. Considering that the multinodular HCC showed no extrahepatic metastases and that the patient’s condition was stable, TACE was first tried to treat the main tumor mass. Systemic chemotherapy was then performed. After performing TACE twice, a newly appeared bladder tumor was found on follow-up liver dynamic CT. PET-CT performed at this time confirmed no prominent extrahepatic metastases. However, it was difficult to identify the bladder lesion due to its physiological uptake. Therefore, two possibilities, HCC metastasis to the bladder and primary bladder cancer, were considered. Considering their incidence, primary bladder cancer was considered first. After consulting with a urologist, it was considered that bladder tumor invasion was not deep in the imaging study. Thus, TUR-BT was performed for diagnosis and treatment.

Bladder cancer is the most common malignancy of the urinary tract. Its subtypes include urothelial carcinoma, squamous cell carcinoma, and adenocarcinoma. In the United States and Europe, urothelial (formerly transitional cell) carcinoma accounts for more than 90% of bladder cancer[9]. Most patients show symptoms of gross or microscopic hematuria. They are diagnosed with biopsy through urine cytology and cystoscopy. Treatment and prognosis of urothelial carcinoma depend on the stage and muscle invasion. Transurethral resection is the basic treatment for a non-muscle invasive disease. Intravesical therapy may be additionally considered for intermediate to high-risk patients[10]. Neoadjuvant or adjuvant chemotherapy can be considered based on radical cystectomy for a muscle invasive disease. Platinum-based chemotherapy and immunotherapy can be implemented for a metastatic bladder cancer[11].
She underwent TACE for HCC at S5 and S8 previously confirmed on CT. After the second TACE, a follow-up CT was taken one month later. On CT, a polypoid mass of 1 cm in the bladder which had not been seen in the previous study was observed without any viable HCC (Figure 3). Follow-up CT was taken three months later. After 3 mo, the bladder mass previously seen showed an increase in size from 1 cm to 1.8 cm. We additionally performed liver MRI, chest CT, and Positron emission tomography (PET)-CT. In these studies, probable viable HCCs at S8 were found. There were no other prominent distant metastases.
3) 零件尺寸進行微調、更改,無需進行繁雜的模型轉換,只需在CAD上更改后的二維輪廓圖上采點生成程序段,反應迅速,方便準確。
Treatment for HCC differs depending on its stage. The prognosis of HCC can vary greatly. Therefore, it is important to check for metastases at the first diagnosis. In addition to intrahepatic metastases for HCC, extrahepatic metastases are also known to be common[2]. Recently, PET-CT has been used so that small-sized early metastatic HCC will not be overlooked[7]. Extrahepatic metastasis occurs mainly in the lungs, lymph nodes, bones, adrenal glands, peritoneum, and omentum through direct invasion, vascular spread, or lymphatic spread[2-6]. The lung as the most metastatic site of HCC can be metastasized from the liver due to hematogenous spread through the pulmonary capillary network. If lung metastasis is present, hematogenous metastasis in other organs can also occur. Metastasis of the peritoneum and/or omentum is also important since tumor cells can propagate through ascites. Hematogenous spread through variceal collaterals and direct invasion of cancer are all possible[2]. However, metastasis to the urinary bladder alone without metastasis to other organs is known to be rare[8].
Mu:Lao Yang,you’d better sign this contract(簽賣身契).Or,you know,Master will be very angry!
Since liver biopsy is often not performed when HCC is first diagnosed, histological comparison with metastatic lesion is difficult. However, since this patient underwent liver biopsy, it was possible to perform histological comparison of the HCC tissue and the metastatic lesion sample obtained by TURBT. Hepatocyte antigen and GATA3 were negative in the immunohistochemical staining performed for the lesion of the bladder tumor. Unlike the primary HCC lesion, hepatocytes were not stained. Other immunohistochemical staining performed on bladder tumor tissue, Arginase-1 was positive and glypican-3 was weakly positive. Arginase-1 is the most sensitive and specific hepatocellular marker. It can be used to differentiate HCC from other tumors and HCC. If glypican-3 is positive, which is not expressed in normal or benign hepatocellular lesions, most HCC can be diagnosed[18,19]. With the help of immunohistochemical staining, bladder tumor could be diagnosed as metastatic HCC.
Based on previous reports[12-16], primary bladder cancer and metastatic HCC do not show significant difference in morphology under imaging study or cystoscopy. Thus, it is necessary to distinguish them through histological evaluation. For the diagnosis of metastatic HCC, it is necessary to histologically confirm HCC tumor cells in a bladder tumor. HCC tumor cells are similar to hepatocytes in morphology and function. They are polygonal and sinusoidal with a trabecular pattern. They can also secrete bile[17]. Metastatic HCC shows hepatocellular differentiation similar to HCC tumor cells.
In the present case, metastatic HCC to the bladder was diagnosed. However, hepatocytes of HCC might be well stained or not well stained in metastatic HCC as properties of HCCs might not be the same. Such molecular heterogeneity with primary tumor and its corresponding metastases showing different molecular marker expression is frequently found in HCC. This heterogeneity can affect treatment options and clinical outcome. It can also cause treatment failure[20]. Thus, accurate histological diagnosis and immunohistochemical staining through biopsy are needed. Recently, in addition to immunohistochemistry, comparison between HCC and metastatic lesions has been attempted by identifying properties of HCC and metastatic sites through genetic analysis using next generation sequencing[21].
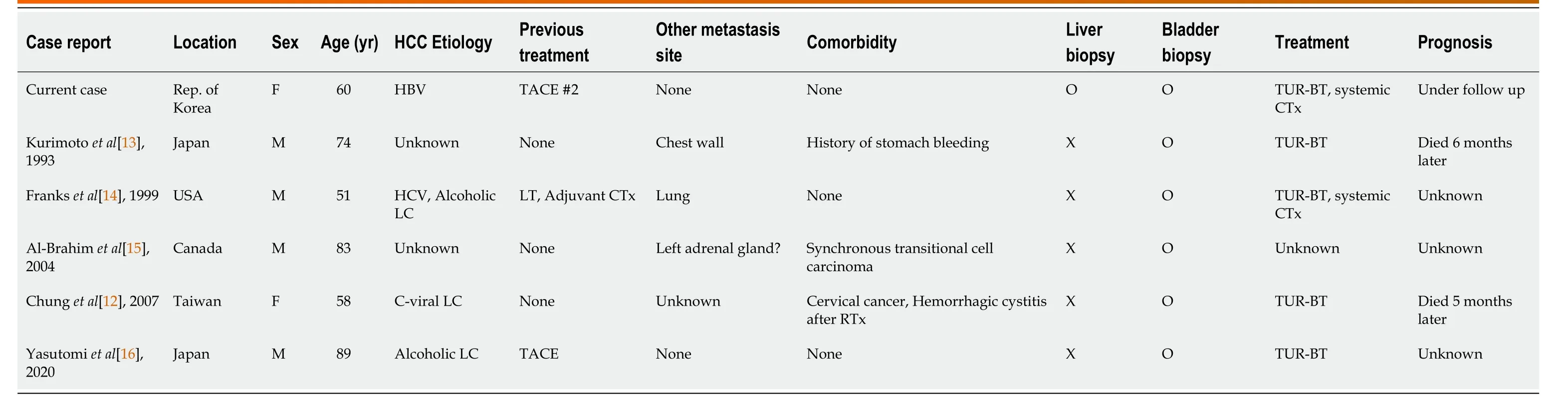
This case is an independent bladder metastasis case of hepatocellular carcinoma, which is very rare worldwide. Thus, this case report itself is meaningful. However, based on previous cases listed in Table 1, some variables such as bladder cancer after liver transplantation and hemorrhagic cystitis after radiotherapy could affect metastasis[12,14]. In the present case, there were no additional factors to consider in the primary site or the metastatic site. In addition, unlike previous studies, it is the only case report that compares biopsies from both primary and bladder metastasis sites. Because there is no established prognosis or optimal treatment modality due to its rarity, this case provides important data for future studies on HCC metastasis to the bladder.
CONCLUSION
HCC is often an advanced disease with metastases. It is clinically, molecularly, and biologically heterogenous. Even if extrahepatic metastases are not detected at the time of initial diagnosis of HCC, metastasis might progress during treatment. It is necessary to differentiate between primary cancer of other lesions and metastatic HCC. To distinguish between these two, histologic confirmation is recommended. Molecular expression and genetic analysis can also be considered for precise diagnosis. As in this case, distant metastasis to an uncommon organ may occur during HCC treatment. Thus, regular follow-up examinations and clinical attention are required even after treatment.
FOOTNOTES
Kim YS contributed to conceptualization, investigation, project administration, and writing—review & editing; Kim Y contributed to data curation; formal analysis, resources, visualization, and writing—original draft; Kim SG contributed to methodology; Yoo JJ contributed to supervision; all authors contributed to approval of final manuscript.
The requirement of informed written consent was waived by the Institutional Review Board (IRB) due to the retrospective nature of this case report.
The authors have no conflicts of interest relevant to this study to disclose.
The authors have read the CARE Checklist (2016). The manuscript was prepared and revised according to the CARE Checklist (2016).
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
South Korea
用SPSS 20.0統計學軟件分析該研究數據,計數資料以[n(%)]表示,行 χ2檢驗;計量資料以(±s)表示,行t檢驗。P<0.05為差異有統計學意義。
Yohan Kim 0000-0002-9878-2105; Young Seok Kim 0000-0002-7113-3623; Jeong-Ju Yoo 0000-0002-7802-0381; Sang Gyune Kim 0000-0001-8694-777X; Susie Chin 0000-0003-2754-1483; Ahrim Moon 0000-0001-6587-0013.
Liu JH
A
經濟危機迫使美國政府必須改變胡佛總統實行的政策。而羅斯福本人則是一個新自由主義者,在他執政后,美國國會成立了第一個全國性的救濟機構——聯邦緊急救濟署,并撥款5億美元作為各州實施緊急事業救助的資金。然而,以工代賑和直接救濟保障等模式給國家財政帶來了巨大的負擔。1935年,美國國會在人們提出各種社會保險方案的影響下通過了《社會保障法》,這是世界第一部以社會保障為內容的全面性法律,規定了社會保險包括下列4個方面:(1)養老金;(2)失業保險;(3)老年保險;(4)對盲人、需贍養的兒童和其他遭遇不幸者的救濟。法案致力于減少財政的負擔、提高社會福利水平。
Liu JH
1 Kew MC. Epidemiology of chronic hepatitis B virus infection, hepatocellular carcinoma, and hepatitis B virus-induced hepatocellular carcinoma.
2010 ; 58 : 273 -277 [PMID: 20378277 DOI: 10 .1016 /j.patbio.2010 .01 .005 ]
2 Katyal S, Oliver JH 3 rd, Peterson MS, Ferris JV, Carr BS, Baron RL. Extrahepatic metastases of hepatocellular carcinoma.
2000 ; 216 : 698 -703 [PMID: 10966697 DOI: 10 .1148 /radiology.216 .3 .r00 se24698 ]
3 Natsuizaka M, Omura T, Akaike T, Kuwata Y, Yamazaki K, Sato T, Karino Y, Toyota J, Suga T, Asaka M. Clinical features of hepatocellular carcinoma with extrahepatic metastases.
2005 ; 20 : 1781 -1787 [PMID:16246200 DOI: 10 .1111 /j.1440 -1746 .2005 .03919 .x]
4 Kanda M, Tateishi R, Yoshida H, Sato T, Masuzaki R, Ohki T, Imamura J, Goto T, Hamamura K, Obi S, Kanai F, Shiina S, Omata M. Extrahepatic metastasis of hepatocellular carcinoma: incidence and risk factors.
2008 ; 28 : 1256 -1263[PMID: 18710423 DOI: 10 .1111 /j.1478 -3231 .2008 .01864 .x]
5 Becker AK, Tso DK, Harris AC, Malfair D, Chang SD. Extrahepatic metastases of hepatocellular carcinoma: A spectrum of imaging findings.
2014 ; 65 : 60 -66 [PMID: 24239313 DOI: 10 .1016 /j.carj.2013 .05 .004 ]
6 Arora S, Harmath C, Catania R, Mandler A, Fowler KJ, Borhani AA. Hepatocellular carcinoma: metastatic pathways and extra-hepatic findings.
2021 ; 46 : 3698 -3707 [PMID: 34091729 DOI: 10 .1007 /s00261 -021 -03151 -3 ]
7 Lee JE, Jang JY, Jeong SW, Lee SH, Kim SG, Cha SW, Kim YS, Cho YD, Kim HS, Kim BS, Jin SY, Choi DL.Diagnostic value for extrahepatic metastases of hepatocellular carcinoma in positron emission tomography/computed tomography scan.
2012 ; 18 : 2979 -2987 [PMID: 22736922 DOI: 10 .3748 /wjg.v18 .i23 .2979 ]
8 Boldo E, Santafe A, Mayol A, Lozoya R, Coret A, Escribano D, Fortea-Sanchis C, Mu?oz A, Pastor JC, Perez de Lucia G,Bosch N. Rare Site Hepatocellular Carcinoma Metastasis.
2020 ; 7 : 39 -44 [PMID: 32274362 DOI:10 .2147 /JHC.S238963 ]
9 Malats N, Real FX. Epidemiology of bladder cancer. Hematol Oncol Clin North Am 2015 ; 29 : 177 -189 , vii [PMID:25836927 DOI: 10 .1016 /j.hoc.2014 .10 .001 ]
10 Sylvester RJ, van der MEIJDEN AP, Lamm DL. Intravesical bacillus Calmette-Guerin reduces the risk of progression in patients with superficial bladder cancer: a meta-analysis of the published results of randomized clinical trials.
2002 ;168 : 1964 -1970 [PMID: 12394686 DOI: 10 .1097 /01 .ju.0000034450 .80198 .1 c]
11 Chang SS, Bochner BH, Chou R, Dreicer R, Kamat AM, Lerner SP, Lotan Y, Meeks JJ, Michalski JM, Morgan TM, Quale DZ, Rosenberg JE, Zietman AL, Holzbeierlein JM. Treatment of Non-Metastatic Muscle-Invasive Bladder Cancer:AUA/ASCO/ASTRO/SUO Guideline.
2017 ; 198 : 552 -559 [PMID: 28456635 DOI: 10 .1016 /j.juro.2017 .04 .086 ]
12 Chung SD, Ho CH, Hung SF, Tai HC, Yu HJ, Huang KH. Metastatic hepatocellular carcinoma in the urinary bladder with radiation-induced hemorrhagic cystitis.
2007 ; 106 : 861 -863 [PMID: 17964966 DOI:10 .1016 /S0929 -6646 (08 )60052 -2 ]
13 Kurimoto S, Komatsu H, Doi N, Wakumoto Y, Tominaga T, Nishimura Y. [Metastasis of hepatocellular carcinoma to the urinary bladder].
1993 ; 32 : 64 -65 [PMID: 8383369 ]
14 Franks ME, Konety BR, Bastacky S, Gritsch HA. Hepatocellular carcinoma metastatic to the bladder after liver transplantation.
1999 ; 162 : 799 -800 [PMID: 10458375 DOI: 10 .1097 /00005392 -199909010 -00053 ]
15 Al-Brahim N, Alowami S, Davis I, Daya D. Synchronous transitional cell carcinoma and metastatic hepatocellular carcinoma in the urinary bladder: a case report.
2004 ; 11 : 2463 -2466 [PMID: 15636675 ]
16 Yasutomi E, Yano Y, Kodama Y. Urinary bladder metastasis of hepatocellular carcinoma incidentally revealed by hematuria.
2020 ; 52 : 115 [PMID: 31784350 DOI: 10 .1016 /j.dld.2019 .10 .011 ]
17 El Jabbour T, Lagana SM, Lee H. Update on hepatocellular carcinoma: Pathologists' review. World J Gastroenterol 2019 ;25 : 1653 -1665 [PMID: 31011252 DOI: 10 .3748 /wjg.v25 .i14 .1653 ]
18 Nguyen T, Phillips D, Jain D, Torbenson M, Wu TT, Yeh MM, Kakar S. Comparison of 5 Immunohistochemical Markers of Hepatocellular Differentiation for the Diagnosis of Hepatocellular Carcinoma.
2015 ; 139 : 1028 -1034 [PMID: 26230595 DOI: 10 .5858 /arpa.2014 -0479 -OA]
19 Choi WT, Kakar S. Immunohistochemistry in the Diagnosis of Hepatocellular Carcinoma.
2017 ; 46 : 311 -325 [PMID: 28506367 DOI: 10 .1016 /j.gtc.2017 .01 .006 ]
20 Zheng H, Pomyen Y, Hernandez MO, Li C, Livak F, Tang W, Dang H, Greten TF, Davis JL, Zhao Y, Mehta M, Levin Y,Shetty J, Tran B, Budhu A, Wang XW. Single-cell analysis reveals cancer stem cell heterogeneity in hepatocellular carcinoma.
2018 ; 68 : 127 -140 [PMID: 29315726 DOI: 10 .1002 /hep.29778 ]
21 Jin K, Lan H, Wang X, Lv J. Genetic heterogeneity in hepatocellular carcinoma and paired bone metastasis revealed by next-generation sequencing.
2017 ; 10 : 10495 -10504 [PMID: 31966388 ]
猜你喜歡
中國核電(2021年3期)2021-08-13 08:56:36
保健醫苑(2021年7期)2021-08-13 08:48:02
學生天地(2020年36期)2020-06-09 03:12:30
小學科學(學生版)(2020年5期)2020-05-25 07:11:32
山東冶金(2019年6期)2020-01-06 07:45:54
世界農藥(2019年2期)2019-07-13 05:55:12
華人時刊(2017年21期)2018-01-31 02:24:01
北方交通(2016年12期)2017-01-15 13:52:53
銅業工程(2015年4期)2015-12-29 02:48:39
領導文萃(2015年4期)2015-02-28 09:19:05
 World Journal of Clinical Cases2022年16期
World Journal of Clinical Cases2022年16期
- World Journal of Clinical Cases的其它文章
- Practical points that gastrointestinal fellows should know in management of COVID-19
- Electroconvulsive therapy plays an irreplaceable role in treatment of major depressive disorder
- Pleural involvement in cryptococcal infection
- Advances in the clinical application of oxycodone in the perioperative period
- Endoscopic surgery for intraventricular hemorrhage: A comparative study and single center surgical experience
- Pediatric acute myeloid leukemia patients with i(17)(q10) mimicking acute promyelocytic leukemia: Two case reports