Chordoma of petrosal mastoid region: A case report
2022-06-28 04:15:46JianJunHuaMingLiangYingZhenWeiChenCongHuangChuShanZhengYuJunWang
World Journal of Clinical Cases 2022年16期
INTRODUCTION
Chordoma is a rare low-grade malignant tumor originating from embryonic notochordal tissue with an incidence of less than 0.1/100000 individuals per year[1]. Chordoma is locally destructive and easily invades important structures, such as bones, nerves, and large blood vessels. Chordoma is likely to relapse after resection, but metastasis is rare. The pathogenesis of chordoma is unclear, and the disease is speculated to originate from residual cells of the notochord that develop during fetal development. The tumor usually occurs in the axial bone, especially at both ends. Most chordomas in the head and neck occur in the spheno-occipital junction, accounting for almost 35% of all chordomas[2]. A few cases occurring in the nasopharynx, paranasal sinuses, oropharynx, and jugular foramen have been reported[2,3], and approximately 0.2% of the cases reported in the literature occurred in the jugular foramen region[4] but not the petrosal mastoid region. Here, we report a case of chordoma in the left petrosal mastoid region with intracranial expansive growth resulting in cerebellar compression and deformation. The main clinical manifestation was a 2-year history of temporal pain and discomfort.
由表2可知,在1h時12T-103菌株對Cry1Ac蛋白降解降較為明顯,由15. 95 μg·L-1降低至0. 68 μg·L-1,降低程度達極顯著水平(p<0. 01),其降解率達92. 26%,此后12T-103菌株對Cry1Ac蛋白降解較為緩慢且不顯著。由此,12T-103菌株對Cry1Ac蛋白的降解能力較強。
馬克思主義中國化,簡而言之,即運用馬克思主義基本原理,密切聯系中國國情,研究新情況,創造性地制定正確的路線、方針和政策,以解決中國革命、建設的實際問題。
CASE PRESENTATION
Chief complaints
The patient underwent microscopic tumor resection through the upper and posterior windows of the left ear. During the operation, the tumor was found to be located in the epidura; the petrous part of the temporal bone and the surface of the occipital bone were eroded by the tumor; the left transverse sinus was involved; and the lower part of the tumor surrounded the nerves and vessels.
History of present illness
In 2012, no obvious cause for his left temporal pain and left-sided headache could be identified, and the patient had no symptoms of hearing loss, dizziness, nausea, or vomiting and no obvious redness, swelling, heat, pain, or structural aberrations in the adjacent skin.
We acknowledge Wang YJ and Huang C, Department of Radiology of Zhejiang provincial hospital of Chenese Medicine and No. 926 Hospital, Joint Logistics Support Force of PLA, for his special contribution to this case. We acknowledge the work of colleagues in the Pathology and Radiology Department in offering the original images and data related to this article.
History of past illness
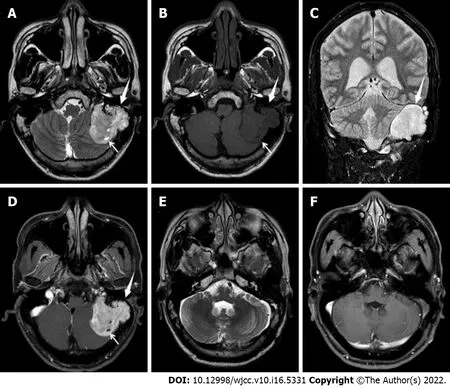
The patient recovered well after surgery, no specific discomfort was mentioned, and he was discharged 1 wk after the operation. As chordoma is a low-grade malignant tumor, the patient was re-examined once a year after the operation, and no obvious abnormality was found after follow-up for 5 years (Figure 1E and F).
Personal and family history
No specific genetic or family history of disease was identified.
Physical examination
Neurological examination revealed House Brackmann Grade II, gait disturbance, and tinnitus. The patient denied hearing loss and diplopia.
Laboratory examinations
No abnormality was found in the laboratory examination.
Imaging examinations
Magnetic resonance imaging (MRI) of the brain a lobulated mass in the left petrous mastoid region with a maximum interface of approximately 3.2 cm × 3.9 cm × 5.0 cm; surrounding bone absorption and destruction; uneven signal intensity on T2-weighted imaging (T2WI) (Figure 1A); isointensity and hypointensity on T1-weighted imaging (Figure 1B); hyperintensity on fluid-attenuated inversion recovery (Figure 1C); small cystic degeneration in the interior of the tumor (Figure 1A and B); and obvious enhancement of the solid components of the lesion on the contrast-enhanced scan (Figure 1D). No sign of involvement of the left jugular vein and left sigmoid sinus was observed. Left cerebellar compression and displacement were evident, but no brain parenchymal edema was noted.
FINAL DIAGNOSIS
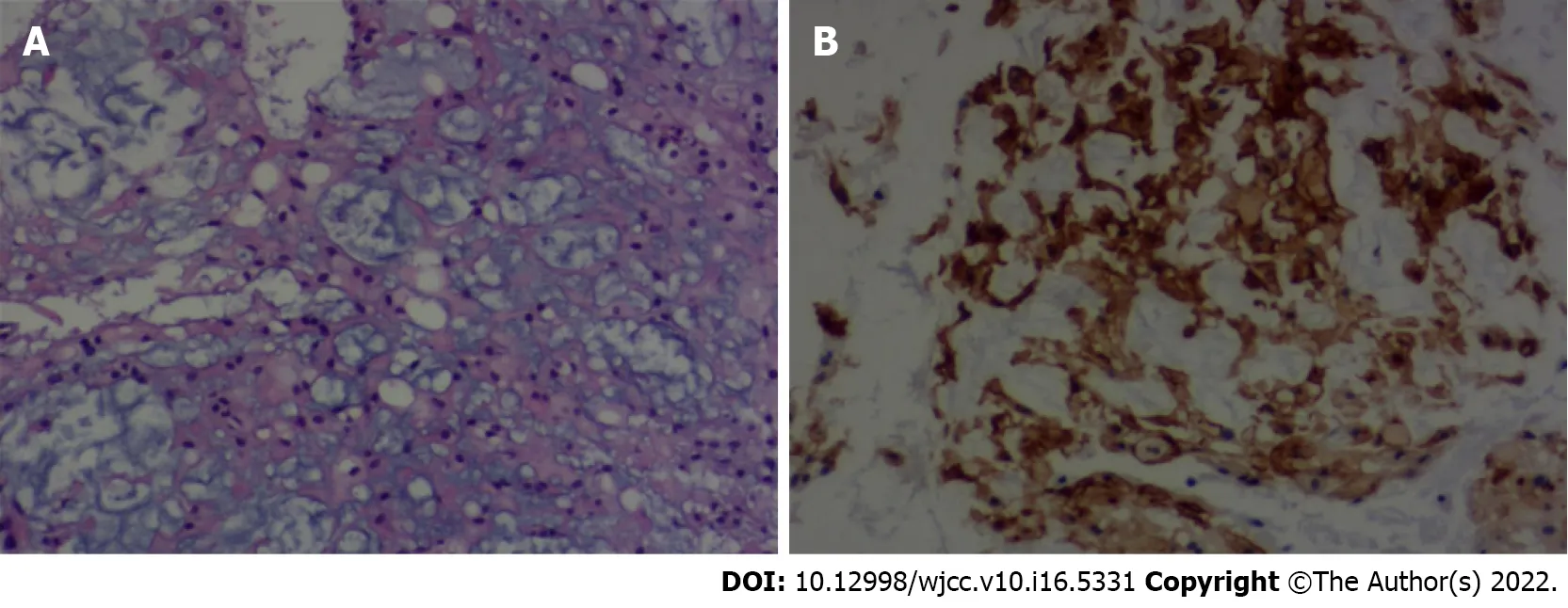
The gross specimen of the tumor was grayish-red and tough with a rich blood supply and had an unclear boundary. Microscopically, the tumor consisted of a dual cell population embedded in an abundant myxoid background. The cells were epithelioid polygonal in appearance with clear or eosinophilic cytoplasm, and a few mitotic cells were observed (Figure 2A). The immunohistochemical staining showed that vimentin, soluble protein-100 (S-100), epithelial membrane antigen (Figure 2B), and cytokeratin (CK)19 were positive, and CK staining was negative. The Ki67 antigen (Ki-67) fraction was approximately 1%. Ultimately, a diagnosis of chordoma was made.
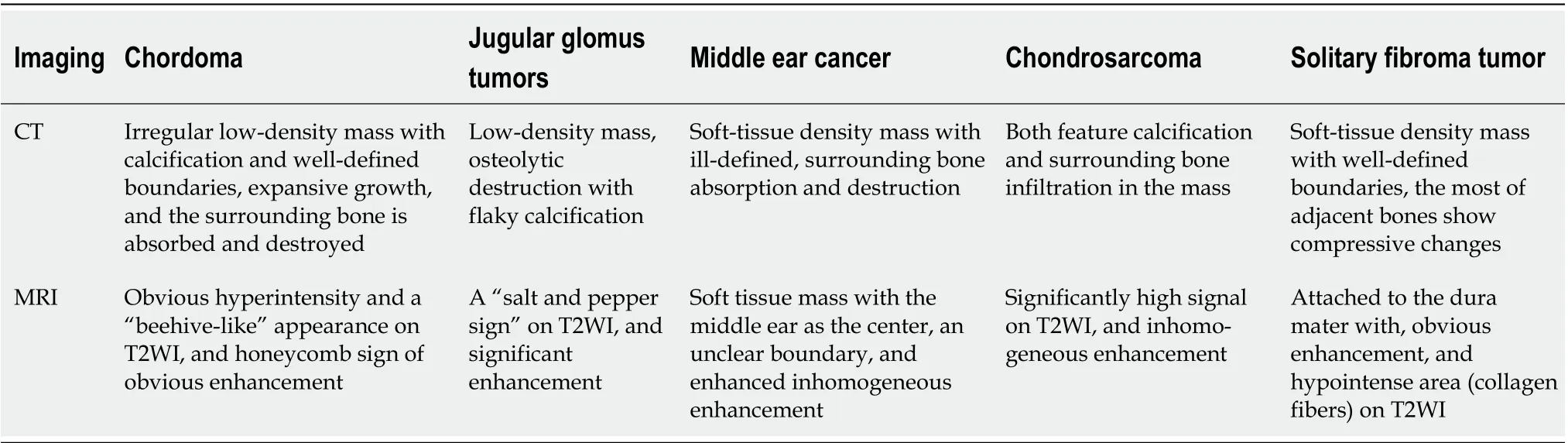
Chordoma in the petrous mastoid region should be differentiated from the following tumors (Table 1): (1) Jugular glomus tumors also show osteolytic destruction with flaky calcification, marginal bone infiltration, and a “salt and pepper sign” on T2WI, while chordomas show a high signal intensity, small cystic degeneration and obvious enhancement on T2WI; (2) Most patients with middle ear cancer have a history of chronic suppurative otitis media, and symptoms, such as earache, tinnitus, and ear canal bleeding, may occur. The main manifestations on MRI are a soft tissue mass with the middle ear as the center, an unclear boundary, surrounding bone absorption and destruction, and enhanced inhomogeneous enhancement; in contrast, although chordomas show expansion and growth, the boundary is clear, and the enhancement is obvious; (3) Chondrosarcoma and chordoma have overlapping ages of onset, both feature calcification and surrounding bone infiltration in the mass, and T2WI can show a significantly high signal intensity. Thus, distinguishing between these two diseases relying solely on imaging features is difficult, and the final diagnosis depends on histopathology; and (4) Solitary fibroma tumor (SFT) is a borderline tumor, and most SFTs are considered benign and more common in adults than children. MRI mainly shows well-defined masses mostly in the supratentorial space that are primarily attached to the dura mater with an abundant blood supply and obvious enhancement; a specific sign of intracranial solitary fibroma is a hypointense area (collagen fibers) on T2WI. In most cases, empty blood vessels can be observed, and most adjacent bones show compressive changes, while chordoma has hyperintensity on T2WI, and the surrounding bone is absorbed and destroyed.
TREATMENT
A 36-year-old man visited our hospital in December 2014 because of left temporal pain.
員工當月工資薪金所得低于稅法規定的費用扣除額,適用公式:應納稅額=(員工當月取得全年一次性獎金-員工當月工資薪金所得與費用扣除額的差額)×適用稅率-速算扣除數。
OUTCOME AND FOLLOW-UP
The patient had a history of hepatitis B infection for > 30 years, and his liver function was normal.
Chordoma is a rare, slow-growing, locally invasive malignant tumor originating from primitive notochordal tissues that develop longitudinally along the axis. Chordomas account for 3% of all primary bone tumors[5]. Approximately 50% of chordomas occur in the sacrococcyx, 30% of chordomas occur in the spheno-occipital region, and 20% of chordomas occur in the mobile spine[6]. Chordoma can occur at any age, and the most common age at diagnosis is 20–40 years. The gross specimen of the tumor showed lobulated and expansive growth with mucus, cystic necrosis, a small bleeding focus, calcification, ossification, and cartilage islands, which easily invaded the surrounding bone and caused extensive bone destruction. Histologically, the tumor was composed of droplet cells; the tumor tissue was divided into lobules by connective tissue; and the tumor cells were arranged into small clusters, flakes, strips, and acini with common degeneration and myxoid degeneration in the stroma. Histologically, chordoma appearance can be divided into the following three subtypes: classical, chondroid and dedifferentiated, and classical chordoma is the most common subtype. In addition, chondroid tumor growth is the slowest, and dedifferentiated tumor growth is the fastest.
DISCUSSION
腹腔鏡下大腸癌根治術后病人易出現排便困難、肛門墜脹等癥狀,將中醫治療、排便功能訓練、生物反饋訓練應用到病人治療及護理過程中,可一定程度上改善病人癥狀,提高病人生活質量。
Typical chordoma computed tomography (CT) findings mainly include: irregular low-density masses with well-defined boundaries; expansive growth, absorption and destruction of surrounding bone; irregular calcification inside the lesion; and obvious enhancement[7]. CT can accurately show bone and internal calcification but is insufficient for soft tissue analyses, and MRI is needed to facilitate further diagnosis.
The MRI findings of chordomas are diverse[8]. The typical MRI findings of chordomas in the clival region show obvious hyperintensity and a “beehive-like” appearance on T2WI, reflecting the histological characteristics of tumor tissue mainly composed of mucous stroma and droplet tumor cells secreting mucus. In this case, the presence of scattered strips and flakes with a low signal intensity suggested that the tumor was related to bone destruction, calcification, or a fibrous septum, and the high signal area in the tumor was separated and appeared beehive-like[9]. Enhancement of the chordoma on imaging is mainly inhomogeneous and obvious, while the dynamic enhancement scan shows continuous and slow enhancement, which is mainly caused by the adsorption of Gd-DTPA molecules to the mucin in the cell or cell interstitium, and the typical enhancement of chordoma shows a “honeycomb sign”[9]. In this case, the MRI findings differed from those of typical chordomas in the clival region. T2WI showed that the lesion was mainly slightly hyperintense with only narrow areas of hyperintensity. Given the pathological results, the low signal intensity on T2WI was likely due to the dense arrangement of tumor cells and scarcity of mucous cells. On the contrast-enhanced scan, the focus was not uniformly enhanced, the small cystic area was not enhanced, and the typical honeycomb sign was not observed.
貿易份額主要集中在越南,與越南的密切往來主要得益于邊境貿易(見圖4)。2012~2016年,廣西與越南貿易往來總額共981.89億美元,占廣西與東盟國家貿易總額的79.68%。其次為泰國,占5.46%;印度尼西亞占比4.87%。
CONCLUSION
Chordoma occurring in the petrous mastoid region is rare, its imaging findings are rarely reported, and an understanding of its MRI findings is lacking. However, in the differential diagnosis of petrous mastoid tumors, chordoma should be considered, especially when lobulated masses are found. The T2WI results are mainly characterized by a high signal intensity, obvious enhancement, and surrounding bone absorption and destruction. Therefore, an imaging examination can sufficiently show the extent of the focus and surrounding involvement, which can provide more useful information for clinical treatment.
ACKNOWLEDGMENTS
至于古代的衣服上為什么沒有口袋。這就是一個哲學問題了。就像我們有一個生活習慣,它融于生活,并且沒有給生活帶來什么不便之處,也就沒必要再做什么來改變這個習慣。所以,也沒有什么漢服沒口袋不方便之類的說法,畢竟從袖子里掏東西還是挺酷的,不是嗎?
“自強不息、艱苦奮斗,苦干實干、興業報國,敢為人先、追求卓越”,是蘭州石化的企業精神,也是蘭州石化的“魂”和“魄”。正是憑著這種精神,在60年的時光長河中,蘭州石化歷經改革改制浪潮,卻始終保持著隊伍不散、思想不亂、精神不垮、作風過硬。
FOOTNOTES
Hua JJ carried out the literature search and image and data collection, and drafted the manuscript; Ying ML reviewed the literature and drafted the manuscript; Chen ZW was the pathologist involved in the case, reviewed the literature, and drafted the manuscript; Huang C and Wang YJ made substantial contributions to the manuscript, including revising it critically for intellectual content; All authors read and approved the final manuscript.
Informed written consent was obtained from the patient for publication of this report and any accompanying images.
The authors declare that they have no conflict of interest to report.
The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).
于是,“走出去與請進來”自溫秀玲擔任院長的第一天就被提上日程并開始密集踐行。派出醫生到北京協和醫院進修婦產與風濕免疫專科,到中科院腫瘤醫院進修腫瘤專科,到阜外醫院進修心血管專科,到北醫三院骨科與生殖醫學專業學習……
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
China
Jian-Jun Hua 0000-0003-2350-3308; Ming-Liang Ying 0000-0002-2350-3308; Zhen-Wei Chen 0000-0003-4160-775X; Cong Huang 0000-0005-2350-3308; Chu-Shan Zheng 0000-0004-2350-3308; Yu-Jun Wang 0000-0003-3701-0598.
Ma YJ
Kerr C
Ma YJ
1 Stiller CA, Trama A, Serraino D, Rossi S, Navarro C, Chirlaque MD, Casali PG; RARECARE Working Group. Descriptive epidemiology of sarcomas in Europe: report from the RARECARE project.
2013 ; 49 : 684 -695 [PMID:23079473 DOI: 10 .1016 /j.ejca.2012 .09 .011 ]
2 Chen QQ, Liu Y, Chang CD, Xu YP. Chordoma located in the jugular foramen: Case report. Medicine (Baltimore) 2019 ;98 : e15713 [PMID: 31124949 DOI: 10 .1097 /MD.0000000000015713 ]
3 Tirabosco R, Mangham DC, Rosenberg AE, Vujovic S, Bousdras K, Pizzolitto S, De Maglio G, den Bakker MA, Di Francesco L, Kalil RK, Athanasou NA, O'Donnell P, McCarthy EF, Flanagan AM. Brachyury expression in extra-axial skeletal and soft tissue chordomas: a marker that distinguishes chordoma from mixed tumor/myoepithelioma/parachordoma in soft tissue.
2008 ; 32 : 572 -580 [PMID: 18301055 DOI: 10 .1097 /PAS.0 b013 e31815 b693 a]
4 Dwivedi RC, Ojha BK, Mishra A, Youssefi P, Thway K, Hassan MS, Agrawal N, Kazi R. A rare case of jugular foramen chordoma with an unusual extension.
2011 ; 137 : 513 -516 [PMID: 21576564 DOI:10 .1001 /archoto.2011 .66 ]
5 Ropper AE, Cahill KS, Hanna JW, McCarthy EF, Gokaslan ZL, Chi JH. Primary vertebral tumors: a review of epidemiologic, histological and imaging findings, part II: locally aggressive and malignant tumors.
2012 ; 70 :211 -9 ; discussion 219 [PMID: 21768918 DOI: 10 .1227 /NEU.0 b013 e31822 d5 f17 ]
6 Stacchiotti S, Sommer J; Chordoma Global Consensus Group. Building a global consensus approach to chordoma: a position paper from the medical and patient community.
2015 ; 16 : e71 -e83 [PMID: 25638683 DOI:10 .1016 /S1470 -2045 (14 )71190 -8 ]
7 Erdem E, Angtuaco EC, Van Hemert R, Park JS, Al-Mefty O. Comprehensive review of intracranial chordoma.
2003 ; 23 : 995 -1009 [PMID: 12853676 DOI: 10 .1148 /rg.234025176 ]
8 Meyers SP, Hirsch WL, Jr, Curtin HD, Barnes L, Sekhar LN, Sen C. Chordomas of the skull base: MR features.
1992 ; 13 : 1627 -36 [DOI: 10 .1148 /radiology.184 .1 .1609064 ]
9 Anis N, Chawki N, Antoine K. Use of radio-frequency ablation for the palliative treatment of sacral chordoma.
2004 ; 25 : 1589 -1591 [PMID: 15502143 ]
 World Journal of Clinical Cases2022年16期
World Journal of Clinical Cases2022年16期
- World Journal of Clinical Cases的其它文章
- Practical points that gastrointestinal fellows should know in management of COVID-19
- Electroconvulsive therapy plays an irreplaceable role in treatment of major depressive disorder
- Pleural involvement in cryptococcal infection
- Advances in the clinical application of oxycodone in the perioperative period
- Endoscopic surgery for intraventricular hemorrhage: A comparative study and single center surgical experience
- Pediatric acute myeloid leukemia patients with i(17)(q10) mimicking acute promyelocytic leukemia: Two case reports