妊娠期糖尿病及正常糖耐量孕婦血漿護骨素水平的比較
2012-06-05 05:10:34宋愛羚孫梅勵
基礎醫學與臨床 2012年1期
宋愛羚,聶 敏*,孫梅勵,王 瑛,2
(1.中國醫學科學院北京協和醫學院北京協和醫院內分泌科衛生部內分泌重點實驗室,北京 100730;2.山西醫科大學附屬第二臨床學院內分泌科,山西太原 030000)
妊娠期糖尿病及正常糖耐量孕婦血漿護骨素水平的比較
宋愛羚1,聶 敏1*,孫梅勵1,王 瑛1,2
(1.中國醫學科學院北京協和醫學院北京協和醫院內分泌科衛生部內分泌重點實驗室,北京 100730;2.山西醫科大學附屬第二臨床學院內分泌科,山西太原 030000)
目的 比較妊娠期糖尿病(GDM)和正常糖耐量(NGT)妊娠婦女在懷孕中晚期血漿護骨素(OPG)及相關因子水平。方法 NGT和GDM妊娠婦女各65例,于孕24~28周取靜脈血,-20℃低溫保存。用酶聯免疫吸附測定法(ELISA)測定血漿護骨素(OPG)水平,同時測定空腹血糖(FPG),空腹胰島素(FINS),糖化血紅蛋白(HbA1c),血脂水平,超敏C反應蛋白(hs-CRP),血細胞計數,計算胰島細胞功能(HOMA-B)和胰島素抵抗(HOMA-IR)的評估指數。結果 GDM 組和 NGT組血漿骨保護素(OPG)水平分別為2 619[1 968,3 917]ng/L和3 225[2 146,4 226]ng/L,兩組間無明顯差異。在NGT組,OPG與FINS(r=0.335;P<0.05)、HOMA-IR(r=0.363;P<0.05)和血小板計數(r=0.333;P<0.05)呈正相關,與載脂蛋白B(r=-0.254;P<0.05)呈負相關,在GDM組,未發現上述指標與OPG水平相關。結論 OPG可能參與了糖耐量正常孕婦孕期的胰島素抵抗和炎性反應。
護骨素;妊娠期糖尿病;空腹胰島素水平
*通信作者(corresponding author):nm_pumch@yahoo.com.cn
護骨素(Osteoprotegerin,OPG)又稱破骨細胞抑制因子,是由380個氨基酸組成的分泌型糖蛋白,屬于腫瘤壞死因子受體超家族的新成員。它阻止RANKL與RANK的結合,抑制RANK的作用,從而阻斷破骨細胞的生成,在骨代謝中發揮關鍵作用[1]。
研究發現,OPG不僅僅是一種骨保護因子,也是一種重要的血管調節因子。在發生血管鈣化、冠狀動脈疾病和中風時,患者血清OPG水平增加,其升高原因可能是機體發生的代償反應,通過增加OPG水平,延緩血管的鈣化[2]。文獻報道,新診斷的2型糖尿病患者血漿OPG水平增加[3]。患糖尿病的老年女性的OPG水平高于未患糖尿病的老年女性[4]。糖尿病患者的循環OPG水平與其微血管并發癥、尿微量白蛋白水平[5]和神經病變[6]顯著相關。以上研究表明OPG可能也參與了糖尿病的發病。對于妊娠婦女來說,胎盤是產生OPG的重要來源,在人類胎盤組織、胎膜及羊水中均存在OPG及OPGmRAN的表達。但有關OPG水平與妊娠糖尿病發病關系的研究國內外尚未見報道。本研究擬探討OPG在正常糖耐量(normal glucose tolerance,NGT)組以及妊娠期糖尿病(gestational diabetes mellitus,GDM)組中的水平差異及其相關影響因素,以明確其與GDM發病的關系。
1 對象與方法
1.1 研究對象
經研究對象知情同意,從2010年4月~2011年3月在北京協和醫院內分泌門診常規產前檢查的妊娠婦女中隨機選取研究對象,合并自身免疫性疾病以及孕前已有糖耐量異常或2型糖尿病者均予排除。所有受試者于懷孕24~28周進行50 g葡萄糖篩查實驗,1 h血糖大于7.8 mmol/L者繼續進行100 g葡萄糖耐量實驗(oral glucose tolerance test,OGTT),按照美國糖尿病診斷標準,空腹、1、2和3 h血糖閾值分別為:5.3、10.0、8.6 和7.8 mmol/L,其中任意兩個點超過正常范圍,診斷為妊娠期糖尿病,納入GDM組;4點全部正常診斷為糖耐量正常,納入NGT組。兩組分別納入65例研究對象。
1.2 研究方法
1.2.1 方法:測量身高,血壓,記錄懷孕前的體質量,計算孕前體質量指數(pre-BMI=體質量/身高2),并空腹抽取靜脈5 mL置 EDTA抗凝管中,3 000 r/min離心5 min后留血漿。酶聯免疫測定法測定真胰島素(TINS);葡萄糖氧化酶法測定空腹血糖(FPG)(Olympus公司);微柱層析法測定糖化血紅蛋白(HbA1c)(試劑由 Bio-Rd,INC公司);奧林巴斯全自動生化儀測定血脂各項指標(Olympus公司)。
1.2.2 ELISA測定OPG:酶聯免疫法檢測護骨素水平(Beneficical Solution,INC公司),批內變異系數為5.3%,批間變異系數為9.6%。
1.2.3 評價指標和計算公式:用HOMA指數來評估胰島細胞功能(HOMA-B)和胰島素抵抗(HOMAIR)。計算公式:HOMA-IR=FINS(mIU/L)×FBG(mmol/L)/22.5;HOMA-B=FINS(mIU/L)×20/(FPG-3.5)。
1.3 統計學分析
SPSS10.0軟件進行統計分析,所有指標進行正態性檢驗后,服從正態分布的用均數 ±標準差(±s)表示,非正態分布的用中位數和四分位數間距表示。兩組間均數的比較采用t檢驗或非參數檢驗。Person相關分析統計各項指標與OPG的關系。
2 結果
2.1 NGT和GDM組基本臨床資料的比較
GDM組的年齡,收縮壓,空腹血糖,空腹胰島素,糖化血紅蛋白,HOMA-IR,甘油三酯,載脂蛋白(a)均明顯高于對照組(P<0.05),而HOAM-B、高密度脂蛋白和膽固醇則低于對照組(P<0.05)(表1)。
表1 研究對象臨床和生化指標的比較Table 1 The comparision of clinical and metabolic characteristics of the subjects studied( ± s or medians,n=65)
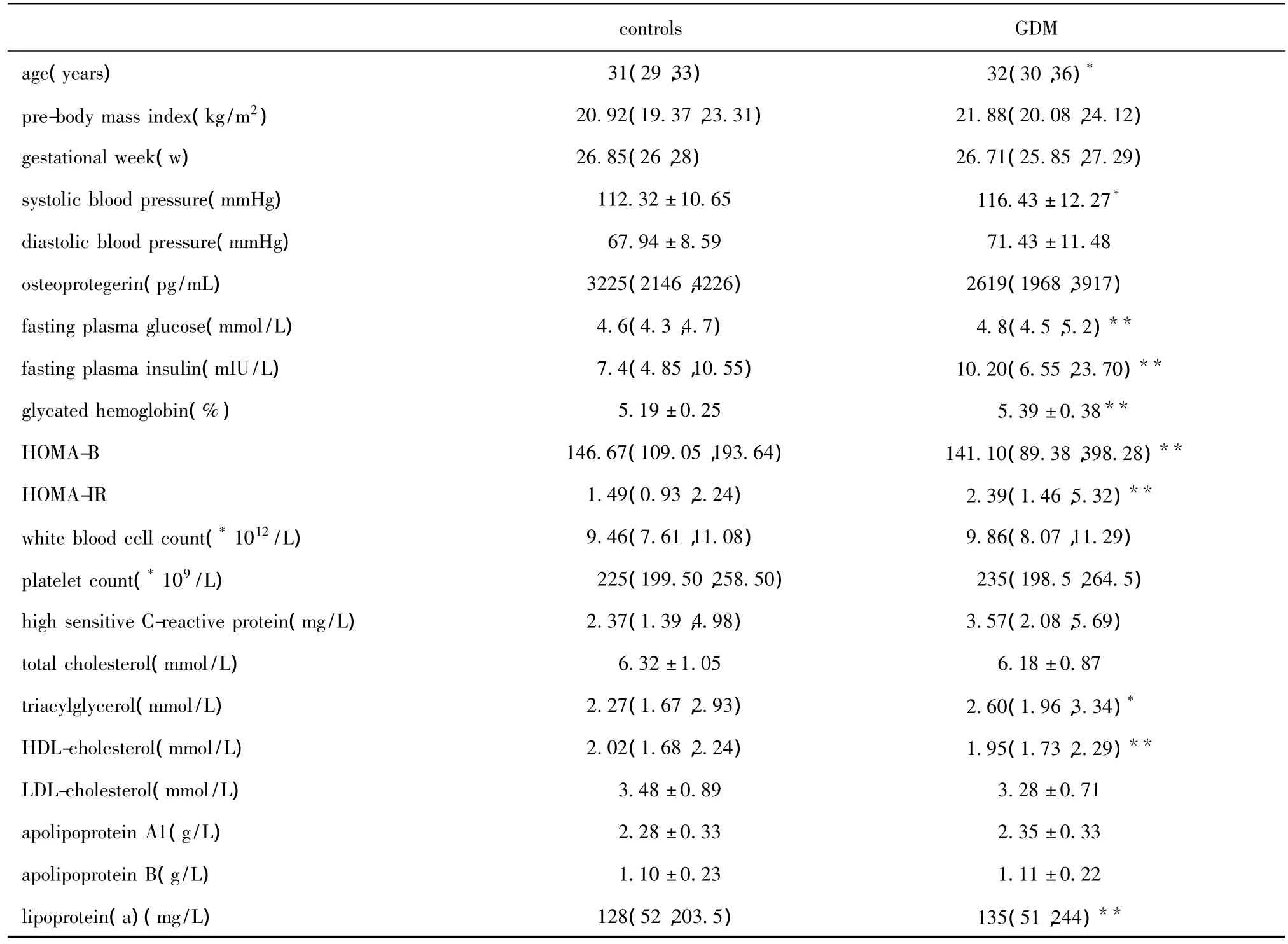
表1 研究對象臨床和生化指標的比較Table 1 The comparision of clinical and metabolic characteristics of the subjects studied( ± s or medians,n=65)
*P <0.05,**P <0.01 compared with control.
controls GDM age(years) 31(29,33) 32(30,36)*pre-body mass index(kg/m2) 20.92(19.37,23.31) 21.88(20.08,24.12)gestational week(w) 26.85(26,28) 26.71(25.85,27.29)systolic blood pressure(mmHg) 112.32±10.65 116.43±12.27*diastolic blood pressure(mmHg) 67.94±8.59 71.43±11.48 osteoprotegerin(pg/mL) 3225(2146,4226) 2619(1968,3917)fasting plasma glucose(mmol/L) 4.6(4.3,4.7) 4.8(4.5,5.2)**fasting plasma insulin(mIU/L) 7.4(4.85,10.55) 10.20(6.55,23.70)**glycated hemoglobin(%) 5.19±0.25 5.39±0.38**HOMA-B 146.67(109.05,193.64) 141.10(89.38,398.28)**HOMA-IR 1.49(0.93,2.24) 2.39(1.46,5.32)**white blood cell count(*1012/L) 9.46(7.61,11.08) 9.86(8.07,11.29)platelet count(*109/L) 225(199.50,258.50) 235(198.5,264.5)high sensitive C-reactive protein(mg/L) 2.37(1.39,4.98) 3.57(2.08,5.69)total cholesterol(mmol/L) 6.32±1.05 6.18±0.87 triacylglycerol(mmol/L) 2.27(1.67,2.93) 2.60(1.96,3.34)*HDL-cholesterol(mmol/L) 2.02(1.68,2.24) 1.95(1.73,2.29)**LDL-cholesterol(mmol/L) 3.48±0.89 3.28±0.71 apolipoprotein A1(g/L) 2.28±0.33 2.35±0.33 apolipoprotein B(g/L) 1.10±0.23 1.11±0.22 lipoprotein(a)(mg/L) 128(52,203.5) 135(51,244)**
2.2 NGT和GDM組OPG水平的比較及OPG與臨床指標的相關研究結果
統計結果提示,血漿OPG水平在GDM組是2 619(1 968,3 917)ng/L,在 NGT 組 是 3 225(2 146,4 226)ng/L,兩組間無明顯差異。按照ADA的診斷標準分層研究發現,在NGT組中,OPG與空腹胰島素、HOMA-IR和血小板數3個指標呈正相關(P<0.01),與載脂蛋白 B呈負相關(P<0.05)。
3 討論
本研究首次探討了血漿OPG水平與GDM相關指標的關系。研究發現血漿OPG水平在GDM組和NGT組無明顯差異,與以前的文獻報道結果相似[7-8]。但另外一項研究認為,與體質量指數(body mass index,BMI)匹配的對照組相比,OPG水平在有GDM病史的婦女中是增加的[9],結果與我們的研究不同。可能是研究的人群不一樣,每個人群所處的疾病階段不同引起的。
本研究發現NGT組,OPG與空腹胰島素以及HOMA-IR呈正相關,一定程度上支持了胰島素抵抗與OPG水平的相關作用。而在GDM組OPG水平與胰島素以及HOMA-IR不相關,可能是GDM組中其他影響胰島素抵抗的作用因素掩蓋了OPG對其的作用。目前研究表明,循環中OPG水平和胰島素抵抗是否明確相關尚無定論[7,10]。有的研究并沒有發現在代謝綜合征患者中OPG水平的明顯改變[11],但在肥胖的患者[12]和老年男性[13]血漿 OPG水平與胰島素抵抗相關。正常血糖鉗夾實驗表明:胰島素能使血漿OPG水平下降[14]。同時,體外培養的血管內皮細胞產生的OPG水平受到胰島素敏感性及其作用的影響,用胰島素增敏劑格列酮類藥物和胰島素均可減少血管平滑肌細胞產生OPG。胰島素抵抗時OPG水平上升的機制,可能與外周胰島素抵抗產生的胰島素活性的下降導致了OPG的累積[10]有關。
本研究還發現,血漿OPG水平與血小板數存在明顯的正相關,關于OPG和炎性反應之間的關系目前尚存在爭議。研究報道有GDM病史的婦女血漿OPG水平和炎性因子超敏C反應蛋白(C-reactive protein,CRP)之間有著明顯的相關性[8]。一項來自達拉斯心臟病學的研究同樣發現血漿OPG水平和CRP明顯相關。而在一項小樣本的研究中并沒有發現其與炎性標志物之間存在關系[15]。另一項研究發現有GDM病史的患者中,超敏C反應蛋白、纖維蛋白酶原以及OPG水平都是增加的[8]。而本研究并沒有發現這種相關性。
大量研究報道循環中OPG水平與心血管危險因素以及動脈粥樣硬化相關。在研究中發現OPG水平和載脂蛋白B有一定的相關性,而載脂蛋白是心血管危險因素之一。但未發現與其他血脂指標有明顯相關性,鑒于研究樣本量較少,因此本研究僅提示OPG有可能參與了脂代謝,需進行大樣本量的研究以證實。
在糖耐量正常懷孕婦女中OPG可能參與了妊娠期的胰島素抵抗和炎性反應。
[1]Simonet WS,Lacey DL,Dunstan CR,et al.Osteoprotegerin:a novel secreted protein involved in the regulation of bone density[J].Cell,1997,89:309 -319.
[2]Kim SM,L eet J,Ryu OH,et al.Serum osteop rotegerin levels are associated with inflammation and pulsew avevelocity[J].Clin Endocrinol,2005,63:594 -598.
[3]Jung CH,Lee WY,Kim SY,et al.The relationship between coronary artery calcification score,plasma osteoprotegerin level and arterial stiffness in asymptomatic type 2 DM[J].Acta Diabetol,2010,47:145 -152.
[4]Browner WS,Lui LY,Cummings SR.Associations of serum osteoprotegerin levels with diabetes,stroke,bone density,fractures,andmortality in elderlywomen [J].J Clin Endocrinol Metab,2001,86:631-637.
[5]Xiang GD,PU JH,Zhao LS,et al.Association between plasma osteoprotegerin concentrations and urinary albumin excretion in type 2 diabetes[J].Diabet Med,2009,26:397-403.
[6]Terekeci HM,Senol MG,Top C,et al.Plasma osteoprotegerin concentrations in type 2 diabetic patients and its association with neuropathy[J].Exp Clin Endocrinol Diabetes,2009,117:119 -123.
[7]Akinci B,Celtik A,Yuksel F,et al.Increased osteoprotegerin levels in women with previous gestational diabetes developing metabolic syndrome[J].Diabetes Res Clin Pract,2011,91:26-31.
[8]Akinci B,Demir T,Celtik A,et al.Serum osteoprotegerin is associated with carotid intima media thickness in women with previous gestational diabetes[J].Diabetes Res Clin Pract,2008,82:172 -178.
[9]Madarasz E,Tamas G,Tabak AG,et al.Osteoprotegerin levels in women with prior gestational diabetes mellitus[J].Diabetes Care,2009,32.
[10]Yaturu S,Rains J,Jain SK.Relationship of elevated osteoprotegerin with insulin resistance,CRP,and TNFalpha levels in men with type 2 diabetes[J].Cytokine,2008,44:168-171.
[11]Golledge J,Leicht AS,Crowther RG,et al.Determinants of endothelial function in a cohort of patients with peripheral artery disease[J].Cardiology,2008,111:51-56.
[12]Ugur-Altun B,Altun A,Gerenli M,et al.The relationship between insulin resistance assessed by HOMA-IR and serum osteoprotegerin levels in obesity[J].Diabetes Res Clin Pract,2005,68:217 -222.
[13]Gannage-Yared MH,Fares F,Semaan M,et al.Circulating osteoprotegerin is correlated with lipid profile,insulin sensitivity,adiponectin and sex steroids in an ageing male population[J].Clin Endocrinol(Oxf),2006,64:652 -658.
[14]Jorgensen GM,Vind B,Nybo M,et al.Acute hyperinsulinemia decreases plasma osteoprotegerin with diminished effect in type 2 diabetes and obesity[J].Eur J Endocrinol,2009,161:95 -101.
[15]Van Campenhout A,Golledge J.Osteoprotegerin,vascular calcification and atherosclerosis [J].Atherosclerosis,2009,204:321-329.
Comparision of plasma osteoprotegerin in women with gestational diabetes mellitus and normal glucose tolerance
SONG Ai-ling1,NIE Min1*,SUN Mei-li1,WANG Ying1,2
(1.Key Laboratory of Endocrine,Ministry of Health,Dept.of Endocrinology,PUMC Hospital,CAMS & PUMC,Beijing 100730;2.the Secondly Affiliated Clinical College,Dept.of Endocrinology,ShanXi Medical College,Taiyuan 030000,China)
ObjectiveTo determine the plasma osteoprotegerin(OPG)levels in pregnant women with gestational diabetes mellitus(GDM)and normal glucose tolerance(NGT)during their mid-late pregnancy,and to investigate the relationship between OPG and its involved factors.MethodsSixty-five women with GDM and 65 women with NGT were enrolled.Blood samples of each participant were collected during the 24~28 weeks of gestation and stored at-20℃ until use.Plasma concentration of OPG was measured by enzyme linked immunosorbent assay(ELISA).The level of fasting plasma glucose(FPG),fasting insulin(FINS),glycated hemoglobin(HbA1c),lipid,high-sensitivity C-reactive protein(hs-CRP),blood cell count,and calculated the homeostasis model assessment of beta-cell function(HOMA-B)and insulin resistance(HOMA-IR)were also measured.ResultsThe levels of plasma OPG in GDM and NGT groups were 2 619[1 968,3 917]and 3 225[2 146,4 226]ng/L.There was no significant different between the two groups.In the group of NGT,OPG levels were positively correlated with FINS(r=0.335,P<0.05),HOMA-IR(r=0.363,P<0.05),platelet count(r=0.333,P<0.05)and negatively related with apolipoprotein B(r= -0.254,P<0.05),but in GDM group,the relation between OPG and the biomarker mentioned above was not found.ConclusionsOPG may be involved in insulin resistance and inflammation during the pregnancy in women with NGT.
osteoprotegerin;gestational diabetes mellitus;fasting insulin
R 714.14
A
1001-6325(2012)01-0021-04
2011-09-28
2011-11-23
國家自然科學基金(81070630)
猜你喜歡
現代臨床醫學(2022年4期)2022-09-29 07:38:00
中老年保健(2022年5期)2022-08-24 02:35:42
中老年保健(2022年1期)2022-08-17 06:14:56
中老年保健(2021年5期)2021-08-24 07:07:20
中老年保健(2021年11期)2021-08-22 03:15:16
昆明醫科大學學報(2021年4期)2021-07-23 01:21:50
中國生殖健康(2019年2期)2019-08-23 08:12:10
海南醫學(2016年8期)2016-06-08 05:43:00
中國衛生標準管理(2015年1期)2016-01-14 03:41:27
醫學研究雜志(2015年9期)2015-07-01 17:28:15