NRS2002 assesses nutritional status of leukemia patients undergoing hematopoietic stem cell transplantation
2012-11-08 07:30:10PengLiuZhaoFengZhangJingJingCaiBoShiWangXiaYan
Peng Liu, Zhao-Feng Zhang, Jing-Jing Cai, Bo-Shi Wang, Xia Yan
1Department of Clinical Nutrition, Peking University People’s Hospital, Beijing 100044, China; 2Department of Nutrition and Food Hygiene, School of Public Health, Peking University, Beijing 100191, China; 3Department of Hematology, Peking University People’s Hospital, Beijing 100044, China
Introduction
Hematopoietic stem cell transplantation (HSCT) is widely used in the treatment of hematological malignancies and some solid tumors (1,2).Patients with hematological malignancies are frequently accompanied with malnutrition (3).Prior to the transplantation, patients usually receive high-dose chemotherapy and/or general radiotherapy, which make their nutrition status injured in different extents (4,5).Nutritional status is an important variable for prognosis of diseases (6).Malnutrition patients have high incidence of complications and mortality (7), prolonged hospitalization days, increased medical costs (8), and poor quality of life (9).Malnutrition will influence the treatment effect of HSCT and the reconstitution of hematopoietic and immune functions (10).Therefore, correctly assessing the nutritional status of patients before and after HSCT is important for a successful transplantation and improving the quality of life after transplantation (11).Nutritional risk screening 2002 (NRS2002) is the first nutrition risk screening tool developed on the basis of evidence-based medicine, and the selected core indicators reflecting nutritional risk are derived from 128 randomized controlled trials (RCT),suitable for nutrition risk screening for inpatients and easy to use (12,13).This study intended to investigate whether NRS2002 is suitable for nutritional risk screening for leukemia patients with HSCT, and whether there are risk differences in other conditions, such as age and gender differences; and to find the methods and indicators of nutritional risk screening and assessment for these patients before and after transplantation, in order to give them timely intervention to guarantee the successful completion of the entire transplantation process.

Table1 Basic information of patients (N=99)
Materials and methods
Subjects
A total of 99 leukemia patients receiving HSCT were sampled from Peking University People’s Hospital.The mean age of these patients was (32.45±11.26) years (range,18-56 years), and the mean time in laminar air flow room(LAFR) was (30±4) d ( range, 23-39 d).All 99 patients were told the fact, and written informed consent was obtained.The study was approved by the Ethic Committee of Peking University People’s Hospital.The basic information of these patients is showed inTable 1.
Assessment methods
After continuously sampling in the designated sites, two trained nutritionists used NRS2002 to screen the nutritional risk of leukemia patients on the enrollment day (before HSCT) and the HSCT completion day (after HSCT).
NRS2002 was developed by the Danish Association of Parenteral and Enteral Nutrition (DAPEN) and recommended by the European Society for Parenteral and Enteral Nutrition (ESPEN).Nutritional risk judgment criteria included: (I) severity of impact of the primary disease on nutritional status, (II) recent (1-3 months) weight change, (III) change of food intake within a week, (IV) body mass index (BMI), and (V) over the age of 70, scored 1.Scoring method was applied to measure the risk, and NRS score ≥3 was defined as nutritional risk (14).
The application of NRS2002 with BMI of Chinese population to screen the nutrition risk of inpatients and to determine whether nutritional support should be given had been shown to be feasible (15).Therefore, in this study,the assessment standard of BMI was Chen’s standard (16),and BMI <18.5 kg/m2is defined as undernutrition {BMI =weight (kg)/[height (m)]2}.
Quality control
Investigators must be trained before the survey; unified nutritional assessment questionnaire was adopted for screening and assessment; height and weight of patients with ward clothes were measured without shoes at fasting.
Statistical analysis
SPSS statistical software version 16.0 (SPSS Inc., Chicago,IL, USA) was used for statistical analysis.Measurement data were expressed as.Enumeration data were expressed as percentage.The differences of enumeration data, such as gender, age and matching degree, were compared by χ2test,while the differences of enumeration data, such as recent(1-3 months) weight loss, reduced food intake within one week and BMI, were compared by continuity correction.P<0.05 was considered statistically significant.
Results
Nutritional risk screening in patients before HSCT
Among 99 leukemia patients, 22 (22.2%) had nutritional risk, whose NRS2002 score ≥3, and nutritional support should be needed (Table 2).
Nutritional risk screening in different groups before HSCT
The patients were grouped according to gender, age and other conditions, and the incidence of nutritional risk was compared.The results showed that there was no significant difference in the nutritional risk incidence according to gender (P>0.05), while there were significant differences according to age, matching degree, weight loss, reduced intake or BMI (P<0.01) (Table 3).
Nutritional risk screening in patients after HSCT
All patients had nutritional risk after HSCT (Table 4).
Discussion
HSCT is an important treatment method for leukemia.The nutritional status is very important for patients after HSCT.Malnutrition can affect the results of HSCT, which is related to patient’s prognosis and quality of life.
NRS grades consist of disease state grade, nutritional status grade and age grade.The subjects of this study were patients with leukemia and less than 70 years old, so the scores of disease state and age were 2 and 0, respectively.Therefore, this study compared the nutritional risk in three aspects: BMI, recent (1-3 months) weight loss, and reduced food intake within a week, and the results showed a significant difference in each aspect, which further explained the results of our previous study (17) showing NRS2002 was appropriate for nutritional risk screening of leukemia patients before HSCT.The result that BMI should be concerned about before HSCT was also consistent with other report (18).
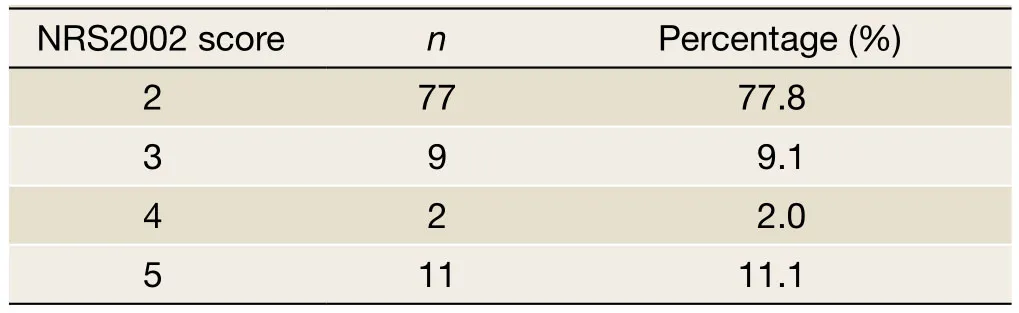
Table 2 Nutritional risk screening before HSCT (N=99)
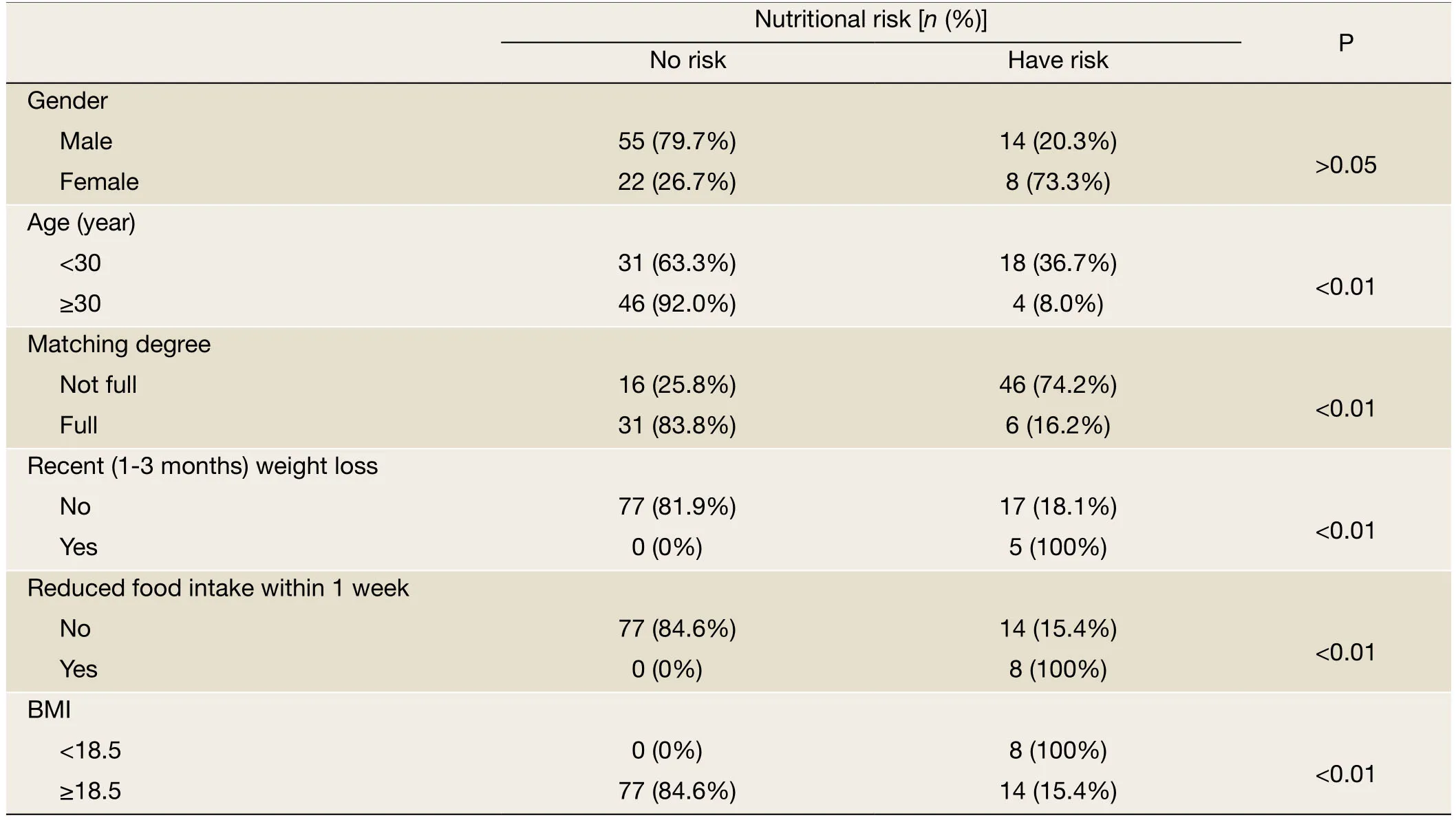
Table 3 Nutritional risk screening in different groups before HSCT (N=99)
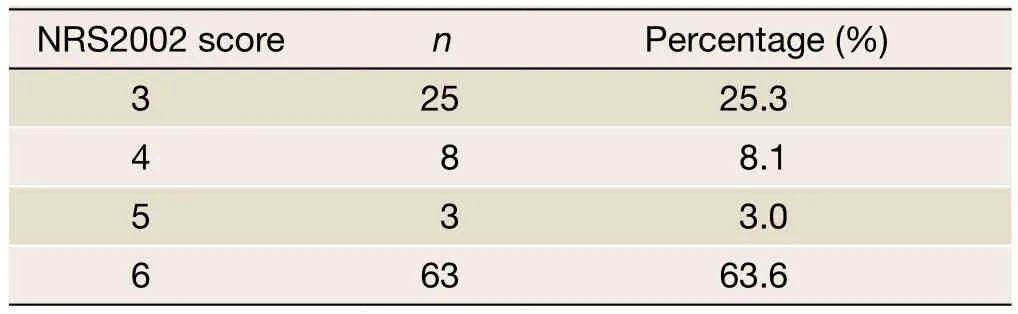
Table 4 Nutritional risk screening after HSCT (N=99)
Furthermore, this study also compared the risk incidence of different gender, age and matching degree, and the results showed that there was no significant difference between male and female, while there were higher incidence rates of nutritional risk in patients less than 30 years old and not-full matched, suggesting that these patients should be paid more attention to.
This study showed that all the patients after HSCT had nutritional risk, because their diagnosis was all “HSCT”,which made all the patients receive 3 score in the aspect of disease state grade, and the total scores were all equal to or greater than 3.Therefore, NRS2002 may not be appropriate for the nutritional risk screening of the patients after HSCT.But we should notice that there were 63.6%of patients after HSCT having 6 score which meant that although NRS2002 could not distinguish nutritional risk status of patients after HSCT well, the nutritional risk of patients after HSCT was higher than before, and a more accurate method was needed for assessment and distinguishing.
There were 77 cases (77.8%) with weight loss after HSCT, of which 49 (63.6%) had weight loss more than 5%in one month.Weight change during the transplantation can indirectly reflect the changes of patient's condition and heat supply.Excessive weight loss will seriously affect various systems of patients, resulting in a decline in disease resistance, even the success of the transplantation (19).It was reported that the measurement of body weight could be useful for the nutritional assessment (20), and underweight might reduce the ability to mobilize peripheral blood stem cells which is associated with a poorer outcome after HSCT (21).It was also reported that body weight loss >10% of the initial value within a week is an indication to start nutritional support with total parenteral nutrition(TPN) (22).Therefore, for the nutritional risk screening and assessment of patients after HSCT, body weight is an important indicator.
In conclusion, leukemia patients should receive the nutritional risk screening conventionally before and after HSCT.NRS2002 is appropriate for nutritional risk screening before HSCT.At the same time, more attention should be paid to the patients less than 30 years old or not-full matched.But the methods of nutritional risk screening and assessment for patients after HSCT remain to be further explored.Moreover, it should be noticed that the weight loss is an important problem for patients after HSCT, and is one of the innegligible indicators of nutritional risk screening and assessment.Ensuring relatively stable weight would have a positive effect for the patients to overcome the stress response and improve the prognosis.
Acknowledgements
Disclosure:The authors declare no conflict of interest.
1.Rzepecki P, Barzal J, Sarosiek T, et al.Biochemical indices for the assessment of nutritional status during hematopoietic stem cell transplantation: are they worth using? A single center experience.Bone Marrow Transplant 2007;40:567-72.
2.Huang XJ.Hematopoietic stem cell transplantation in China: current status and prospects.Am J Blood Res 2011;1:90-7.
3.Turedi A, Demir C, Dilek I.Assessment of malnutrition in adult acute leukemia cases.Asian Pac J Cancer Prev 2010;11:703-7.
4.Arfons LM, Lazarus HM.Total parenteral nutrition and hematopoietic stem cell transplantation: an expensive placebo? Bone Marrow Transplant 2005;36:281-8.
5.Bechard LJ, Feldman HA, Gordon C, et al.A multi-center,randomized, controlled trial of parenteral nutrition titrated to resting energy expenditure in children undergoing hematopoietic stem cell transplantation (“PNTREE”):rationale and design.Contemp Clin Trials 2010;31:157-64.
6.Lobato-Mendizábal E, Ruiz-Argüelles GJ, Marín-López A.Leukaemia and nutrition.I: Malnutrition is an adverse prognostic factor in the outcome of treatment of patients with standard-risk acute lymphoblastic leukaemia.Leuk Res 1989;13:899-906.
7.Arnaud-Battandier F, Malvy D, Jeandel C, et al.Use of oral supplements in malnourished elderly patients living in the community: a pharmaco-economic study.Clin Nutr 2004;23:1096-103.
8.Raja R, Lim AV, Lim YP, et al.Malnutrition screening in hospitalised patients and its implication on reimbursement.Intern Med J 2004;34:176-81.
9.Fine JT, Colditz GA, Coakley EH, et al.A prospective study of weight change and health-related quality of life in women.JAMA 1999;282:2136-42.
10.Martin-Salces M, de Paz R, Canales MA, et al.Nutritional recommendations in hematopoietic stem cell transplantation.Nutrition 2008;24:769-75.
11.Jones L, Watling RM, Wilkins S, et al.Nutritional support in children and young people with cancer undergoing chemotherapy.Cochrane Database Syst Rev 2010;7:CD003298.
12.Kondrup J, Rasmussen HH, Hamberg O, et al.Nutritional risk screening (NRS 2002): a new method based on an analysis of controlled clinical trials.Clin Nutr 2003;22:321-36.
13.Jiang ZM, Chen W, Zhan WH, et al.Parenteral and enteral nutrition application in west, middle and east China: a multi-center investigation for 15098 patients in 13 metropolitans using Nutritional Risk Screening 2002 tool (abstract).Clin Nutr 2007;2:133-4.
14.Kondrup J, Allison SP, Elia M, et al.ESPEN guidelines for nutrition screening 2002.Clin Nutr 2003;22:415-21.
15.Chen W, Jiang ZM, Zhang YM, et al.A clinical feasibility study in hospitalized patients with european survey method for risk of malnutrition.Zhong Hua Lin Chuang Ying Yang Za Zhi (in Chinese) 2005;13:137-41.
16.Chen CM.Chinese adult body mass index classification recommendation profile.Chin J Pre Med (Chin)2001;35:349-350.
17.Liu P, Yan X, Wang BS, et al.Three methods assess nutritional status of leukemia patients before hematopoietic stem cell transplantation.Chin Med J(Engl) 2012;125:440-3.
18.Hadjibabaie M, Iravani M, Taghizadeh M, et al.Evaluation of nutritional status in patients undergoing hematopoietic SCT.Bone Marrow Transplant 2008;42:469-73.
19.Ji YY, Ji SQ, Ju XS.Parenteral nutrition in bone marrow transplantation.Chang Wai Yu Chang Nei Ying Yang (in Chinese) 1995;2:119-21.
20.Rzepecki R, Barzal J, Sarosiek T, et al.Nutritional assessment during allogeneic hematopoietic stem cell transplantation: single centre experience.J BUON 2007;12:253-9.
21.Crowther M, Avenell A, Culligan DJ.Being underweight may reduce your ability to mobilise peripheral blood stem cells.Transfus Apher Sci 2010;43:365-7.
22.Rzepecki P, Barzal J, Sarosiek T, et al.Which parameters of nutritional status should we choose for nutritional assessment during hematopoietic stem cell transplantation?Transplant Proc 2007;39:2902-4.
 Chinese Journal of Cancer Research2012年4期
Chinese Journal of Cancer Research2012年4期
- Chinese Journal of Cancer Research的其它文章
- Combination chemotherapy with paclitaxel, cisplatin and fluorouracil for patients with advanced and metastatic gastric or esophagogastric junction adenocarcinoma: a multicenter prospective study
- Activation of sonic hedgehog signaling pathway is an independent potential prognosis predictor in human hepatocellular carcinoma patients
- High-risk endometrial cancer may be benefit from adjuvant radiotherapy plus chemotherapy
- Circulating tumor cells (CTCs) in breast cancer: a diagnostic tool for prognosis and molecular analysis
- Evaluation of treatment response for breast cancer: are we entering the era of “biological complete remission”?
- Perivascular epithelioid cell tumor of male pelvic cavity: a case report and literature review