視神經管和頸內動脈與鞍區結構位置關系的CT研究
2013-11-02 03:44:08燕程也張斯文
中國民族民間醫藥 2013年11期
關鍵詞:測量
彭 燕程 也張斯文
1.長春大學校醫院醫技科,吉林 長春 130022;2.吉林大學白求恩醫學院;吉林 長春 130022
視神經管和頸內動脈與鞍區結構位置關系的CT研究
彭 燕1程 也2張斯文2
1.長春大學校醫院醫技科,吉林 長春 130022;2.吉林大學白求恩醫學院;吉林 長春 130022
目的:通過CT對視神經管和頸內動脈在鞍區的位置進行研究并為神經外科醫生進行經鼻蝶的鞍區手術提供指導。方法:觀察并測量120個成人顱腦CT圖像,并通過多平面重建技術進行冠狀面、矢狀面和軸面的測量。結果:①視神經管內側壁與經鞍底正中矢狀線的距離為平面1處:13.66±0.84mm,平面2處:11.14±0.98mm,平面3處:7.99±1.02mm;②BO與BM1的夾角為平面1處:89.61±6.38°,平面2處:82.34±7.45°,平面3處:83.99±5.90°;③頸內動脈內側壁與經鞍底正中矢狀線的距離為在平面4處:10.23±2.26mm,平面5處:8.82±3.15mm,平面6處:8.85±1.58mm;④BA2與BM2的夾角為74.99±5.21°;BA1與BM1的夾角為97.12±12.05°;⑤視神經管與水平線的夾角為10.14±4.99°。結論:視神經管、頸內動脈在鞍區的位置的測量,可為二者的位置的解剖學研究和內窺鏡下經鼻蝶進行鞍底的手術提供指導。
頸內動脈;視神經管;蝶竇;鞍區;經鼻蝶手術
視神經管和頸內動脈與鞍區結構關系 (如蝶竇、鞍底)比較復雜,視神經管位于視神經管內而頸內動脈位于海綿竇內,稱為頸內動脈海綿竇段(cavernous segment of the internal carotid artery,CSICA)[1-2]。視神經管和頸內動脈都可以突入蝶竇并且在蝶竇腔內形成隆突[3-4]。因此它們在頸內動脈瘤切除、垂體瘤切除等經蝶竇的手術中需要被特殊保護[5]。如果打開蝶竇側壁時未進行限制會造成視神經和頸內動脈的損傷[6],因此,對視神經管和頸內動脈進行準確的定位十分重要。已有很多文獻報道以視神經隆突和頸內動脈隆突作為蝶竇側壁開口的標志,但這些隆突在不同人所形成的程度不同,并由很大一部分缺如的情況,因次,CT的測量提供相應的數據是必要的。
1 材料和方法
觀測120例健康成年人的蝶竇CTA影像,男69例,女51例,所選取的成年人樣本年齡為19~76歲(平均48.3歲),圖像不含蝶竇畸形,垂體腺瘤、頸內動脈畸形的患者。測量地點為吉林大學中日聯誼醫院,儀器為東芝320排容積CT(片層0.5mm)。所有圖像進行多平面重建(multiplanar reconstruction,MPR)。
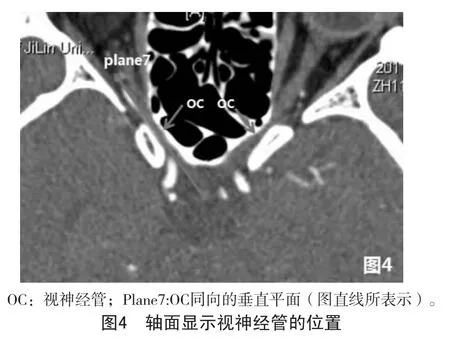
測量平面的選擇:選取6個冠狀平面 (圖1)和一個垂直平面 (圖4),各個平面的位置見表1,選取的測量線段的位置見表2。
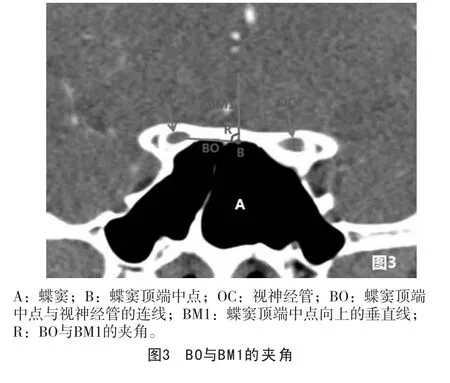
①在平面1、2、3測量OC內側壁與經鞍底正中矢狀線的距離以及線BO和BM1之間的夾角(圖2,圖3);
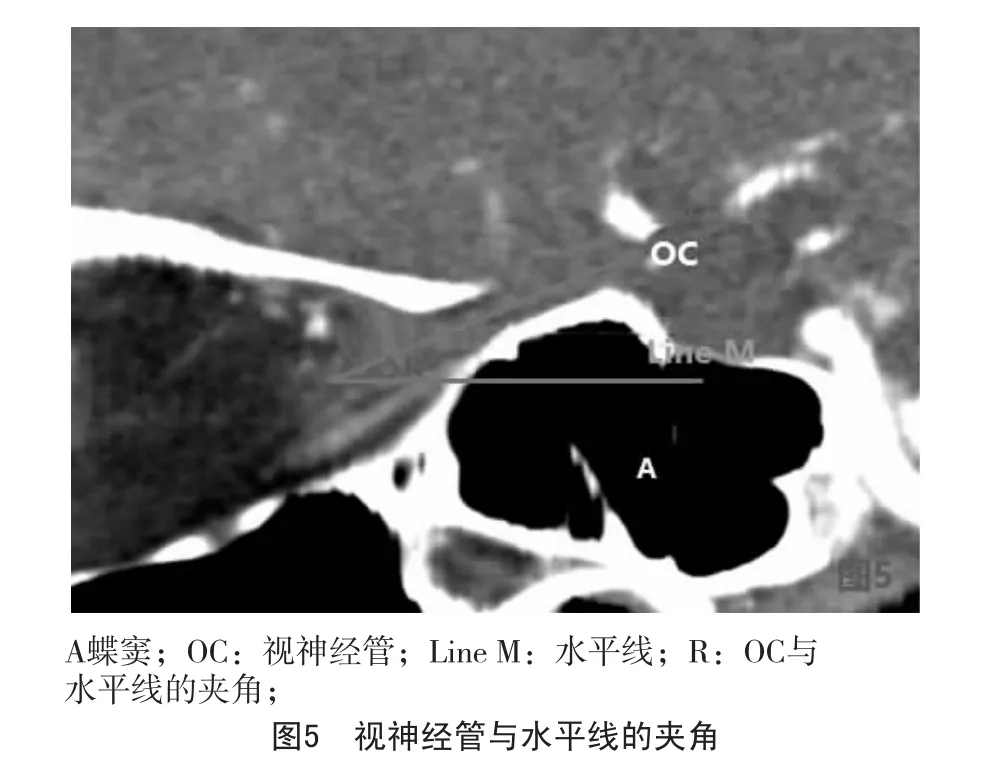
②在平面7測量OC和水平線的夾角(圖5);
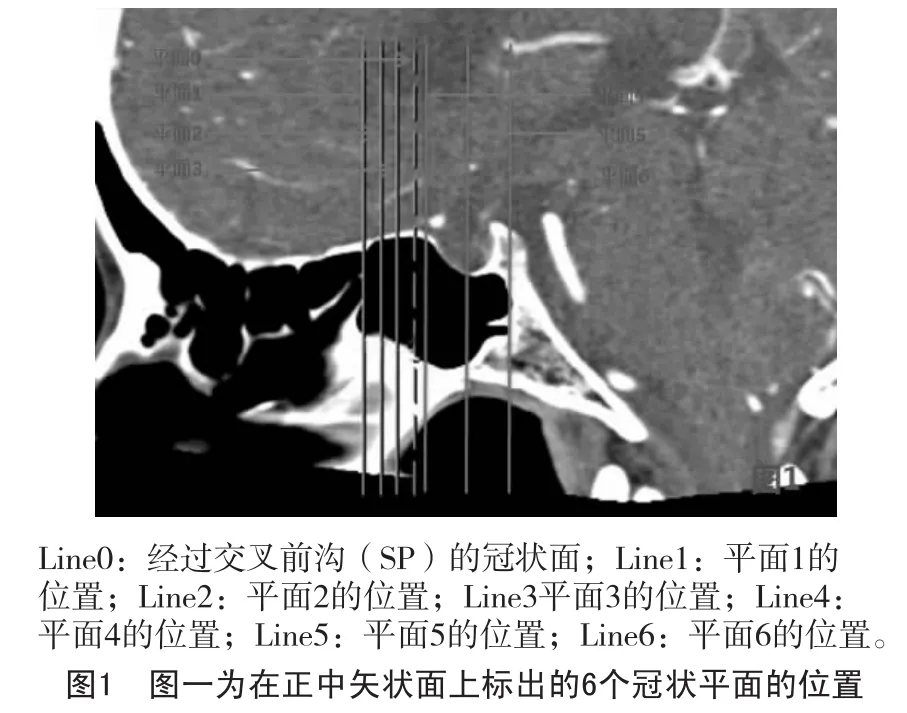
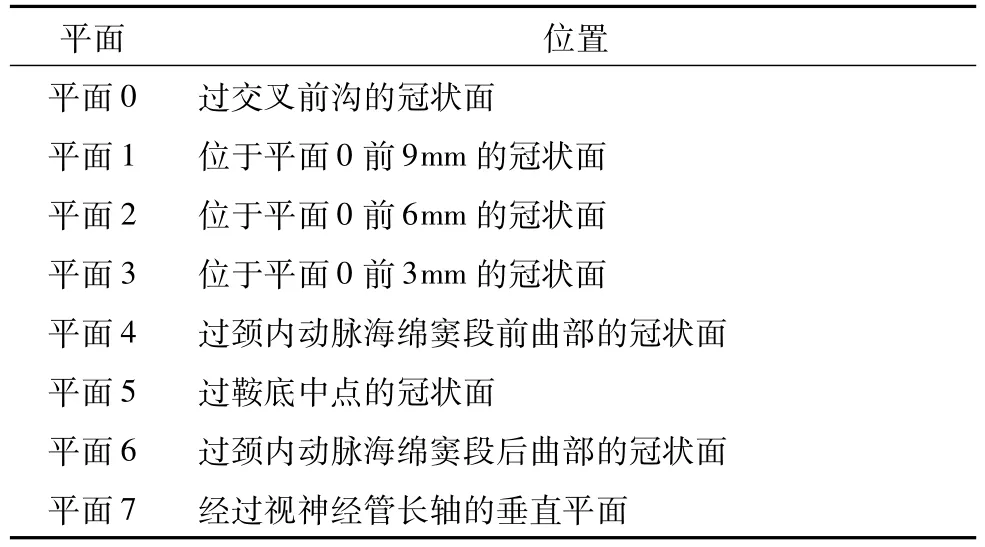
表1 測量平面

表2 測量所用輔助線與測量距離

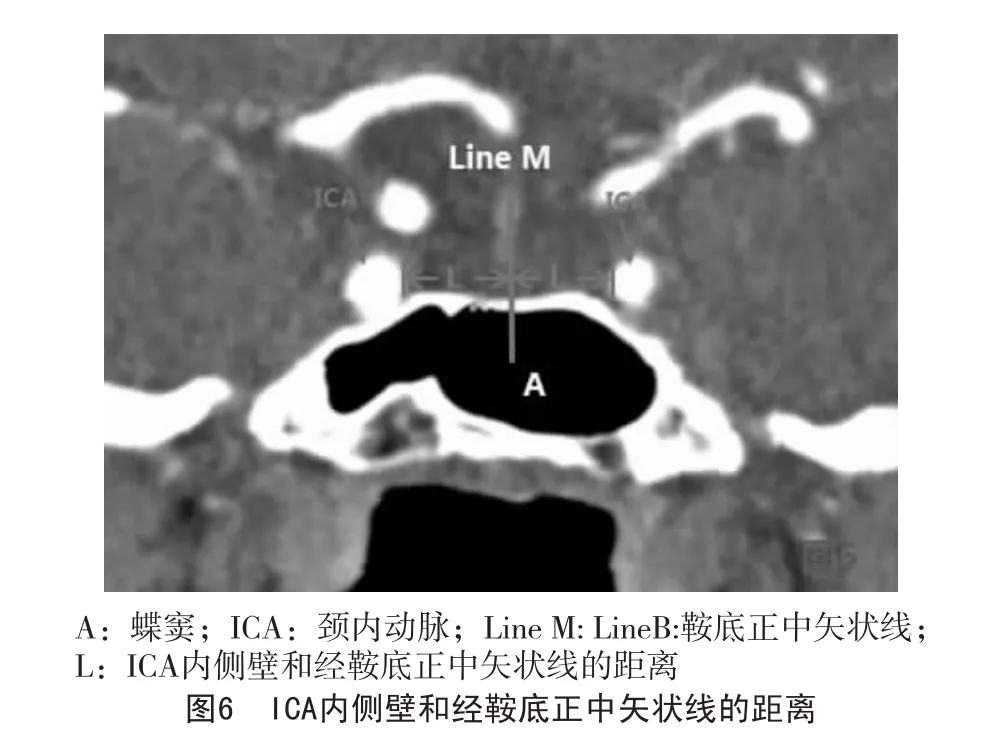

③在平面4、5、6測量ICA內側壁和經鞍底正中矢狀線的距離(圖6),在平面5測量BA2和BM2的距離;
④在平面4進行線BA1與線BM1夾角的測量(圖7)
統計結果采用SPSS15.0軟件進行統計。
2 結果
在CTA上可以在冠狀面、矢狀面和軸面清楚看到OC和ICA的位置及走形。OC在冠狀面上類似“蝶眼狀”在矢狀面上類似 “軌道狀”。視神經管呈相對低密度兒頸內動脈呈相對高密度。測量結果表明視神經管和境內動脈都有很好的對稱性。
2.1 視神經管與鞍區結構的關系
OC內側壁與鞍底正中矢狀線的距離見表3。
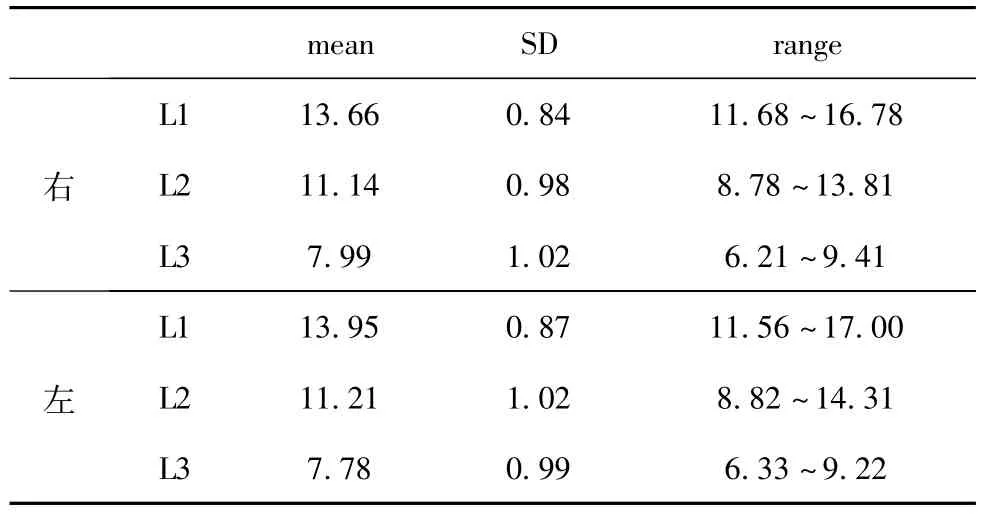
表3 OC內側壁與鞍底正中矢狀線的距離(mm)
經統計學ANOVA分析,在L1、L2和L3之間存在顯著差異。經Student-t檢驗,L1與L2之間以及L2與L3之間存在顯著差異。且男女之間無顯著差異(P>0.05)。BO與BM1的夾角見表4。統計結果t檢驗表明R1與R2間無顯著差異,但R3與R1之間以及R3與R2之間存在顯著差異,表明R3與R1和R2存在差異,且數據顯示R3更接近90°,因此視神經管在平面3位置與蝶竇上緣幾乎平齊。

表4 BO與BM1的夾角
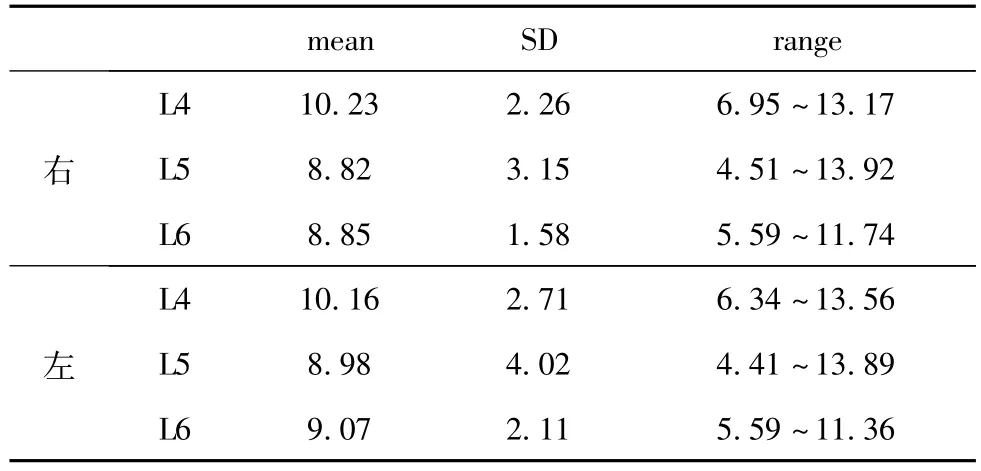
表5 頸內動脈與鞍底正中矢狀線的距離 (mm)
視神經管與水平線的夾角為右側10.14±4.99°;左側9.99±5.03°
2.2 頸內動脈與鞍區結構的關系 頸內動脈與鞍底正中矢狀線的距離見表5,結果在平面4相對較大在平面6相對較小,與WEI[7]以及XUE[8]的結果一致。線BA2與BM2的夾角為右側74.99±5.21°,左側76.02±5.98°;線BA1與BM1的夾角為右側97.12±12.05°,左側98.00±11.02°。
3 討論
隨著內窺鏡技術的發展,內鏡下經鼻蝶手術可以在較小創傷的情況下進行垂體瘤頸內動脈瘤的手術,而較小的創傷意味著更小的手術成本,更短的恢復時間,更容易控制的手術并發癥而達到更好的外科治療效果[6,9-11]。對于腫瘤的切除來說,完整地暴露病灶是安全手術的保障[12],而對于經蝶入路來說,對蝶骨側壁的破壞增加了損傷視神經管和頸內動脈的危險性,而OC與ICA形態的多樣性意義蝶竇氣化的程度差異也增加了OC和ICA損傷的危險性[13]。雖然視神經隆突和頸內動脈隆突可作為手術的重要標志,但它們在很大一部分人中會缺如[3],從而又增加了手術的難度。因此尋找視神經管和頸內動脈和鞍區其它固定結構的位置關系變得更加重要。
3.1 OC的位置以及和鞍區結構的關系 視神經損傷依然是經蝶手術的主要并發癥之一。視神經隆突被確定為是進行蝶竇開窗的最外界限,但除了視神經隆突缺如的可能性外 (86.6%可見[14]),視神經的近側段和遠側段也無法形成隆突。因此CT的測量可在無法參考視神經隆突的情況下提供幫助。
同時,結節隱窩(Tubercular recess,TR)是視神經管的起始部位也是視神經進入視神經管的部位[3],TR唯一交叉前溝的正下方,平面1、平面2、平面3的位置可以根據TR的位置而確定。而對OC的測量結果提示:為了避免對視神經的損傷,在TR前3mm處,開窗的寬度應該小于7.80±1.23mm(右側),7.92±1.14mm(左側);在TR前6mm處,開窗的寬度應該小于11.35±1.08mm(右側)11.09±1.12mm(左側);在TR前9mm處,開窗的寬度應該小于13.97±0.78mm(右側)14.01±0.87(左側)。
由于蝶竇的頂端很容易確定,因此線BO與BM1的角度可以通過蝶竇頂端尋找OC的位置。
3.2 ICA的位置以及和鞍區結構的關系 當頸內動脈隆突缺如時,鞍底正中點,蝶竇頂端可以作為尋找頸內動脈的標志。由于雙側頸內動脈的高度有時不一致,因此在冠狀面上進行頸內動脈內側壁距離鞍底中線距離的測量優與軸面 (圖6)。頸內動脈內側壁與鞍底正中矢狀線之間的距離可以視為蝶竇側壁開窗的最大距離。因此,在頸內動脈前曲部,開窗的寬度應該小于10.23±2.26mm(右側),10.12±2.21mm(左側);在鞍底中點,開窗寬度應該小于8.82±1.15mm(右側),8.76±1.23mm(左側);在頸內動脈后曲部,開窗寬度應該小于8.85±1.58mm(右側),8.45±1.61mm(左側)。
鞍底最中點也是垂體窩的最低點,它已經被研究和定位[15]。根據線BA2和BM2的夾角和鞍底最低點的位置可以確定ICA的位置。同時,在頸內動脈的前曲段,根據線BA1和BM1的夾角以及蝶竇頂部中點可以確定頸內動脈的位置。
4 結論
由于OC和ICA在CTA上較易發現,因此我們可以根據影像學的定位進行術前定位。同時,精確的數據測量也是必不可少的。研究表明,OC和ICA與鞍區結構之間有一定的關系,因此OC和ICA的位置可以根據這些結果進行確定。
[1]Bouthillier A,van Loveren HR,Keller JT:Segments of the internal carotid artery:a new classification.Neurosurgery,1996,38:425-33.
[2]Fischer E.Die lageabweichungen der vorderen hirnarterie imgefaβblid[J].Zentralbl Neurochir,1938,3:300-313.
[3]Yilmazlar S,Saraydaroglu O,Korfali E.Anatomical aspects in the transsphenoidal-transethmoidal approach to the optic canal:An anatomic-cadaveric study.JCraniomaxillofac Surg.2012,40:198-205.
[4]ZHU Xi-wen,SUN Jia-qi,LIYue-feng:The correlation between the volume of the sphenoid and the bulge of the internal carotid artery in the sphenoid:CT study.Chinese journal of clinical anatomy,2010,28:551-553.
[5]Cavallo LM,Messina A,Cappabianca P,Esposito F,de Divitiis E,Gardner P,et al:Endoscopic endonasal surgery of themidline skull base:anatomical study and clinical considerations.Neurosurg Focus,2005,19(1):E2.
[6]Ossama Al-Mefty,Svetlana Pravdenkova,Cristian Gragnaniello:A technical note on endonasal combined microscopic endoscopic with free head navigation technique of removal of pituitary adenomas.Neurosurg Rev2010,33:243-249.
[7]WEIYukui,KANG Jun,WANG Renzhi:Microscopic and endoscopic anatomy of the cavernous segment of the internal carotid artery.CMINSJ,2008,13:64-67.
[8]XUE Liang,JING Jun-Jie:Microscopic anatomy of cavernous segmentof internal carotid artery via extended transnasal approach.J Fourth M il M ed Univ,2009,30:229-231.
[9]Berker M,Hazer DB,Yücel T,Gürlek A,Cila A,Aldur M,Onerci M:Complications of endoscopic surgery of the pituitary adenomas:analysis of 570 patients and review of the literature.Pituitary.2012;15(3):288-300.
[10]Raithatha R,McCoul ED,Woodworth GF,Schwartz TH,Anand VK:Endoscopic endonasal approaches to the cavernous sinus.Int Forum Allergy Rhinol,2012,2:9-15.
[11]Chamoun R,CouldwellWT:Practical and technical aspects of trans-sphenoidal surgery.JNeurosurg Sci,2011,55:265-75.
[12]Yazhuo Zhang,Zhongcheng Wang,Yejian Liu,Xuyi Zong,Ming Song,Ao Pei,Peng Zhao,Pengfei Zhang and Mingxue Piao:Endoscopic transsphenoidal treatment of pituitary adenomas.Neurological Research,2008,30:581-586.
[13]LocatelliM,Bertani G,Carrabba G,Rampini P,Zavanone M,Caroli M,Sala E,Ferrante E,Gaini SM,Spada A,Mantovani G,Lania A:The transsphenoidal resection of pituitary adenomas in elderly patients and surgical risk.Pituitary 2012 Apr 10.[Epub ahead of print].
[14]Cappabianca P,Cavallo LM,Esposito F,De Divitiis O,Messina A,De Divitiis E:Extended endoscopic endonasal approach to themidline skull base:the evolving role of transsphenoidal surgery.Adv Tech Stand Neurosurg,2008,33:151.
[15]Nikolaos Lazaridis,Konstantinos Natsis,Juergen Koebke et al:Nasal,Sellar,and Sphenoid Sinus Measurements in Relation to Pituitary Surgery.Clinical Anatomy,2010,23:629-636.
The position of optic canal and internal carotid artery in sella region:CT study
Yan Peng1,Ye Cheng2,Siwen Zhang2
1.Changchun University Hospital,Medical department;2.Norman Bethune Medical School of Jilin University
Background:The position of Optic canal(OC)and internal carotid artery(ICA)are relatively complex in sella region,they can be injured in the transsphenoidal surgery and result in severe complications such as haemorrhage and optic nerve damage.Purpose:the aim of our study is to provide new specific and comprehensive data about the location of OC and ICA in sella region in order to guide surgeons through the difficulties in the approaches.Material and method:Computer topographic angiography(CTA)images of 120 sphenoid sinuses in adultswere reviewed.Themeasurementwas on coronal,sagittal and axis planes aftermultiplanar reconstruction(MPR).We selected 6 coronal planes(plane1 to plane6)tomake themeasurement.Results:The distance between themedial wall of OC and the sagittalmidline of sella bottom were 13.66±0.84mm in plane1,11.14±0.98mm in plane2,7.99±1.02mm in plane3.The angle between line BO and BM1 were 89.6±6.38 degree in plane1,82.34±7.45 degree in plane2,83.99±5.90 degree in plane3.The distance between ICA and the sagittalmidline of sella bottom were 10.23±2.26mm in plane4,8.82±1.15mm in plane5,8.85±1.58mm in plane6.The angle between line BA2 and BM2 was74.99±5.21 degree;the angle between line BA1 and BM1 was 97.12±12.05 degree.The angle between OC and the horizontal line was 97.12±12.05 degree.Conclusion:After finding the relationships among OC,ICA and the structures in sella region,we can have amore comprehensive anatomical understanding of them as well as the clinical importance of the location of them.
ICA;OC;Sphenoid sinus;Sella region;Transsphenoidal approach
R651.1
A
1007-8517(2013)11-0060-04
2013.03.19)
猜你喜歡
小學科學(學生版)(2021年5期)2021-07-22 02:40:06
中學生數理化·八年級物理人教版(2019年9期)2019-11-25 07:33:02
中學生數理化·八年級物理人教版(2019年3期)2019-04-25 06:20:54
中學生數理化·八年級物理人教版(2018年3期)2018-05-31 08:52:45
數學小靈通(1-2年級)(2017年10期)2017-11-08 08:39:45
軍事文摘·科學少年(2017年4期)2017-06-20 23:25:16
軍事文摘·科學少年(2017年2期)2017-04-26 21:58:43
中學生數理化·八年級物理人教版(2016年3期)2016-04-07 04:49:32
少兒科學周刊·兒童版(2016年1期)2016-03-14 03:52:21
閱讀與作文(小學低年級版)(2015年4期)2015-04-29 00:00:00