人類白細胞抗原G在宮頸癌組織中的表達及臨床意義
2014-04-21 00:45:32王元芬牛子儒郭一帆劉忠宇姚元慶
解放軍醫學院學報 2014年7期
關鍵詞:檢測
王元芬,牛子儒,郭一帆,谷 芳,劉忠宇,姚元慶
解放軍總醫院 婦產科,北京 100853
人類白細胞抗原G在宮頸癌組織中的表達及臨床意義
王元芬,牛子儒,郭一帆,谷 芳,劉忠宇,姚元慶
解放軍總醫院 婦產科,北京 100853
目的 探討人類白細胞抗原G(human leukocyte antigen G,HLA-G)在宮頸癌組織中的表達及其臨床意義。方法應用S-P免疫組織化學方法檢測于2006年1月- 2011年12月就診我院的98例宮頸鱗癌患者術后病理標本,并分析HLA-G的表達與病理參數之間的關系。結果HLA-G分子在宮頸癌組織中表達率為43.9%(43/98),而在癌旁正常宮頸組織的表達率為0。HLA-G分子表達與淋巴結轉移、脈管浸潤有相關性(P<0.01)。結論HLA-G分子在宮頸癌組織中表達上調,并與宮頸癌的侵襲性生長相關。HLA-G分子參與腫瘤細胞免疫逃逸過程,促進腫瘤的發生和發展。
宮頸癌;人類白細胞抗原G;免疫組織化學
腫瘤微環境中有多種分子參與腫瘤細胞免疫逃逸過程,例如血管內皮生長因子(vascular endothelial growth factor,VEGF)、白細胞介素-10(interleukin-10,IL-10)、轉化生長因子-P(transforming growth factor-p,TGF-p)、前列腺素等[1]。近年來,人白細胞抗原G(human leukocyte antigen G,HLA-G)逐漸成為腫瘤免疫逃逸的研究熱點。HLA-G最早發現其特異性表達于母胎界面絨毛膜外滋養層細胞,在妊娠過程中,阻止母體對同種半異體的胎兒進行免疫排斥反應,維持妊娠。近年來多項研究發現,HLA-G分子亦表達于黑色素瘤、乳腺癌、肺癌等30余種腫瘤細胞表面,提示HLA-G分子可能在腫瘤細胞的免疫逃逸中發揮重要作用[2-7]。然而,HLA-G分子在宮頸癌組織中的表達尚不十分清楚。本研究旨在分析HLA-G分子在宮頸癌組織中的表達與病理參數之間的關系。
材料和方法
1 病例及標本來源 98例組織標本均為2006年1月- 2011年12月就診于本院并行宮頸癌根治術患者,根據2009年國際婦產科協會(Federation International of Gynecology and Obstetrics,FIGO)指南均診斷為ⅠB ~ ⅡA期,術前未行放、化療。宮頸癌組織蠟塊經病理學證實組織類型為宮頸鱗癌。同時取20例宮頸癌旁3 ~ 5 cm宮頸組織,經病理學證實無癌細胞浸潤。HLA-G表達陽性對照標本取自解放軍總醫院計劃生育門診3例孕婦(孕8 ~ 12周)行人流術后絨毛組織,石蠟包埋成組織蠟塊。
2 試劑 鼠抗人HLA-G單抗,購自LifeSpan BioScience公司。即用型小鼠SP-9002檢測試劑盒購自北京中杉金橋生物技術有限公司。
3 免疫組織化學S-P法檢測HLA-G表達 切片脫蠟,二甲苯(Ⅰ)10 min→二甲苯(Ⅱ)10 min→100%乙醇2 min→95%乙醇2 min→80%乙醇2 min→蒸餾水浸洗2次,將切片放置高壓鍋中。抗原修復:加熱蒸餾水至270℃煮沸,切片置于高壓鍋中,待安全閥門抬起后,蓋上散氣閥,待散氣閥轉動后,降至100℃ 2.5 min,關閉電源,置于冷水中,冷卻15 min。蒸餾水浸洗切片2次。消除內源性過氧化物酶:切片置于30% H2O2浸泡15 min,蒸餾水充分浸洗3次。PBS浸洗3次,每次5 min。滴加鼠抗人HLA-G蛋白單克隆抗體(工作濃度:1∶750),4℃過夜。PBS浸洗3次,每次5 min,滴加生物素標記的二抗,37℃孵育20 min,PBS浸洗3次,每次5 min。DAB顯色,自來水充分沖洗,蘇木素染液,沖冼,水溶性樹脂膠進行封片。
4 實驗結果判定 將癌細胞膜或細胞質內出現棕黃色顯色定為陽性表達,每張切片由兩名經驗豐富的病理醫師分別判定。
5 統計學處理 應用SPSS19.0軟件進行處理。計數資料用χ2檢驗,P<0.05為差異有統計學意義。
結 果
1 HLA-G在組織中的表達 在98例宮頸癌組織中,43例HLA-G分子表達陽性,表達率為43.9% (43/98),主要定位于細胞質或細胞膜上。而在20例癌旁正常宮頸組織中無HLA-G分子的表達。見圖1 ~圖4。
2 HLA-G分子表達與病理參數之間的關系 98例宮頸癌組織中,HLA-G分子陽性表達率與分化、宮頸肌層浸潤無關(P>0.05),與淋巴結轉移、脈管浸潤相關(P<0.01)。見表1。
討 論
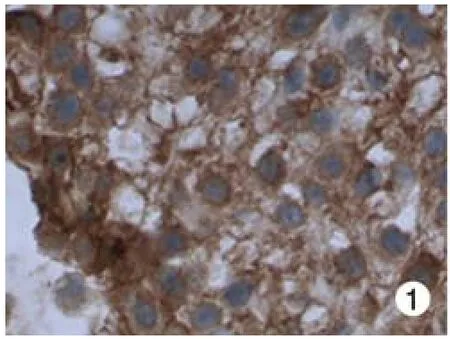
圖 1 HLA-G在絨毛膜組織的表達(×200,陽性對照)Fig. 1 Expression of HLA-G in chorionic tissues(×200, positive control group)
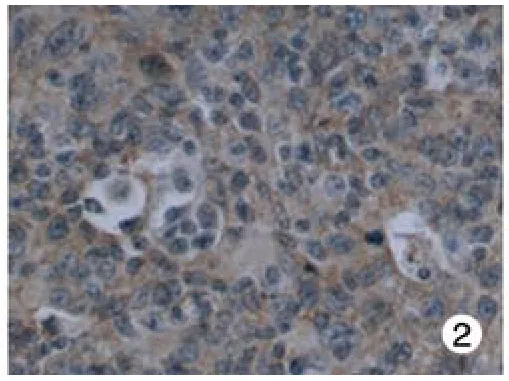
圖 2 宮頸癌組織中陽性表達(×200)Fig. 2 Positive expression in cervical cancer(×200)
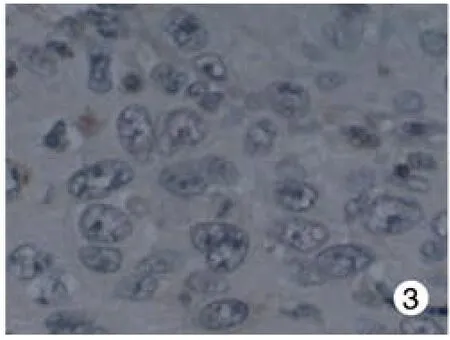
圖 3 宮頸癌組織中陰性表達(×200)Fig. 3 Negative expression in cervical cancer(×200)
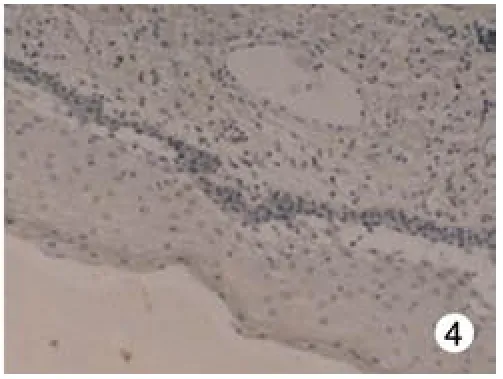
圖 4 正常宮頸組織無表達(×100)Fig. 4 No expression in normal cervical tissues(×100)
多項研究證實某些腫瘤細胞表達HLA-G分子,通過與免疫細胞表面的抑制性受體結合,抑制宿主免疫功能,這可能成為腫瘤免疫逃逸機制之一[8]。目前已發現3種可結合HLA-G分子的殺傷細胞免疫球蛋白樣受體(killer cell immunoglobulin-like receptor,KIR):免疫球蛋白樣轉錄體2(immunoglobulin-like transcripts ILT2/CD85j/leukocyte immunoglobulin-like receptors LILRB1)、免疫球蛋白樣轉錄體4(ILT4/CD58d/LILRB2)及殺傷細胞抑制性受體(KIR2DL4/CD158d)。這3種受體特異性表達于T淋巴細胞(ILT2)、NK細胞(KIR2DL4和ILT2)、單核細胞、巨噬細胞及抗原提呈細胞(ILT2和ILT4)[9]。HLA-G分子的免疫抑制功能主要有:1)通過Fas/ FasL信號通路,誘導CD8+T細胞及CD8+NK細胞凋亡;2)抑制細胞毒性T細胞及CD8+NK細胞的細胞溶解作用;3)抑制CD4+T細胞增殖以及幼稚CD4+T細胞活化;4)HLA-G分子促使T細胞轉化為調節性T細胞(regulatory T cell,Treg cell),在腫瘤中Treg細胞通過細胞間接觸或分泌可溶性細胞因子(IL-10、TGF-β等)的途徑,抑制腫瘤特異性CD8+CTL和CD4+T細胞的免疫活性,抑制NK細胞的殺傷作用,從而抑制機體免疫功能[10-13]。
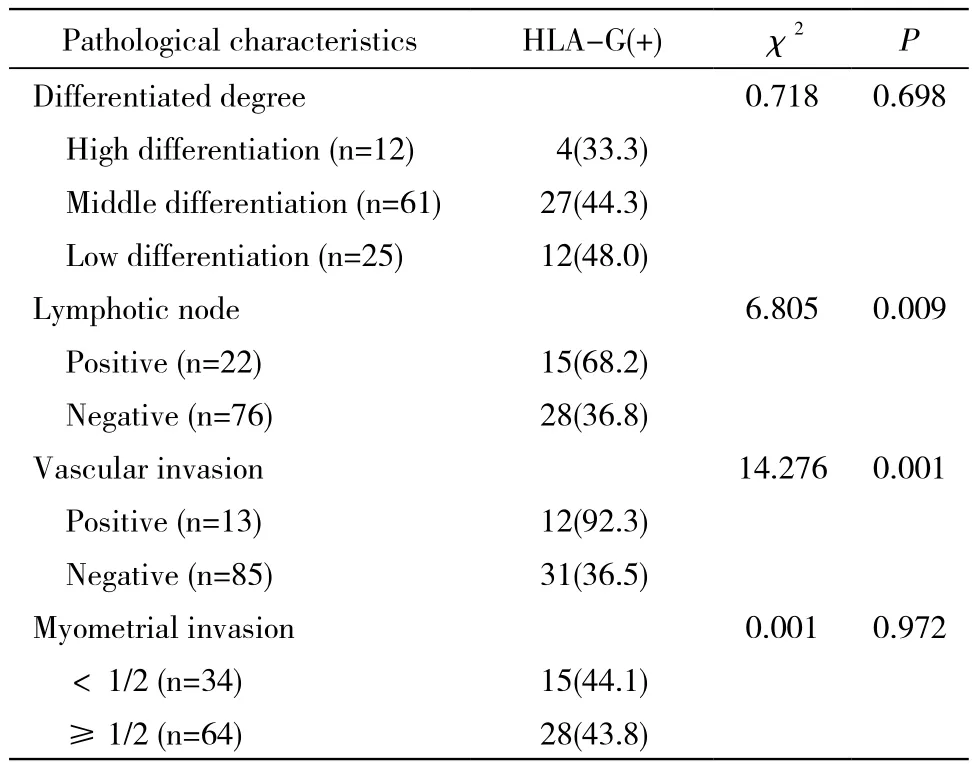
表1 HLA-G分子表達與病理參數的關系Tab. 1 Relationship between HLA-G and clinicopathological characteristics (n, %)
生理狀態下,HLA-G分子表達分布具有組織特異性。最早發現HLA-G表達于母胎界面絨毛膜外滋養層細胞,參與母胎界面的免疫耐受過程,抑制母體對同種半異體的胎兒進行免疫排斥反應,維持妊娠[14]。運用RNA印記及RT-PCR證實:HLA-G mRNA廣泛存在于成人組織細胞,如皮膚、脾、胸腺等。然而與經典MHC-Ⅰ類分子相比,在多數組織中檢測到的HLA-G mRNA數量極少[15]。
1998年,Paul等[16]首次報道惡性黑色素瘤細胞系表達HLA-G分子。并且,在對黑色素瘤患者活檢組織的研究中,在原發瘤及轉移瘤組織中檢測到HLA-G mRNA的轉錄水平和HLA-G分子表達增高,而癌旁正常皮膚組織及腫瘤壞死部位HLA-G mRNA的水平很低,且未檢測到HLA-G蛋白表達。Elliott等[17]的研究中運用RT-PCR方法檢測正常乳腺上皮細胞系及乳腺癌細胞系HLA-G mRNA轉錄水平,結果正常乳腺上皮細胞系未檢測到HLA-G mRNA,而在不同的乳腺癌細胞系中HLA-G mRNA轉錄水平不同。Yie等[18-19]研究中發現90.9%(110/121)食管鱗癌、71%(113/160)胃癌原發部位有HLA-G分子的表達,而在正常組織中HLA-G表達陰性。Jung等[20]研究發現卵巢癌患者中HLA-G mRNA和蛋白表達水平顯著高于正常卵巢組織。
本次試驗結果證實,在宮頸癌組織中HLA-G分子的陽性表達率為43.9%,而癌旁正常宮頸組織中未發現HLA-G分子的表達。這與之前在其他腫瘤中發現的結論一致。HLA-G分子與宮頸癌病理參數關系研究發現,HLA-G分子的表達與淋巴結轉移、脈管浸潤相關,這可能成為宮頸癌轉移的一個前期信號,同時進一步支持HLA-G分子免疫抑制,促進腫瘤發生、發展的結論。而鄭妮等[21]研究中顯示,HLA-G在宮頸癌中的表達與腫瘤分化相關,與淋巴結轉移相關性無統計學意義。對比兩個實驗研究,結果不同可能是因為病例選擇及例數不同,鄭妮等試驗中選擇54例宮頸鱗癌及腺癌,臨床分期為Ⅰ~Ⅳ期,而本實驗僅選擇了98例早期宮頸鱗癌,臨床分期為ⅠB ~ⅡA期。亦可能是不同實驗室所使用的單克隆抗體不同或敏感度不同。因此,需要更大標本量的試驗進一步研究HLA-G分子在宮頸癌中的表達、作用機制及臨床意義。
綜上所述,可通過檢測宮頸癌患者HLA-G分子的表達,評估患者的病情變化及預后。同時,HLA-G分子可作為免疫治療的靶點,研發針對HLA-G分子特異性的抗體,阻斷HLA-G分子與抑制性受體結合,從而恢復或增強機體抗腫瘤效應,改善患者預后及臨床結局。
1 Kim R, Emi M, Tanabe K, et al. Tumor-driven evolution of immunosuppressive networks during malignant progression[J]. Cancer Res, 2006, 66(11): 5527-5536.
2 Mach P, Blecharz P, Basta P, et al. Differences in the soluble HLA-G blood serum concentration levels in patients with ovarian cancer and ovarian and deep endometriosis[J]. Am J Reprod Immunol, 2010, 63(5):387-395.
3 Elliott RL, Jiang XP, Phillips JT, et al. Human leukocyte antigen G expression in breast Cancer: role in immunosuppression[J]. Cancer Biother Radiopharm, 2011, 26(2): 153-157.
4 Zhu CB, Wang CX, Zhang X, et al. Serum sHLA-G levels: a useful indicator in distinguishing colorectal Cancer from benign colorectal diseases[J]. Int J Cancer, 2011, 128(3): 617-622.
5 de Kruijf EM, Sajet A, van Nes JG, et al. HLA-E and HLA-G expression in classical HLA class I-negative tumors is of prognostic value for clinical outcome of early breast cancer patients[J]. J Immunol, 2010, 185(12):7452-7459.
6 Kren L, Valkovsky I, Dolezel J, et al. HLA-G and HLA-E specific mRNAs connote opposite prognostic significance in renal cell carcinoma[J]. Diagn Pathol, 2012, 7:58.
7 Lin A, Zhu CC, Chen HX, et al. Clinical relevance and functional implications for human leucocyte antigen-g expression in non-smallcell lung Cancer[J]. J Cell Mol Med, 2010, 14(9): 2318-2329.
8 Yan WH. Human leukocyte antigen-G in Cancer: are they clinically relevant?[J]. Cancer Lett, 2011, 311(2): 123-130.
9 Yan WH. HLA-G expression in cancers: potential role in diagnosis,prognosis and therapy[J]. Endocr Metab Immune Disord Drug Targets, 2011, 11(1): 76-89.
10 Contini P, Ghio M, Poggi A, et al. Soluble HLA-A,-B,-C and -G molecules induce apoptosis in T and NK CD8+ cells and inhibit cytotoxic T cell activity through CD8 ligation[J]. Eur J Immunol,2003, 33(1): 125-134.
11 Le Gal FA, Riteau B, Sedlik C, et al. HLA-G-mediated inhibition of antigen-specific cytotoxic T lymphocytes[J]. Int Immunol, 1999,11(8): 1351-1356.
12 Bainbridge DR1, Ellis SA, Sargent IL. HLA-G suppresses proliferation of CD4(+) T-lymphocytes[J]. J Reprod Immunol,2000 , 48(1):17-26.
13 Amiot L, Ferrone S, Grosse-Wilde H, et al. Biology of HLA-G in cancer: a candidate molecule for therapeutic intervention?[J]. Cell Mol Life Sci, 2011, 68(3):417-431.
14 侯彩英.可溶性人類白細胞抗原-G在子癇前期患者的表達和臨床意義[D]. 西安:第四軍醫大學,2008.
15 Gobin SJ, Biesta P, de Steenwinkel JE, et al. HLA-G transactivation by cAMP-response element-binding protein (CREB). An alternative transactivation pathway to the conserved major histocompatibility complex (MHC) class I regulatory routes[J]. J Biol Chem, 2002,277(42):39525-39531.
16 Paul P, Rouas-Freiss N, Khalil-Daher I, et al. HLA-G expression in melanoma: a way for tumor cells to escape from immunosurveillance[J]. Proc Natl Acad Sci U S A, 1998, 95(8):4510-4515.
17 Elliott RL, Jiang XP, Phillips JT, et al. Human leukocyte antigen G expression in breast cancer: role in immunosuppression[J]. Cancer Biother Radiopharm, 2011, 26(2):153-157.
18 Yie SM, Yang H, Ye SR, et al. Expression of HLA-G is associated with prognosis on esophageau squamous cell carcinoma[J]. Am J Clin Pathol, 2007, 128(6): 1002-1009.
19 Yie SM, Yang H, Ye SR, et al. Expression of human leukocyte antigen G (HLA-G) correlates with poor prognosis in gastric carcinoma[J]. Ann Surg Oncol, 2007, 14(10): 2721-2729.
20 Jung YW, Kim YT, Kim SW, et al. Correlation of human leukocyte antigen-G (HLA-G) expression and disease progression in epithelial ovarian Cancer[J]. Reprod Sci, 2009, 16(11): 1103-1111.
21 Zheng N, Wang CX, Zhang X, et al. Up-regulation of HLA-G expression in cervical premalignant and malignant lesions[J]. Tissue Antigens, 2011, 77(3):218-224.
Expression and clinical signifcance of human leukocyte antigen G in cervical cancer
WANG Yuan-fen, NIU Zi-ru, GUO Yi-fan, GU Fang, LIU Zhong-yu, YAO Yuan-qing
Department of Gynecology and Obstetrics, Chinese PLA General Hospital, Beijing 100853, China
YAO Yuan-qing. Email:yaoyq@126.com
ObjectiveTo investigate the expression of HLA-G molecule in cervical cancer and its clinical signifcance.MethodsPostoperative pathological samples of 98 patients with cervical cancer admitted to our hospital from January 2006 to December 2011 were detected by immunohistochemical method (S-P method), and the relationship between HLA-G and clinico-pathological characteristics in cervical cancer was analyzed.ResultsThe positive expression rate of HLA-G in cervical cancer was 43.9% (43/98),while no positive expression was found in normal tissues. The expression of HLA-G was correlated with lymphatic metastasis and vascular invasion (P<0.01).ConclusionExpression of HLA-G in cervical cancer tissues is signifcantly higher than that in normal tissues and it relates to the invasive growth of cervical cancer. It is also suggested that HLA-G molecule is closely related to immune evasion which will also promote the development of tumor.
cervical cancer; human leukocyte antigen G; immunohistochemical method
R 737.33
A
2095-5227(2014)07-0741-04
10.3969/j.issn.2095-5227.2014.07.026
時間:2014-04-18 17:38
http://www.cnki.net/kcms/detail/11.3275.R.20140418.1738.001.html
2014-04-02
北京市科技計劃項目(Z131100006813023)
Supported by Beijing Science and Technology Program(Z131100006813023)
王元芬,女,碩士。研究方向:婦科腫瘤。Email:wyf1988119@163.com
姚元慶,男,博士,主任醫師,教授。Email:yaoyq@126.com
猜你喜歡
中國設備工程(2022年12期)2022-07-11 04:33:00
中學生數理化·七年級數學人教版(2021年6期)2021-11-22 07:50:58
中學生數理化·七年級數學人教版(2021年6期)2021-11-22 07:50:58
中學生數理化·七年級數學人教版(2021年6期)2021-11-22 07:50:58
中學生數理化·七年級數學人教版(2020年12期)2021-01-18 06:57:46
中學生數理化·七年級數學人教版(2020年12期)2021-01-18 06:57:46
中學生數理化·七年級數學人教版(2019年9期)2019-11-25 07:34:36
中學生數理化·七年級數學人教版(2019年9期)2019-11-25 07:34:34
中學生數理化·七年級數學人教版(2019年12期)2019-05-21 02:53:50
中學生數理化·七年級數學人教版(2019年12期)2019-05-21 02:53:48