關節鏡下治療創傷復發性Bankart損傷療效分析
2014-07-05 15:29:02李彥林王國梁何川李建鄭家禮陳廣超李松余洋
中華肩肘外科電子雜志 2014年4期
關鍵詞:手術
李彥林 王國梁 何川 李建 鄭家禮 陳廣超 李松 余洋
·論著·
關節鏡下治療創傷復發性Bankart損傷療效分析
李彥林 王國梁 何川 李建 鄭家禮 陳廣超 李松 余洋
目的探討肩關節鏡下Bankart損傷重建術治療復發性肩關節前脫位的臨床療效。方法自2010年6月至2014年4月隨訪60例應用肩關節鏡下Bankart損傷重建術治療的復發性肩關節前脫位患者,隨訪10~38個月,平均26.6個月;年齡15~45歲,平均29歲。60例患者均為前方單方向性不穩定,術前平均脫位次數為6.5次(2~17次)。手術中采用縫合錨進行Bankart損傷重建術。隨訪時采用ASES評分和Constant-Murley評分進行功能評估。結果60例患者手術前及終末隨訪時ASES平均評分為(83.5±3.2)分與(97.1±2.1)分(t=4.79,P>0.01),肩關節平均前屈上舉角度為(163.8±6.0)°與(185.4±3.9)°(t=4.87,P>0.01),外展角度為(90±1.1)°與(135.4±9.9)°(t=6.40,P>0.01),外旋角度為(57.6±4.3)°與(86.5±5.2)°(t=5.43,P>0.01);術前及終末隨訪時Constant-Murley平均評分為(77.6±3.5)分與(97.2±3.2)分(t=5.06,P>0.01)。終末隨訪時所有病例均未發生術后再脫位,術后殘存恐懼試驗陽性4例(6.7%)。所有患者均恢復術前工作,52例(86.7%)恢復到第一次脫位前的運動水平。結論肩關節鏡下微創行Bankart損傷重建手術是治療復發性肩關節前脫位的有效方法之一,術前病例選擇、術中關節鏡下操作技術及術后功能康復鍛煉是手術成功的關鍵。
肩關節脫位;關節鏡;Bankart損傷
復發性肩關節脫位(或創傷性肩關節不穩)始于第一次肩關節脫位,該脫位損傷了穩定肩關節的韌帶。當盂唇從關節盂上撕裂時,這些韌帶的穩定作用就不復存在,創傷性肩關節不穩定的發展與盂緣和周圍韌帶損傷的類型和程度密不可分。Bankart損傷是發生肩關節復發性前脫位最常見的原因,修復和重建肩關節前方的穩定結構,是治療復發性肩關節前脫位的關鍵。隨著關節鏡技術的發展和普及,肩關節鏡下微創治療復發性肩關節前脫位已被越來越多的醫師采用。2010年6月至2014年4月,我們于關節鏡下采用金屬縫合錨內固定修復Bankart損傷治療60例復發性肩關節前脫位患者,取得良好臨床療效,現報道如下:
資料與方法
一、一般資料
我院自2010年6月至2014年4月,在肩關節鏡下行Bankart損傷重建術治療60例復發性肩關節前脫位患者。隨訪10~38個月,平均26.6個月。年齡15~45歲,平均29歲。60例患者均為前方單方向性不穩定,術前平均脫位次數為6.5次(2~17次)。術后肩關節功能恢復時間為6周,均未發生再脫位。本組患者均除外肩袖全層撕裂、肩峰撞擊征等。
二、影像學檢查
術前均拍攝肩關節正位、側位及肩關節岡上肌出口位X線片(圖1~3),CT掃描、MRI及肩關節去除肱骨頭后CT三維重建(圖4),術前X線片均未見肩關節明顯的骨折,CT三維重建未見明確的骨性Bankart損傷,所有MRI均表現為前側盂唇與關節盂緣之間有高信號,其中3例盂唇消失(圖4,5)。

圖1 肩關節正位片,未見異常
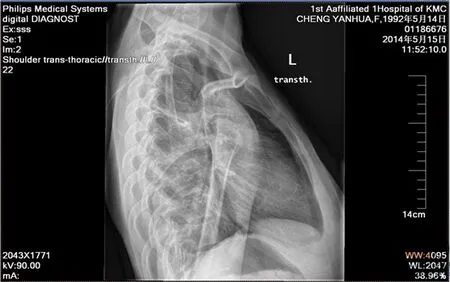
圖2 肩關節側位片,無異常
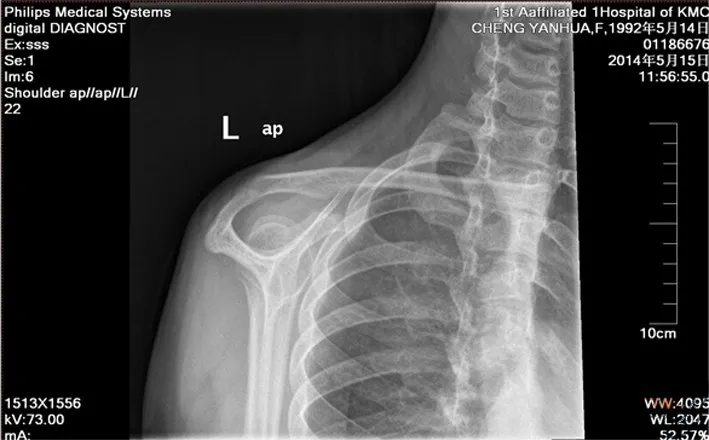
圖3 肩關節岡上肌出口位片,為正常肩峰結構
三、手術方法
全身麻醉,側臥位,沖洗用的生理鹽水每3 000 ml加0.1%腎上腺素1 ml,可調式水泵的壓力維持在60 mm Hg。術前標記肩關節骨性標記及手術入口。后方入口/關節鏡入口:位于肩峰后角向下約2 cm,向內側約1 cm。前上方入口:在喙突外側,關節內位于肱二頭肌長頭腱和肩胛下肌腱上緣之間。前下方入口:在前上方入口下2~3 cm處,關節內盡可能接近肩胛下肌腱上緣。前方兩入口安裝工作套管,作為器械操作通道。于后方入口進入關節鏡,按順序進行肩關節探查,本組所有病例均可見盂唇-肩關節囊-韌帶復合體與盂唇分離、移位(圖6),前關節囊和韌帶組織松弛。損傷部位多位于肩盂1~5點鐘的范圍。7例伴有肱骨頭軟骨損傷,5例伴有盂肱關節軟骨退變。采用低溫等離子射頻消融和刨刀行關節軟骨損傷和退變處表面清理。
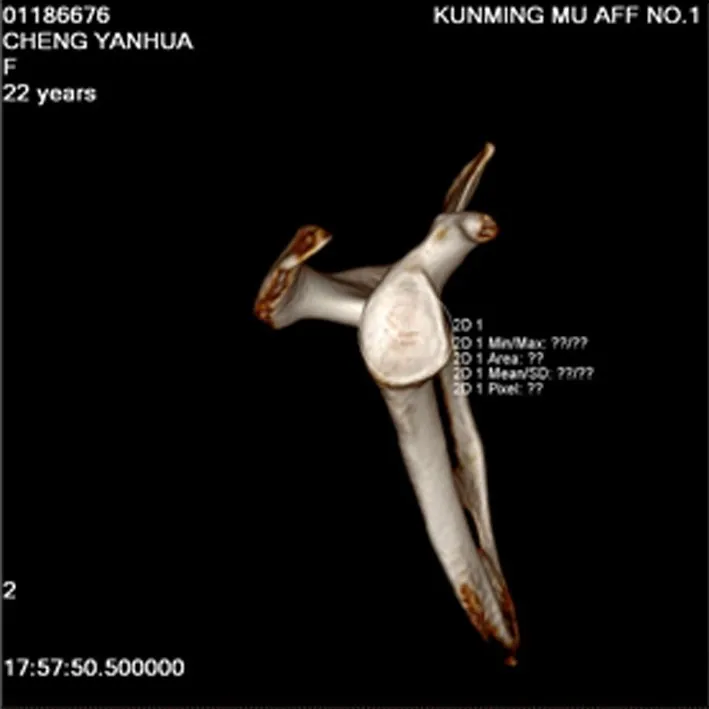
圖4 肩關節去除肱骨頭后CT三維重建,盂唇無骨缺損

圖5 MRI表現為前側盂唇與關節盂緣之間有高信號
使用肩關節軟組織剝離器在肩盂受損處前部,向肩胛頸方向剝離黏連的盂唇-肩關節囊-韌帶復合體。用肩盂銼銼去肩唇受損處纖維組織,露出新鮮骨面。通過前下方入口工作套管,將定位器置于肩盂緣2、3、4、5點鐘位置。于關節盂成45°角,骨錘叩擊定位器,使其在肩盂緣新鮮骨面上形成一個導向孔。移去內芯,金屬縫合錨插入定位器中央并擰入至肩盂內,以穿刺縫合器穿刺縫合盂唇-肩關節囊-韌帶復合體,進行打結收緊完成固定。固定完成后以探鉤再次檢查修復效果,用射頻消融刀清理創緣(圖7)。

圖6 關節鏡下可見Bankart損傷,盂唇-肩關節囊-韌帶復合體與盂唇分離
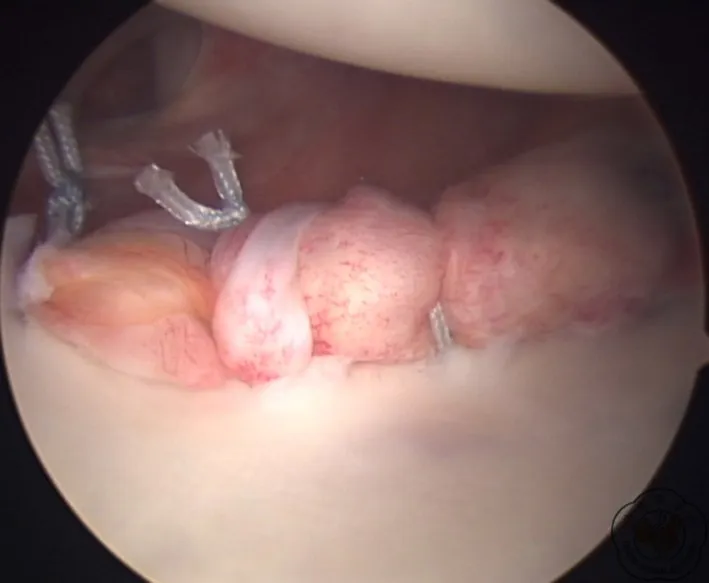
圖7 Bankart損傷重建術后可見分離盂唇已縫合至原位
四、術后處理
術后復查肩關節正側位片(圖8,9),術后采用肩關節外展位支具固定6周,6周內禁止做主動活動。囑患者活動肘、腕及手,并進行局部理療、消腫止痛及冰敷治療。6周后進行保護性康復訓練,包括鐘擺訓練,滑輪器訓練。3個月后進行肌力強度康復訓練,包括增加關節活動度范圍和肌肉的抗阻力訓練,耐力訓練。6個月后進行運動功能康復訓練,加強肩關節周圍肌肉鍛煉,本體感覺鍛煉等,并可進行非對抗性體育活動,包括恢復運動訓練功能的專項訓練,負重上舉、啞鈴訓練等。術后即刻在康復醫師和治療師的指導下進行術后早期物理治療和康復訓練。物理治療主要包括早期冷療減輕疼痛和腫脹,超短波治療改善局部血液循環,促進腫痛消退和組織愈合,康復訓練可改善循環,促進關節囊-盂唇復合體的愈合,加強肌力,增加關節的穩定性,防止關節僵直、腫脹等并發癥。
表1 肩關節復發性脫位手術前、后肩關節功能比較(±s)

表1 肩關節復發性脫位手術前、后肩關節功能比較(±s)
組別 ASES評分 肩關節前屈(°) 肩關節外展(°) 肩關節外旋(°) Constant-Murley.5術后 97.1±2.1 185.4±3.9 135.4±9.9 86.5±5.2 97.2±3.2t值評分術前 83.5±3.2 163.8±6.0 90.0±1.1 57.6±4.3 77.6±3 4.79 4.87 6.40 5.43 5.06P值 <0.01 <0.01 <0.01 <0.01 <0.01
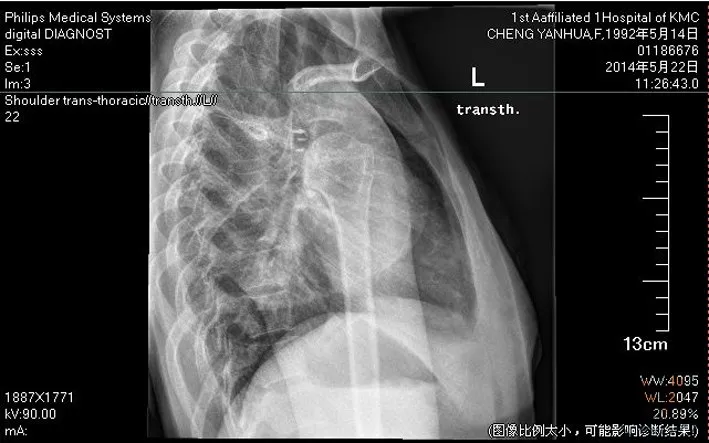
圖8 術后肩關節正位片,錨釘位置良好

圖9 術后肩關節側位片,錨釘位置良好
結 果
術后3周、6周、3個月、6個月及1年門診隨訪,此后每年隨訪一次,60例患者手術前及終末隨訪時進行ASES平均評分,肩關節前屈上舉、外展、外旋角度及終末隨訪時平均Constant-Murley評分采用配對t檢驗處理,P<0.05差異有統計學意義,見表1。終末隨訪時所有病例均未發生術后再脫位,術后殘存恐懼試驗陽性4例(6.7%)。
討 論
肩關節由關節盂和肱骨頭以及周圍的肩關節囊和韌帶組成,正常情況下肱骨頭在關節盂內,當外傷造成肱骨頭脫出關節盂即為肩關節脫位,根據肱骨頭脫位的方向分為肩關節前脫位和后脫位。常見的是肩關節前脫位,致傷原因有跌倒壓在外展并強力被迫過頂的手臂上、肩部的直接擊打、手臂強力被迫外旋;肩關節向后脫位不常見,常常與癲癇發作或電擊有關,此時肩部的肌肉強力收縮造成脫位。Bankart損傷是肩關節盂唇前下方在前下盂肱韌帶復合體附著處的撕脫性損傷,因肩關節前脫位引起,是造成習慣性前方不穩定和脫位的基本損傷。Bankart損傷經常伴隨發生關節囊的異常,超過30%的患者會有前下盂肱韌帶復合體的延長及松弛。經典的Bankart損傷為纖維性Bankart損傷:即關節囊破裂,盂肱韌帶連同附著的關節盂唇從關節盂上撕脫,肩關節前脫位時最常見的是下盂肱韌帶-盂唇復合體損傷,占創傷性肩關節前脫位的85%。治療因患者首次脫位時的年齡而異,當患者首次脫位時年齡<30歲,再次脫位的可能性>80%,建議手術治療,修補撕裂的韌帶及盂唇;但如果患者首次脫位時年齡>30歲,再次脫位的可能性就大為減少,可以先行保守治療[1-2]。本組患者均有明確的外傷史,傷后首診均為手足牽引復位關節,復位后未得到充分的制動固定,盂唇-肩關節囊-韌帶復合體未能愈合,這樣易致復發性脫位。
關節鏡輔助下治療復發性肩關節脫位已經成為治療肩關節疾病的一種不可或缺的治療手段,Bankart損傷采用關節鏡手術的理想患者是從事非接觸性運動伴有Bankart病變,而且其盂唇本身沒有變性,肩關節盂肱下韌帶及盂肱中韌帶質量良好者[3]。許多研究[4-7]報道,關節鏡下治療Bankart損傷修復肩關節前方不穩的效果優于切開手術。
本組采用的金屬帶線錨釘在松質骨中具有多點固定和高穩定性,其釘尾帶有縫針的不可吸收縫線,適合腱骨結合處韌帶肌腱的固定,操作簡便,效果可靠,安全有效,對韌帶肌腱的修復與重建提供了極大的方便[8]。金屬骨錨具有以下優勢:(1)操作簡便,只需暴露骨面,能簡便地完成肌腱與骨的接觸固定,手術時間短,固定牢固;(2)手術創傷小,手術剝離范圍小,軟組織損傷輕;(3)避免了對骨骼進行過多操作所帶來的骨骼畸形而影響生長發育的并發癥;(4)Press-fit固定方式使其在皮質骨下固定牢靠,預置的Ethibond縫線在軟組織愈合期間能保持長時間拉力,使肌腱修復后強度良好,且與骨質連結緊密,適宜于術后早期開展功能鍛煉,防止關節僵硬;(5)由于骨錨固定牢靠,手術后關節內固定時間由6周減少到3~4周,適宜于早期進行功能鍛煉,減少關節僵硬的機會;(6)骨錨為永久置入物,若無骨錨松動退出,影響關節活動、壓迫皮膚或出現無法控制的傷口感染,一般無需取出,避免二次手術的痛苦[9-10]。
本組病例術后均獲隨訪,平均隨訪時間為26.6個月,均未發現再脫位現象。通過分析本組病例手術前、后肩關節的功能,術后肩關節平均前屈上舉角度明顯提高,平均外展90°外旋明顯增加,Gonstant-Murley評分明顯增多。本組病例有4例術后殘存恐懼試驗陽性,考慮患者盂唇-肩關節囊-韌帶復合體與盂唇分離較大,術中難以完全復位及患者不適當的運動有關。因此,關節鏡下行Bankart重建手術能恢復復發性前脫位肩關節的穩定性,術后肩關節的功能得到明顯改善,取得較好的療效,鏡下實施Bankart重建手術,可改善預后,促進肩關節功能恢復,加速康復進程,值得臨床推廣。鑒于本研究病例樣本量相對較少,隨訪時間較短,遠期效果還有待臨床進一步觀察。
[1] 龔熹,崔國慶,王健全,等.復發性肩關節前脫位的臨床病理表現[J].中華骨科雜志,2006,26(6):399-403.
[2] Owens BD,Nelson BJ,Duffey ML,et al.Pathoanatomy of first-time,traumatic,anterior glenohumeral subluxation events[J].J Bone Joint Surg Am,2010,92(7):1605-1611.
[3] Miniaci A,Codsi MJ.Thermal capsulorrhaphy for the treatment of 273 shoulder instability[J].Am J Sports Med,2006,34(8):1356-1363.
[4] Rook RT,Savoie FH 3rd,field LD.Arthroscopic treatment of instability attributable to capsular injury or laxity[J].Clin Orthop Relat Res,2001(390):52-58.
[5] Kartus J,Kartus C,Povacz P,et al.Unbiased evaluation of the arthroscopic extra-articular technique for Bankart repair:a clinical and radiographic study with a 2-to 5-year follow-up[J].Knee Surg Sports Traumatol Arthrosc,2001,9(2):109-115.
[6] Arce G,Arcuri F,Ferro D,et al.Is selective arthroscopic revision beneficial for treating recurrent anterior shoulder instability?[J].Clin Orthop Relat Res,2012,470(4):965-971.
[7] Zaffagnini S,Marcheggiani Muccioli GM,Giordano G,et al.Long-term outcomes after repair of recurrent post-traumatic anterior shoulder instability:comparison of arthroscopic transglenoid suture and open Bankart Reconstruction[J].Knee Surg Sports Traumatol Arthrosc,2012,20(5):816-821.
[8] 涂明中,陳立,曹博,等.關節鏡下GⅡ錨釘固定治療肩關節Bankart損傷[J].臨床骨科雜志,2011,14(1):47-48.
[9] Tokish JM,Mcbratney CM,Solomon DJ,et al.Arthroscopic repair of circumferential lesions of the glenoid labrum:surgical technique[J].J Bone Joint Surg Am,2010,92(Suppl 1 Pt 2):130-144.
[10] Ozorak M,Kokavec M,Svec A.Arthroscopic management of anterior instability of the shoulder[J].Ortop Traumatol Rehabil,2014,16(2):111-118.
Clinical curative effect of the arthroscopic reconstruction for recurrent anterior dislocation of the shoulder
Li Yanlin,Wang Guoliang,He Chuan,Li Jian,Zheng Jiali,Chen Guangchao,Li Song,Yu Yang.Department of Sports Medicine,the First Affiliated Hospital of Kunming Medical University,Kunming 650032,China
BackgroundRecurrent dislocation of shoulder joint(or traumatic shoulder instability)initiates from the first shoulder dislocation,compromising the ligaments for stability of the shoulder.When the labrum is torn from the glenoid,the stable function of these ligaments is lost.The progression of traumatic shoulder instability and the type and degree of injuries in glenoid labrum and surrounding ligaments are inextricably linked.Bankart injury is the most common cause of recurrent anterior shoulder dislocation,and the rehabilitation and reconstruction of stable structure in anterior shoulder is critical for the treatment of recurrent anterior dislocation of the shoulder joint.With the development and popularization of the arthroscopic technique,shoulder arthroscopic surgery in the treatment of recurrent anterior dislocation of the shoulder joint has been adopted by increasing surgeons.From June 2010 to April 2014,60 patients of recurrent anterior shoulder dislocation were treated arthroscopically with metallic suture anchor Bankart repair to explore its clinical efficacy.MethodsClinical data:From June of 2010 to April of 2014,sixty patients in our hospital were treated with arthroscopic reconstruction for Bankart injury of recurrent anterior dislocation of the shoulder.The patients were followed up for 10~38 months and the mean time was 26.6 months.Their agesranged from 15 to 45 years with an average of 29 years.Each of 60 cases had a unidirectional instability of anterior shoulder,and the average number of dislocation before surgery was 6.5 times(2-17 times).Suture anchor was applied for reconstruction of Bankart injury.ASES score and Constant-Murley score were adopted for the functional assessment during follow-ups.The postoperative recovery time of shoulder function was 6 weeks without redislocation in each case.Complete rotator cuff tear,subacromial impingement syndrome,etc.were excluded from this group of patients.Imaging examination:X-ray films of anteroposterior view,lateral view and supraspinatus outlet view,CT scanning,MRI and CT three-dimensional reconstruction with humeral head removed were done preoperatively.No obvious bone defect was shown on preoperative X-ray films,no definite bony Bankart injury was revealed on CT three-dimensional reconstruction,and all MRI showed hyperintense between anterior labrum and glenoid rim with 3 cases of glenoid labrum disappeared.Operative methods:After successful general anesthesia,the patient was placed in lateral position.Every 3000 ml saline for flushing purpose was added with 1 ml of 0.1%epinephrine,and the pressure of adjustable water pump was maintained at 60 mm Hg.The bony markers and surgical portals were marked before operation.Posterior portal/arthroscopic portal:2 cm below the posterior corner of acromion.Anterosuperior portal:in the lateral side of coracoid process and between the long head of the biceps tendon and upper margin of the subscapularis tendon inside the joint.Antroinferior portal:2~3 cm below the anterosuperior portal and close to the upper margin of the subscapularis tendon inside the joint as much as possible.Two arthroscopic working cannulas were positioned as working channels.The arthroscopy was put in through the posterior portal to explore the shoulder joint in order.The labrum-shoulder joint capsule-ligament complex was found detached and shifted from the glenoid labrum and the anterior joint capsule and ligaments were aneuros in all cases of this group.The injury sites were often located in the range of 1~5 o′clock.7 patients were with articular cartilage lesion of humeral head and 5 patients were with glenohumeral cartilage degeneration.Radiofrequency ablation and cartilage-plasty were adopted for surface cleaning of articular cartilage injury and degeneration.The shoulder joint soft tissue detacher was used in the front of the damaged glenoid to dissect the adhesive labrum-shoulder joint capsule-ligament complex to the direction of scapular neck.The fibrous tissue was rasped off at the damage of labrum with glenoid file,exposing the fresh bone.The locator was put at the glenoid rim of 2,3,4,5 o′clock position through the antroinferior working cannula.Employed the bone mallet to percuss the locator with in an angle of 45°with glenoid to make a pilot hole on the fresh bony surface of glenoid.The inner core was removed and the metal suture anchor was put in the center of locator and screwed in the glenoid.The labrum-shoulder joint capsule-ligament complex was sutured with suture penetrator device with the knot tied to complete the fixation.After finishing the fixation,the repair effect was rechecked with probe and the wound margin was cleaned by radiofrequency ablation.Postoperative management:Postoperative examination of shoulder joint includes radiographs,and the shoulder joint is fixed with abduction orthosis for 6 weeks with active movement prohibited.The patient is advised to exercise elbow,wrist and hand,and be given local physical therapy,pain relief and icing.Protective rehabilitation,including pendulum training and pulley device training,is allowed 6 weeks later.Rehabilitation for muscle strength begins 3 months later,consisting of increased joint range of motion,resistance training of muscle and endurance training.After 6 months motor function recovery is initiated to strengthen the exercises of muscles around the shoulder joint,proprioception,etc.,and non-contact sports activities can be engaged,including special training of restoration movement function,weight lifting,dumbbell training,etc.Immediate postoperative physical therapy and rehabilitation is performed under the guidance of rehabilitation physicians and therapists.Physical therapy mainly contains early cold compress to relieve pain and disperse swelling,ultrashort wave therapy to improve local blood circulation and promotion of soreness subsiding and tissue healing.Rehabilitation can improve circulation,promote joint capsule-labrum complex healing,strengthen muscle,increase joint stability,and prevent joint stiffness,swelling and other complications.ResultsOutpatient follow-upswere carried out 3 week,6 week,3 month,6 month and 1 year after operation and henceforth once each year.The mean ASES score before operation and at the final follow-ups,the angle of anteflexion,abduction and external rotation,and the mean Constant-Murley score at the final followups of 60 patients were processed by paired t-test and a value ofP<0.05 was considered statistically significant.No postoperative redislocation occurred in all patients during the final follow-up.Postoperative residual Crank test was positive in 4 patients(6.7%).All patients restored preoperative work with 52 patients(86.7%)restored to the sports level before the first dislocation.DiscussionArthroscopic Bankart repair is one of the effective methods for treatment of recurrent anterior dislocation of the shoulder,the proper case selection,and arthroscopic technique during operation and strict postoperative functional rehabilitation are the keys to successful operation.
Shoulder dislocation;Arthroscopy;Bankart Injury
Wang Guoliang,Email:200301144@163.com
2014-08-07)
(本文編輯:李靜)
10.3877/cma.j.issn.2095-5790.2014.04.003
云南省醫學學科帶頭人項目(D-201207);云南省創新團隊項目(2014HC018)
650032 昆明醫科大學第一附屬醫院運動醫學科
王國梁,Email:200301144@163.com
李彥林,王國梁,何川,等.關節鏡下治療創傷復發性Bankart損傷療效分析[J/CD].中華肩肘外科電子雜志,2014,2(4):219-224.
猜你喜歡
環球時報(2022-12-23)2022-12-23 09:28:37
昆明醫科大學學報(2022年1期)2022-02-28 07:45:04
中老年保健(2021年11期)2021-08-22 03:13:36
昆明醫科大學學報(2021年2期)2021-03-29 07:42:46
河北畫報(2020年10期)2020-11-26 07:20:50
小學閱讀指南·低年級版(2017年1期)2017-03-13 20:07:35
中國衛生標準管理(2015年3期)2016-01-14 03:41:47
中國醫療美容(2015年1期)2015-07-12 10:06:38
鄭州大學學報(醫學版)(2015年2期)2015-02-27 14:50:54
西南軍醫(2014年5期)2014-04-25 07:42:48