血漿脂蛋白相關性磷脂酶A2水平與脈搏波傳導速度相關性臨床研究
2014-08-22 11:18:40楊成林鄭忠愛雷黎明梁錦軍
新醫(yī)學 2014年10期
楊成林 鄭忠愛 雷黎明 梁錦軍
近年來,大量基礎研究證實血漿脂蛋白相關性磷脂酶A2(Lp-PLA2)是致動脈粥樣硬化的主要危險因素之一[1-3]。部分臨床研究結(jié)果也提示,血漿Lp-PLA2水平的升高與冠心病患者預后具有明顯的相關性,但降低血漿Lp-PLA2水平是否能夠減少心腦血管疾病發(fā)生率目前尚未完全明確[4-7]。脈搏波傳導速度(PWV)是指脈搏波由動脈的一特定位置沿管壁傳播至另一特定的位置的速率。這是一個用來反映動脈彈性及可擴張的非侵入性指標,PWV值越高表明血管壁越硬。為探討血漿Lp-PLA2水平與早期大動脈彈性的相關性,本研究擬采用橫斷面的方法,評估血漿Lp-PLA2水平與PWV,現(xiàn)將結(jié)果報道如下。
對象與方法
一、研究對象
收集2012年1月至2012年12月在湖北省人民醫(yī)院就診患者122例,以及2013年1月至2013年7月在我院就診患者46例,共168例非心腦血管疾病患者。排除標準:既往有心腦血管動脈粥樣硬化性疾病(主要為心肌梗死、腦卒中和外周動脈粥樣硬化疾病);合并其他嚴重肝腎衰竭疾病患者以及合并嚴重感染和腫瘤患者。
二、研究方法
采集清晨空腹靜脈血10 ml,以1 000×g離心10 min后分離血漿,置于-80℃冰箱保存。血漿Lp-PLA2水平檢測采用ELISA,試劑盒購于武漢新啟迪生物科技有限公司(嚴格按照試劑盒說明書進行相關操作,每份標本重復檢測3次,取平均值)。PWV檢測采用法國Artech-Medical 公司生產(chǎn)的康普樂(Compli OR SP)儀器進行檢測。空腹血糖、糖化血紅蛋白、膽固醇水平、腎功能等指標送實驗室(采用全自動生化分析儀,日本奧林巴斯AU2700)進行檢測,同時收集所有入選者血壓、心率、吸煙情況、BMI以及心腦血管疾病家庭史等情況。
三、統(tǒng)計學處理

結(jié) 果
一、 血漿Lp-PLA2正常組和升高組一般資料比較
依據(jù)血漿Lp-PLA2水平,按照既往文獻[8]報道,將所有入選者分為正常組(< 235 ng/ml)和升高組(≥ 235 ng/ml),對兩組人群一般資料進行比較,由表1可見,兩組人群除了PWV及血漿Lp-PLA2水平差別存在統(tǒng)計學意義,其余各指標無明顯差別。

表1 血漿Lp-PLA2正常組和升高組一般資料比較
二、多重線性回歸分析
采用多重線性回歸分析各變量對PWV的預測價值,由表2可見,年齡、高血壓以及血漿Lp-PLA2水平均與PWV獨立相關,是PWV的獨立危險因素,其他傳統(tǒng)危險因素如吸煙、血糖以及膽固醇等與PWV無獨立相關性。
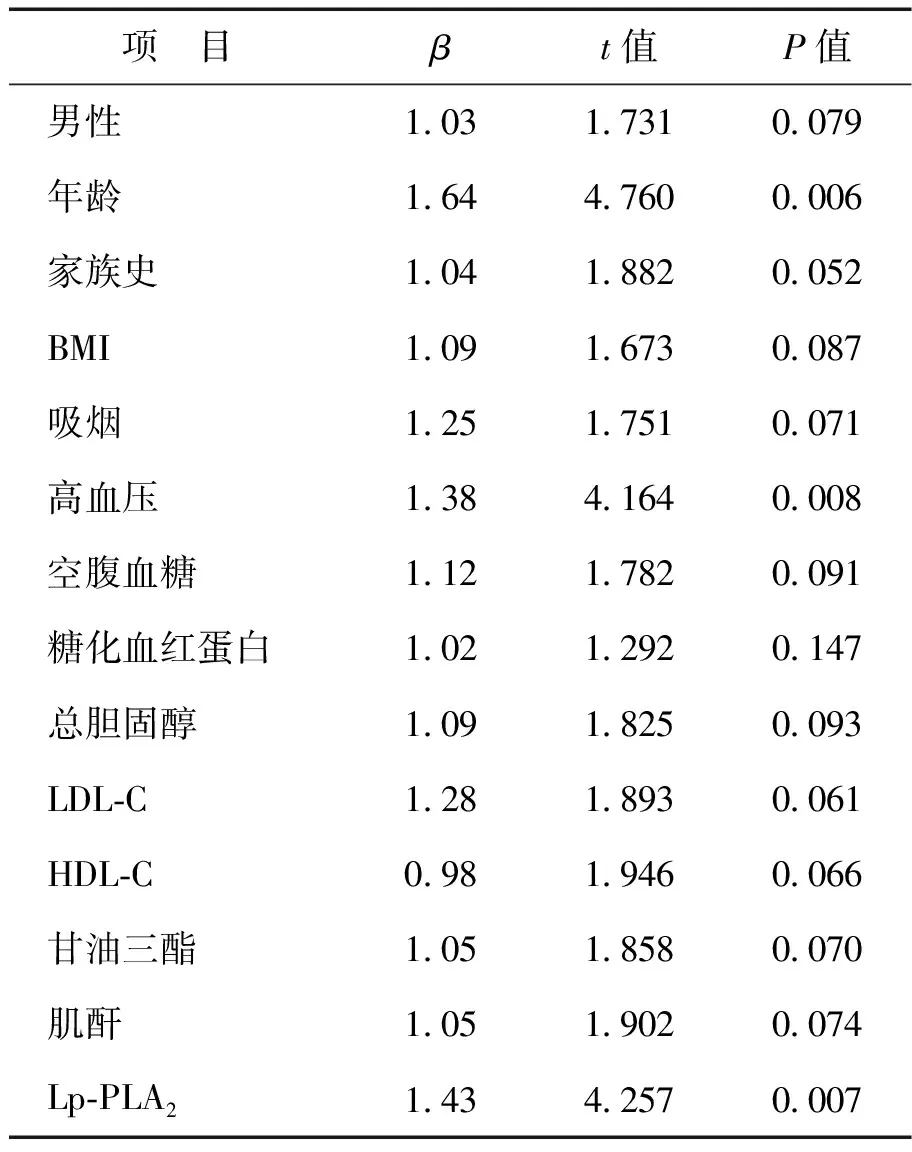
表2 各變量與PWV多重線性回歸分析
討 論
業(yè)已證實,大動脈彈性的下降是早期動脈粥樣硬化的主要表現(xiàn)之一,目前臨床多采用PWV對大動脈彈性進行評估[8]。既往大量研究結(jié)果表明,在存在冠心病、腦梗塞以及外周動脈粥樣硬化性疾病患者,其大動脈彈性明顯下降,主要表現(xiàn)為PWV的明顯升高[9]。與此同時,PWV的明顯升高與冠狀動脈粥樣硬化程度也具有一定的相關性。因此,對于存在動脈粥樣硬化危險因素如吸煙、高血壓、高脂血癥以及糖尿病等患者,采用PWV評估大動脈彈性情況有助于對動脈粥樣硬化的綜合分析。
Lp-PLA2是近年來廣泛推廣的動脈粥樣硬化生化標志物[10]。Lp-PLA2主要有粥樣斑塊中巨噬細胞所分泌的酶類物質(zhì),能夠?qū)е聝?nèi)皮細胞功能的下降、血管痙攣、脂質(zhì)壞死和增加以及粥樣斑塊纖維膜的變薄[10-11]。近十幾年來,大量研究已充分證實血漿Lp-PLA2水平的升高與動脈粥樣硬化間的相關性[12]。然而,血漿Lp-PLA2水平升高是否是大動脈彈性下降的獨立危險因素目前尚未明確。
本研究結(jié)果提示,在血漿Lp-PLA2升高組患者,其PWV值也明顯升高,提示血漿Lp-PLA2水平與大動脈彈性具有一定的相關性,多重線性回歸分析也提示血漿Lp-PLA2水平升高是大動脈彈性下降的獨立危險因素。結(jié)合既往文獻報道,我們認為,血漿Lp-PLA2水平升高可能通過如下作用機制導致大動脈彈性的下降:①血漿Lp-PLA2水平升高將會導致血管內(nèi)皮細胞功能的異常,從而導致血管痙攣以及收縮/舒張功能下降,進而影響血管彈性;②血漿Lp-PLA2水平升高將導致平滑肌細胞的增殖以及遷移,從而導致血管管腔的狹窄,進而影響管腔內(nèi)血流動力學情況;③血漿Lp-PLA2水平升高還可能通過其他信號通路影響動脈中層彈力纖維膜[13-15]。因此,血漿Lp-PLA2可通過上述途徑在動脈粥樣硬化早期影響大動脈彈性。同時本研究結(jié)果還提示年齡和高血壓也與大動脈彈性具有獨立相關性。
綜上所述,在動脈粥樣硬化早期,血漿Lp-PLA2水平升高與PWV具有獨立相關性,對于血漿Lp-PLA2水平升高且具有動脈粥樣硬化高危因素患者,進行嚴格隨訪,定期評估PWV可能可以降低心腦血管事件發(fā)生率。
[1] Packard CJ.Lipoprotein-associated phospholipase A2as a biomarker of coronary heart disease and a therapeutic target. Curr Opin Cardiol,2009,24:358-363.
[2] Cai A, Zheng D, Qiu R, et al. Lipoprotein-associated phospholipase A2(Lp-PLA(2)): a novel and promising biomarker for cardiovascular risks assessment. Dis Markers,2013,34:323-331.
[3] Ridker PM, MacFadyen JG, Wolfert RL, et al. Relationship of lipoprotein-associated phospholipase A2mass and activity with incident vascular events among primary prevention patients allocated to placebo or to statin therapy: an analysis from the JUPITER trial. Clin Chem,2012,58:877-886.
[4] Gon?alves I, Edsfeldt A, Ko NY, et al. Evidence supporting a key role of Lp-PLA2-generated lysophosphatidylcholine in human atherosclerotic plaque inflammation. Arterioscler Thromb Vasc Biol,2012,32:1505-1512.
[5] Ryu SK, Hutten BA, Vissers MN, et al. Lipoprotein-associated phospholipase A2mass and activity in children with heterozygous familial hypercholesterolemia and unaffected siblings: effect of pravastatin. J Clin Lipidol,2011,5:50-56.
[6] Berger JS, Ballantyne CM, Davidson MH, et al. Peripheral artery disease, biomarkers, and darapladib. Am Heart J,2011,161:972-978.
[7] Dohi T, Miyauchi K, Okazaki S, et al. Decreased circulating lipoprotein-associated phospholipase A2 levels are associated with coronary plaque regression in patients with acute coronary syndrome. Atherosclerosis,2011,219:907-912.
[8] Davidson MH, Corson MA, Alberts MJ, et al. Consensus panel recommendation for incorporating lipoprotein-associated phospholipase A2testing intocardiovascular disease risk assessment guidelines. Am J Cardiol,2008,101:51F-57F.
[9] Grundy SM, Cleeman JI, Merz CN, et al. Implications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel IIIguidelines. Circulation,2004,110:227-239.
[10] Ballantyne CM, Nambi V.Markers of inflammation and their clinical significance. Atheroscler Suppl,2005,6:21-29.
[11] 徐如林, 蔡安平, 麥煒頤. 脂蛋白相關性磷脂酶A2:一種新型的、具有前景的評估心血管危險的生化標記物. 新醫(yī)學,2014,45: 211-217.
[12] Zalewski A, Macphee C. Role of lipoprotein-associated phospholipase A2 in atherosclerosis: biology, epidemiology, and possible therapeutic target. Arterioscler Thromb Vasc Biol,2005,25:923-931.
[13] Wang WY, Zhang J, Wu WY, et al. Inhibition of lipoprotein-associated phospholipase A2 ameliorates inflammation and decreases atherosclerotic plaque formation in ApoE-deficient mice. PLoS One,2011,6:e23425.
[14] Liu J, Chen R, Marathe GK, et al. Circulating platelet-activating factor is primarily cleared by transport, not intravascular hydrolysis by lipoprotein-associated phospholipase A2/ PAF acetylhydrolase. Circ Res,2011,108:469-477.
[15] Garg PK, McClelland RL, Jenny NS, et al. Association of lipoprotein-associated phospholipase A(2) and endothelial function in the Multi-Ethnic Study of Atherosclerosis (MESA). Vasc Med,2011,16:247-252.
[16] Casas JP, Ninio E, Panayiotou A, et al. PLA2G7 genotype, lipoprotein-associated phospholipase A2activity, and coronary heart disease risk in 10 494 cases and 15 624 controls of European Ancestry. Circulation,2010,121:2284-2293.
猜你喜歡
現(xiàn)代臨床醫(yī)學(2022年4期)2022-09-29 07:38:00
美與時代·美術學刊(2022年3期)2022-04-27 01:18:15
昆明醫(yī)科大學學報(2021年4期)2021-07-23 01:21:50
火花(2019年12期)2019-12-26 01:00:28
云南醫(yī)藥(2019年3期)2019-07-25 07:25:14
人大建設(2019年12期)2019-05-21 02:55:32
海南醫(yī)學(2016年8期)2016-06-08 05:43:00
學苑創(chuàng)造·A版(2015年11期)2016-01-14 09:03:27
醫(yī)學研究雜志(2015年9期)2015-07-01 17:28:15
鄭州大學學報(理學版)(2014年3期)2014-03-01 04:21:05
